Predictive Value of Hepatitis B Core-Related Antigen for Multiple Recurrence Outcomes After Treatment Cessation in Chronic Hepatitis B: A Meta-Analysis Study
Guoyang Yu, Meiqi Cheng, Yuxin Duan, Minrong Kang, Ning Jiang, Wei Yan, Jianhua Yin

TL;DR
This study shows that a blood test called HBcrAg can reliably predict if chronic hepatitis B patients will relapse after stopping treatment.
Contribution
The study confirms HBcrAg as a robust non-invasive biomarker for predicting relapse in chronic hepatitis B patients after treatment cessation.
Findings
HBcrAg has a pooled sensitivity of 0.81 and specificity of 0.72 for predicting relapse.
Threshold effects were the main source of heterogeneity, resolved after excluding outlier cutoff values.
HBcrAg's predictive value is not affected by age, sex, or detection methods.
Abstract
Background: Hepatitis B core-related antigen (HBcrAg), a novel serum biomarker reflecting the activity of intrahepatic covalently closed circular DNA (cccDNA), has generated conflicting evidence regarding its clinical utility for predicting post-antiviral therapy relapse in chronic hepatitis B (CHB) patients. Methods: We systematically analyzed 13 studies (15 cohorts, n = 1529 patients) from PubMed, Web of Science, Wanfang, and CNKI (through April 2025). A bivariate model evaluated HBcrAg’s predictive performance for relapse outcomes, including virological relapse, clinical relapse, and hepatitis flares. Results: HBcrAg demonstrated a pooled sensitivity of 0.81 (95% CI: 0.75–0.86) and specificity of 0.72 (95% CI: 0.67–0.76) for relapse prediction, with a diagnostic odds ratio of 10.66 (95% CI: 7.36–15.42) and summary AUC of 0.83 (95% CI: 0.80–0.86). Subgroup analysis identified…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
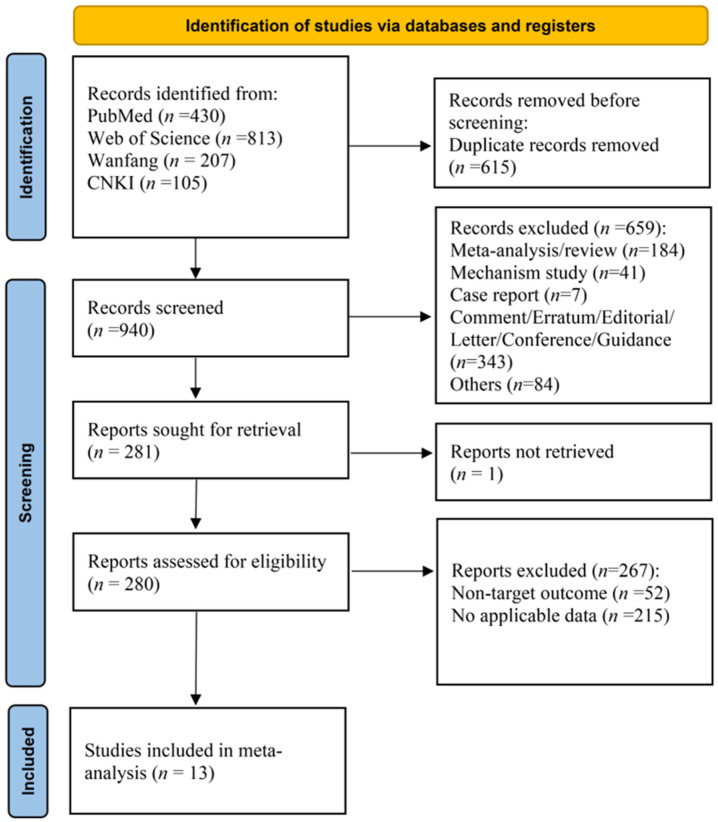 Figure 1
Figure 1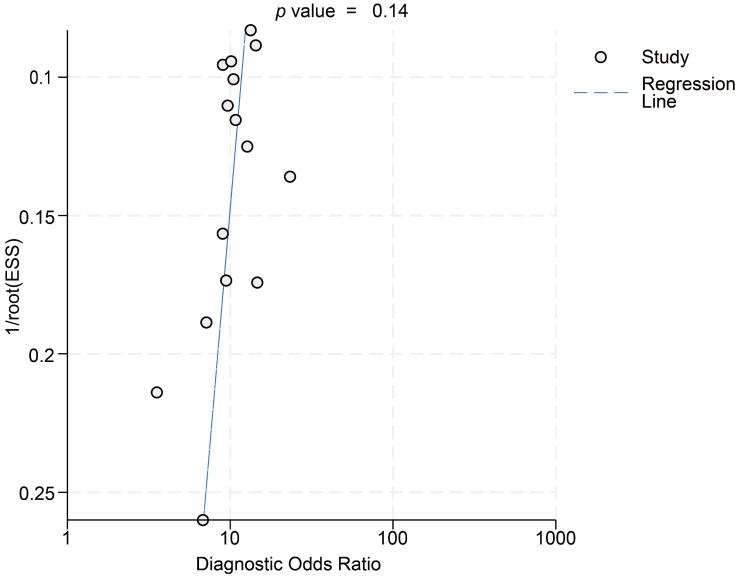 Figure 2
Figure 2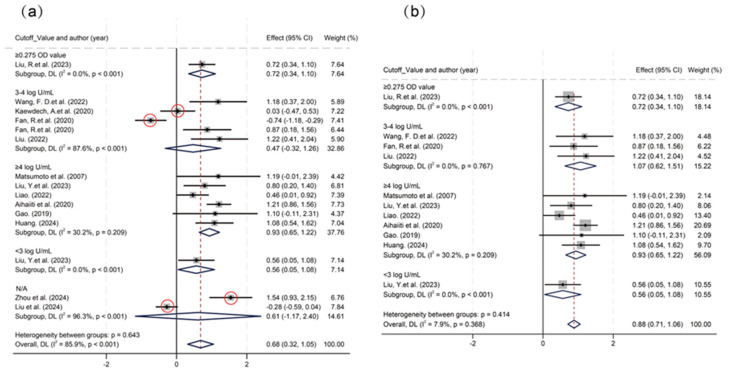 Figure 3
Figure 3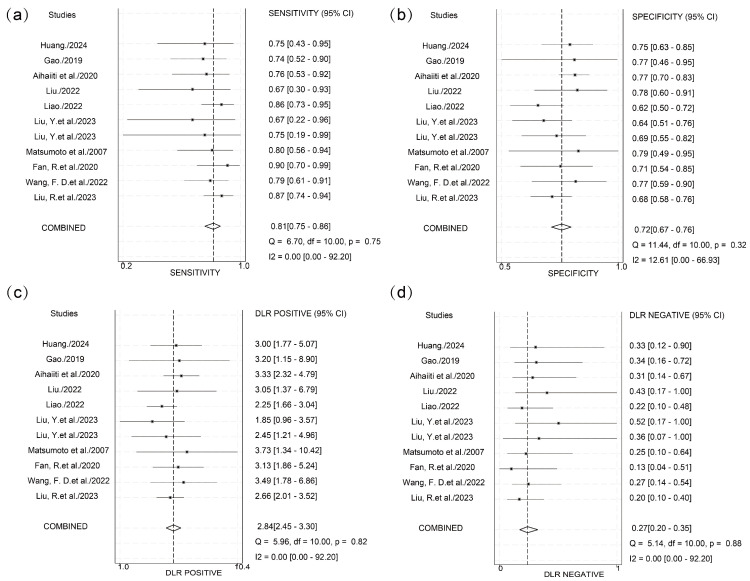 Figure 4
Figure 4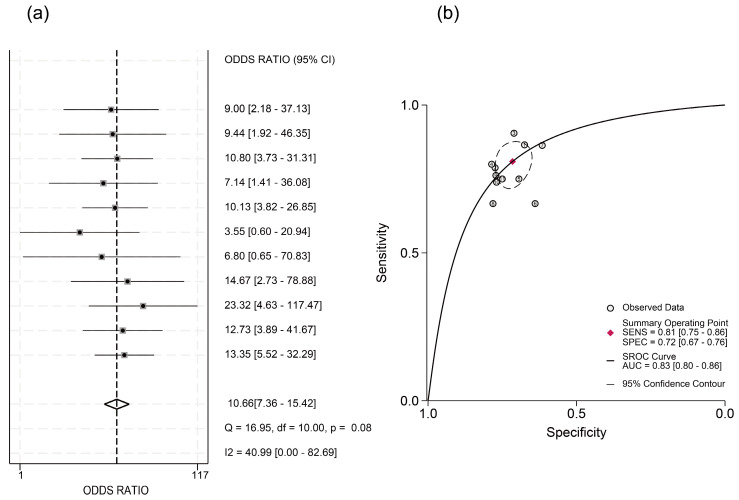 Figure 5
Figure 5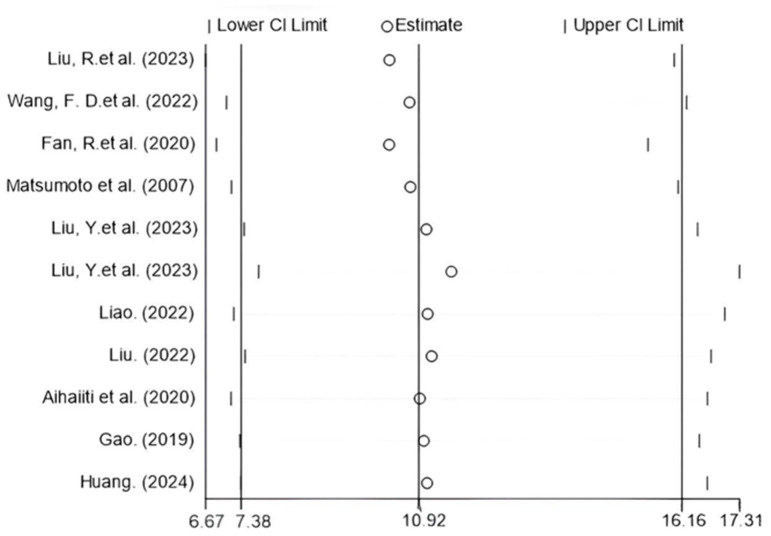 Figure 6
Figure 6- —Program of Shanghai Academic Research Leader
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHepatitis B Virus Studies · Hepatitis C virus research · Liver Disease Diagnosis and Treatment
1. Introduction
According to 2022 data, chronic hepatitis B virus (HBV) infection affects approximately 257 million individuals globally, contributing to over 800,000 annual deaths from complications including cirrhosis and hepatocellular carcinoma (HCC) [1]. Significant diagnostic and therapeutic gaps persist: only 13% of chronic hepatitis B (CHB) patients are diagnosed, and fewer than 3% receive antiviral therapy [2,3,4].
A key barrier to cure is the persistence of covalently closed circular DNA (cccDNA) in hepatocytes. Resisting elimination by current antivirals, cccDNA serves as a molecular reservoir that maintains viral persistence for decades—even after apparent infection resolution. This reservoir can reactivate viral replication, triggering disease relapse following therapy cessation [5,6].
Hepatitis B core-related antigen (HBcrAg) has recently emerged as a serum biomarker strongly correlated with intrahepatic cccDNA activity (r = 0.641, 95% confidence interval [CI]: 0.510–0.743, p < 0.001), outperforming hepatitis B surface antigen (HBsAg) as a virological indicator [5]. Unlike cccDNA quantification requiring invasive liver biopsy, HBcrAg offers a non-invasive surrogate for intrahepatic viral replication [7]. Growing evidence suggests that is has prognostic value for predicting HCC risk and post-treatment recurrence in CHB patients [8], with high sensitivity even at low viral loads (<2000 IU/mL) [9].
Despite these advances, current research focuses predominantly on single recurrence endpoints. No systematic evaluation exists for HBcrAg’s predictive efficacy across multidimensional outcomes (e.g., virological relapse [VR], clinical relapse [CR], hepatitis flares). Existing meta-analyses [10,11,12] remain limited to traditional biomarkers, overlooking HBcrAg’s unique advantages. This meta-analysis comprehensively evaluates HBcrAg’s predictive capacity for diverse recurrence outcomes, providing evidence to optimize individualized treatment cessation strategies and risk-stratified management in high-risk populations.
2. Method
2.1. Search Strategy
To evaluate the clinical utility of HBcrAg, we conducted a comprehensive literature search across four databases: PubMed, Web of Science (WOS), Wanfang, and China National Knowledge Infrastructure (CNKI). The specific search strategies were as follows:
- (1)PubMed: Articles published before 1 April 2025 were retrieved using the search terms “HBcrAg” OR “Hepatitis B core-related Antigen.”
- (2)WOS: Literature indexed between 1 January 1900 and 1 April 2025 was identified using the keywords “hepatitis B core-related antigen” OR “HBcrAg.”
- (3)Wanfang: Journal articles, dissertations, and conference papers published from 1 January 1900 to 7 May 2025 were searched for with the terms “hepatitis B core-related antigen,” “HBcrAg,” or “hepatitis B core-related antigen (in Chinese)”.
- (4)CNKI: All literature from 1 January 1900 to 1 April 2025 was retrieved using the keywords “hepatitis B core-related antigen” OR “HBcrAg” OR “hepatitis B core-related antigen (in Chinese)”.
Following the search, duplicate records were removed, and manual screening was performed to exclude review articles, systematic reviews, practice guidelines, letters, editorials, and non-human studies.
Initial categorization based on study outcomes and designs revealed a substantial number of articles investigating the prognostic value of HBcrAg in post-treatment outcomes in CHB patients. Given the ongoing controversy and divergent findings regarding HBcrAg’s predictive efficacy in clinical outcomes, we focused on studies evaluating HBcrAg as a prognostic biomarker for predicting post-treatment relapse in CHB patients.
2.2. Quality Assessment
In this meta-analysis, the Quality in Prognostic Studies (QUIPS) [13] tool, a validated risk of bias assessment instrument, was employed to ensure the methodological rigor of included studies. The updated QUIPS tool categorizes potential biases in prognostic studies into six domains: study participation, study attrition, prognostic factor measurement, outcome measurement, study confounding, and statistical analysis and reporting. Based on descriptions provided in the original studies, the risk of bias within each domain was classified as high, moderate, or low. The QUIPS tool incorporates detailed signaling questions for each dimension, addressing critical aspects such as comprehensive characterization of the study population, recruitment methodology of participants, and reliability of prognostic factor and outcome measurements. By systematically considering these elements, the tool effectively identifies potential biases arising from study design, implementation, and reporting processes, thereby ensuring the scientific validity and reliability of studies included in the analysis.
2.3. Data Analysis
Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) [14] are critical metrics for evaluating the performance of diagnostic tests. In this study, we extracted reported values of PPV, NPV, sensitivity, and specificity from the included articles. Using these metrics alongside the total sample size and the number of positive outcomes, we back-calculated the values of true positives (TP), false positives (FP), true negatives (TN), and false negatives (FN) based on the following formulas. Sensitivity refers to the proportion of true–positive cases correctly identified among all actual positive cases, calculated as TP/(TP + FN). Specificity represents the proportion of true–negative cases correctly identified among all actual negative cases, calculated as TN/(TN + FP). PPV indicates the proportion of true–positive cases among all samples classified as positive, calculated as TP/(TP + FP). NPV denotes the proportion of true–negative cases among all samples classified as negative, calculated as TN/(TN + FN).
The positive likelihood ratio (PLR) and negative likelihood ratio (NLR) were employed to further assess the diagnostic performance. A higher PLR value signifies a stronger ability of the test to differentiate between diseased and non-diseased populations, whereas a lower NLR value suggests superior performance in excluding the disease.
The diagnostic odds ratio (DOR), calculated as the ratio of true positives multiplied by true negatives to false positives multiplied by false negatives (DOR = [TP × TN]/[FP × FN]), integrates information from both sensitivity and specificity to holistically reflect the accuracy of a diagnostic test. A higher DOR value indicates superior diagnostic performance, underscoring its critical role in evaluating the efficacy of diagnostic methodologies. This metric serves as a robust indicator for quantifying test reliability and discriminatory power in clinical decision-making contexts.
The bivariate model was employed to synthesize effect sizes in atypical meta-analyses [15]. This approach enables simultaneous analysis of sensitivity and specificity while accounting for their intrinsic correlation through joint modeling of their distributions. The model generates a summary receiver operating characteristic (SROC) curve, which graphically plots sensitivity on the y-axis against 1-specificity on the x-axis. This visualization effectively illustrates the distribution of sensitivity–specificity pairs across studies, offering a comprehensive and methodologically rigorous evaluation of diagnostic test performance by integrating multidimensional accuracy metrics into a unified analytical framework.
Furthermore, threshold effects were examined using Spearman’s correlation analysis between sensitivity and 1-specificity. Statistical significance was determined by a p-value threshold of <0.05, with values below this threshold indicating the presence of significant threshold effects. Concurrently, heterogeneity attributable to covariates beyond threshold effects was quantified through the I^2^ statistic, which estimates the proportion of total variation across studies that reflects genuine differences rather than random chance. The I^2^ index was interpreted using established thresholds: values < 25% denote low heterogeneity, 25–50% suggest moderate heterogeneity, and >50% indicate substantial heterogeneity. This dual analytical approach enables systematic differentiation between threshold-induced variability and other sources of study-level heterogeneity, thereby enhancing the interpretative validity of pooled diagnostic accuracy estimates.
Subgroup analysis stratifies study populations according to predefined variables and conducts independent meta-analyses within each stratum, with the objective of investigating between-subgroup heterogeneity in effect magnitudes and identifying potential sources of variability.
Meta-regression extends this approach by modeling study-level effect sizes as dependent variables and incorporating covariates of interest as independent predictors. This regression-based framework quantitatively evaluates the association between explanatory variables and effect estimates, enabling precise quantification of covariate effects on observed heterogeneity. Both methodologies synergistically address the decomposition of variance components in pooled effect estimates, distinguishing clinically meaningful effect modifiers from stochastic variation.
All statistical analyses were conducted using STATA software (version 17.0; StataCorp., College Station, TX, USA) with the MIDAS module for meta-analytical modeling and Review Manager (version 5.3; The Cochrane Collaboration) for systematic review management. This dual-platform approach ensured methodological rigor in both quantitative synthesis (STATA) and evidence organization (RevMan), aligning with best practices for diagnostic accuracy meta-analyses.
3. Results
3.1. Study Selection and Characteristics
Initial database searches identified 1555 potentially relevant records. Following deduplication, 940 unique records underwent manual screening. Exclusion criteria encompassed systematic reviews/meta-analyses, mechanistic investigations (e.g., animal/cell studies, non-patient research), case reports, editorial commentaries, conference guidelines, errata, and other non-qualifying publication types. Subsequent full-text review of 280 articles excluded studies focusing on non-target clinical endpoints (e.g., HCC, hepatic fibrosis, cirrhosis, hepatitis staging) or those with inaccessible outcome data (e.g., missing effect estimates, undocumented treatment histories, or non-predictive analyses). Ultimately, 13 articles met the inclusion criteria for quantitative synthesis.
The study selection process based on PRISMA flow reporting standards is detailed in Figure 1, with study characteristics presented in Table 1. The inclusion and exclusion criteria for the literature are detailed in Table S1.
3.2. Risk of Bias Analysis
Risk of bias assessment for the 13 included articles was conducted using the QUIPS tool. Among the studies evaluating HBcrAg’s predictive capacity for post-treatment relapse in CHB patients, six demonstrated low risk of bias, six moderate risk, and one high risk. Detailed results are presented in Table 2.
3.3. Predictive Efficacy of HBcrAg Across Various Recurrence Outcomes
This meta-analysis incorporated data from 15 cohorts, utilizing effect sizes corresponding to maximal area under the curve (AUC) values reported in individual studies. For predicting all recurrence outcomes, HBcrAg demonstrated a pooled sensitivity of 0.84 (95% CI, 0.77–0.88; I^2^ = 45.8%) and specificity of 0.67 (95% CI, 0.59–0.74; I^2^ = 87.5%). Diagnostic likelihood ratios included a PLR of 2.56 (95% CI, 2.10–3.11; I^2^ = 74.6%) and NLR of 0.24 (95% CI, 0.18–0.32; I^2^ = 0%), with DOR of 10.53 (95% CI, 7.62–14.57; I^2^ = 33.5%). Bivariate modeling revealed substantial heterogeneity (overall I^2^ = 96.44; 95% CI, 93.81–99.06), predominantly driven by specificity heterogeneity (I^2^ = 87.5%) (Figures S1 and S2). Deeks’ funnel plot analysis indicated no significant publication bias (p > 0.05) (Figure 2).
Significant threshold effects were identified via Spearman’s correlation analysis of logit-transformed sensitivity and specificity (ρ = −0.6381, p < 0.05). Subgroup analysis stratified by cutoff value ranges showed significant heterogeneity in the 3–4 log U/mL group (I^2^ = 87.6%) and the N/A group (I^2^ = 96.3%) (Figure 3). Within the 3–4 log U/mL subgroup, studies by Kaewdech et al. and Fan et al. were outliers, showing results contradicting the pooled estimate with significantly non-overlapping 95% CIs. After exclusion of the N/A group and these two outlier studies, threshold effects were eliminated (ρ = −0.1758, p = 0.6218), and heterogeneity was reduced. Pooled analysis demonstrated that HBcrAg achieved a sensitivity of 0.81 (95% CI, 0.75–0.86; I^2^ = 0), specificity of 0.72 (95% CI, 0.67–0.76; I^2^ = 12.61), PLR of 2.8 (95% CI, 2.4–3.3; I^2^ = 0), NLR of 0.27 (95% CI, 0.20–0.35; I^2^ = 0), and DOR of 10.66 (95% CI, 7.36–15.42; I^2^ = 40.99) for predicting recurrence outcomes. The summary AUC was 0.83 (95% CI: 0.80–0.86) (Figure 4 and Figure 5).
Meta-regression analysis of potential confounders (including age, sex, HBeAg positivity rate, HBsAg/HBcrAg levels, publication year, detection timing, and endpoint events) showed no significant impact on HBcrAg’s predictive performance (Tables S2 and S3), suggesting robust diagnostic utility across diverse populations and methodological contexts. Furthermore, sensitivity analysis confirmed result stability with <10% variation in the DOR upon sequential study exclusion (Figure 6).
4. Discussion
Although NAs effectively suppress HBV replication and delay disease progression, most patients require long-term or lifelong therapy. This challenge stems from the persistence of cccDNA in hepatocytes, which serves as a molecular reservoir for viral reactivation. Even patients achieving serological HBV DNA clearance may experience virological rebound and hepatitis recurrence after treatment cessation. Recently, HBcrAg, a novel biomarker reflecting cccDNA activity and viral reservoir dynamics, has gained significant attention. Studies demonstrate strong correlations between HBcrAg and cccDNA (r = 0.70), intrahepatic total HBV DNA (r = 0.67), and serum HBV DNA (r = 0.69) [29]. Furthermore, declining serum HBcrAg levels correlate with increasing HBsAg seroclearance rates over time [30], and HBcrAg reliably reflects persistent viral reservoir activity during long-term NAs therapy. These properties support its theoretical role in predicting post-treatment relapse.
This meta-analysis systematically evaluated HBcrAg’s predictive performance for multidimensional HBV recurrence outcomes (VR, CR, acute hepatitis flares, and HBV reactivation [HBVr]) using data from 13 studies involving 1529 patients. Results revealed excellent predictive value for endpoints including ALT flares, CR, VR, and HBVr, with a pooled AUC of 0.83 (81% sensitivity and 72% specificity). Meta-regression analysis indicated robust clinical generalizability: covariates including age, sex, HBeAg status, HBsAg levels, and study design variations did not significantly affect predictive stability (interaction tests, p > 0.05). Thus, in NA-treated patients meeting current cessation criteria, elevated baseline or EOT serum HBcrAg levels (minimum cutoff: 2.54 log IU/mL in this analysis) may significantly increase relapse risk. This aligns with the Japan Society of Hepatology (JSH) risk stratification strategy, which categorizes HBcrAg levels into three intervals (<3.0 log U/mL, 3.0–4.0 log U/mL, and ≥4.0 log U/mL), assigning relapse risk scores of 0, 1, and 2, respectively. Patients with total scores ≥ 1 exhibit < 50% relapse-free rates and require individualized extended therapy [31].
Current HBV relapse prediction research emphasizes HBsAg, HBV RNA, and HBV DNA. One study found HBsAg significantly inferior to HBcrAg in predicting ALT flares (AUC difference > 0.15, p < 0.01) [32]. Although HBV RNA shows comparable predictive potential [32,33], its reliance on complex nucleic acid amplification techniques (e.g., RT-qPCR) limits utility in primary care. Conversely, HBcrAg detection via routine ELISA or CLEIA offers advantages in simplicity, cost-effectiveness, and standardization, enhancing clinical monitoring feasibility.
This study has several limitations. First, the included studies had relatively high bias risk (six moderate-risk, one high-risk), potentially compromising internal validity. Second, while EOT HBcrAg levels are critical for cessation decisions, insufficient data precluded dedicated analysis of this pivotal timepoint. Third, mild specificity heterogeneity persisted even after excluding four studies with aberrant thresholds; potential sources (e.g., detection methods or viral genotype distribution) remain underexplored. Finally, despite robust statistical predictive performance, HBcrAg alone remains insufficient for clinical decisions. JSH guidelines emphasize comprehensive evaluation including HBV DNA, HBsAg quantification, and histological indicators—though this study did not systematically explore multi-marker models.
5. Conclusions and Perspectives
Although HBcrAg demonstrates robust predictive utility, its standalone application faces inherent limitations. Future research should prioritize multicenter prospective studies employing standardized HBcrAg assays with predefined thresholds. Such studies incorporate diverse patient cohorts spanning viral genotypes, ethnicities, and liver disease stages to improve generalizability. Furthermore, investigating combinatorial strategies integrating HBcrAg with other virological markers (e.g., HBV RNA and intrahepatic cccDNA) to develop multidimensional predictive models is warranted. This integrated approach will establish a refined risk stratification framework essential for guiding evidence-based antiviral treatment cessation decisions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The Polaris Observatory Collaborators Global prevalence, cascade of care, and prophylaxis coverage of hepatitis B in 2022: A modelling study Lancet Gastroenterol. Hepatol.2023887990710.1016/S 2468-1253(23)00197-837517414 · doi ↗ · pubmed ↗
- 2The Polaris Observatory Collaborators Global prevalence, treatment, and prevention of hepatitis B virus infection in 2016: A modelling study Lancet Gastroenterol. Hepatol.2018338340310.1016/S 2468-1253(18)30056-629599078 · doi ↗ · pubmed ↗
- 3Hosaka T. Suzuki F. Kobayashi M. Fujiyama S. Kawamura Y. Sezaki H. Akuta N. Kobayashi M. Suzuki Y. Saitoh S. Ultrasensitive Assay for Hepatitis B Core-Related Antigen Predicts Hepatocellular Carcinoma Incidences During Entecavir Hepatol. Commun.20226364910.1002/hep 4.181934532993 PMC 8710789 · doi ↗ · pubmed ↗
- 4Lin C.L. Kao J.H. Development of hepatocellular carcinoma in treated and untreated patients with chronic hepatitis B virus infection Clin. Mol. Hepatol.20232960562210.3350/cmh.2022.034236788759 PMC 10366811 · doi ↗ · pubmed ↗
- 5Caviglia G.P. Armandi A. Rosso C. Ribaldone D.G. Pellicano R. Fagoonee S. Hepatitis B Core-Related Antigen as Surrogate Biomarker of Intrahepatic Hepatitis B Virus Covalently-Closed-Circular DNA in Patients with Chronic Hepatitis B: A Meta-Analysis Diagnostics 20211118710.3390/diagnostics 1102018733525443 PMC 7910971 · doi ↗ · pubmed ↗
- 6Nassal M. HBV ccc DNA: Viral persistence reservoir and key obstacle for a cure of chronic hepatitis B Gut 2015641972198410.1136/gutjnl-2015-30980926048673 · doi ↗ · pubmed ↗
- 7Mak L.Y. Wong D.K. Cheung K.S. Seto W.K. Lai C.L. Yuen M.F. Review article: Hepatitis B core-related antigen (H Bcr Ag): An emerging marker for chronic hepatitis B virus infection Aliment. Pharmacol. Ther.201847435410.1111/apt.1437629035003 · doi ↗ · pubmed ↗
- 8Cao Q.H. Liu H. Yan L.J. Wang H.C. Ding Z.N. Mao X.C. Li R.Z. Pan G.Q. Zhang X. Tian B.W. Role of hepatitis B core-related antigen in predicting the occurrence and recurrence of hepatocellular carcinoma in patients with chronic hepatitis B: A systemic review and meta-analysis J. Gastroenterol. Hepatol.2024391464147510.1111/jgh.1655838686439 · doi ↗ · pubmed ↗