Comprehensive Assessment of Health Risks Associated with Gram-Negative Bacterial Contamination on Healthcare Personnel Gowns in Clinical Settings
Daniela Moreno-Torres, Carlos Alberto Jiménez-Zamarripa, Sandy Mariel Munguía-Mogo, Claudia Camelia Calzada-Mendoza, Clemente Cruz-Cruz, Emilio Mariano Durán-Manuel, Antonio Gutiérrez-Ramírez, Graciela Castro-Escarpulli, Madeleine Edith Vélez-Cruz, Oscar Sosa-Hernández

TL;DR
This study finds that healthcare workers' gowns are often contaminated with dangerous bacteria, especially in critical hospital areas, and recommends better gown hygiene to prevent infection spread.
Contribution
The study provides new insights into the prevalence and types of Gram-negative bacteria on healthcare gowns and their resistance patterns in clinical settings.
Findings
61.05% of healthcare workers' gowns were microbiologically contaminated.
Critical hospital areas like ICUs showed contamination with medically important bacteria.
Some Pantoea eucrina strains showed resistance to carbapenemics and cephalosporins.
Abstract
Microbiological contamination of healthcare workers’ gowns represents a critical risk for the transmission of healthcare-associated infections (HAIs). Despite their use as protective equipment, gowns can act as reservoirs of antibiotic-resistant bacteria, favouring the spread of pathogens between healthcare workers and patients. The presence of these resistant bacteria on healthcare workers’ gowns highlights the urgent need to address this risk as part of infection control strategies. The aim of this work was to assess the microbiological risks associated with the contamination of healthcare staff gowns with Gram-negative bacteria, including the ESKAPE group, and their relationship with antimicrobial resistance. An observational, cross-sectional, prospective study was conducted in 321 hospital workers. The imprinting technique was used to quantify the bacterial load on the gowns,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
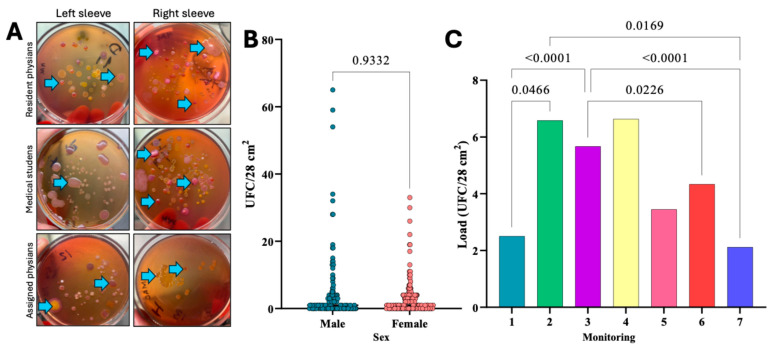 Figure 1
Figure 1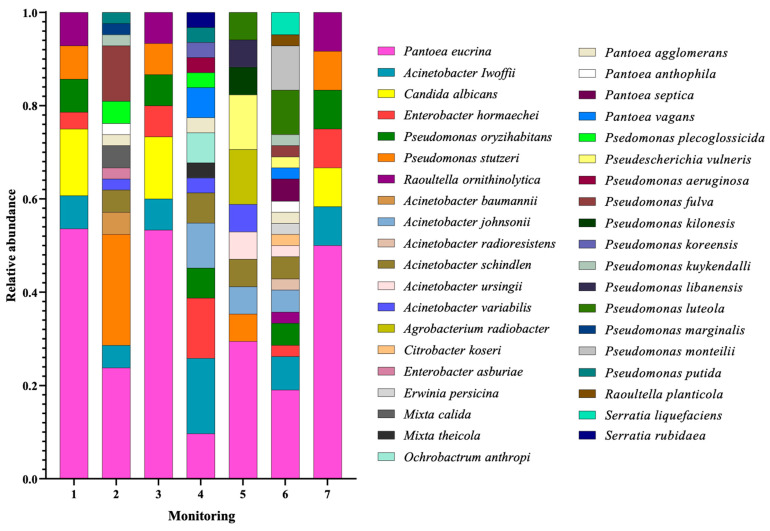 Figure 2
Figure 2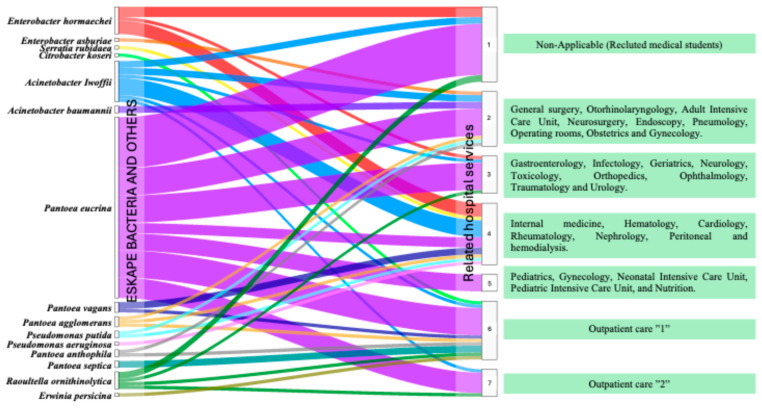 Figure 3
Figure 3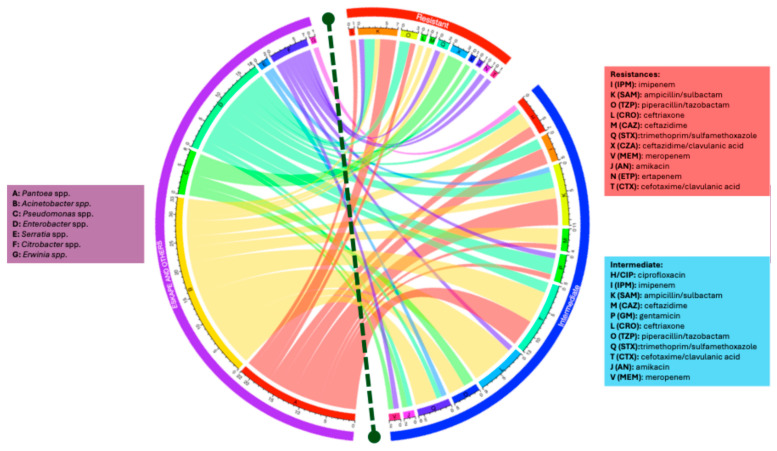 Figure 4
Figure 4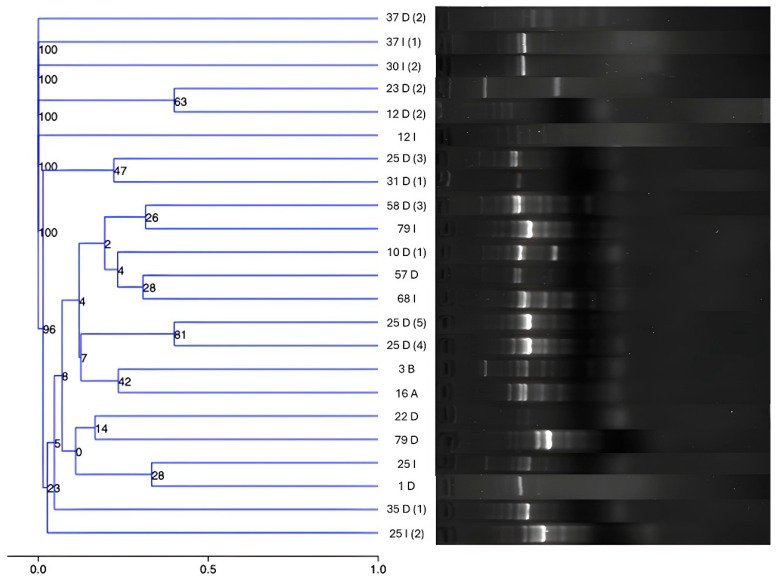 Figure 5
Figure 5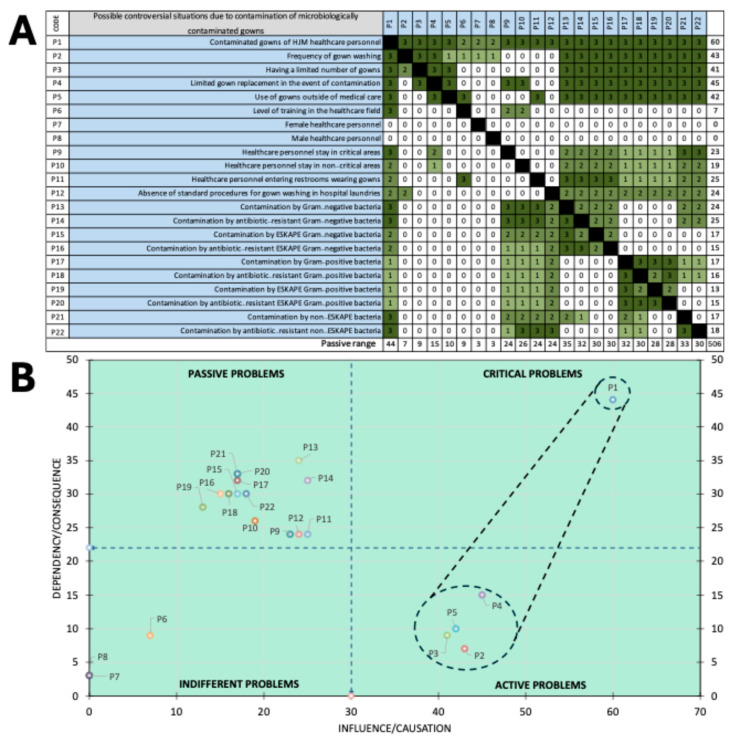 Figure 6
Figure 6| Genus | Species | Healthcare-Associated Infections | Reference |
|---|---|---|---|
|
|
| Catheter-related bloodstream infection | [ |
| Catheter-related bacteraemia | |||
| Sepsis | |||
|
| Sepsis | [ | |
| Catheter-related bacteraemia | [ | ||
| Ventilator-associated pneumonia | [ | ||
| Urinary tract infection | [ | ||
| Bloodstream infection | [ | ||
| Soft tissue infection | [ | ||
|
| Bloodstream infection | [ | |
| Urinary tract infection | [ | ||
|
| Not reported | Non-applicable | |
|
| Bloodstream infection | [ | |
|
|
| Ventilator-associated pneumonia | [ |
| Infection of the skin and soft tissues | |||
| Bacteraemia | |||
| Catheter-related urinary tract infection | [ | ||
| Bloodstream Infection | |||
|
| Catheter-associated bacteraemia | [ | |
| Sepsis | [ | ||
| Pneumonia | |||
| Urinary tract infection | |||
| Skin and wound infections | |||
|
|
| Urinary tract infection | [ |
| Ventilator-associated pneumonia | [ | ||
| Bacteraemia | [ | ||
| Bloodstream infection | [ | ||
| Urinary tract infection | [ | ||
| Pneumonia | |||
| Sepsis | |||
| Wound infection | |||
|
| Ventilator-associated pneumonia | [ | |
| Wound infection | [ | ||
| Bacteraemia | |||
| Catheter-related urinary tract infection | [ | ||
| Bloodstream infection | |||
| Sepsis | [ | ||
|
|
| Ventilator-associated pneumonia | [ |
| Urinary tract infection | |||
| Sepsis | |||
| Bacteraemia | [ | ||
| Infection of the skin and soft tissues | |||
|
| Bacteraemia | [ | |
| Ventilator-associated pneumonia | |||
| Urinary tract infection | |||
| Sepsis | [ | ||
| Bloodstream infection | [ | ||
|
|
| Urinary tract infection | [ |
| Infection of the skin and soft tissues | |||
| Bacteraemia | |||
|
|
| Bacteraemia | [ |
| Ventilator-associated pneumonia | |||
| Sepsis | |||
| Bloodstream Infection | [ | ||
|
|
| Bacteraemia | [ |
| Sepsis | [ | ||
|
|
| Bacteraemia | [ |
|
|
| Not reported | Non-applicable |
|
|
| Bacteraemia | [ |
| Bloodstream infection | |||
| Sepsis | [ | ||
|
| Bloodstream infection | [ | |
| Bacteraemia | |||
|
| Not reported | Non-applicable | |
|
| Not reported | Non-applicable | |
|
| Catheter-associated bacteraemia | [ | |
| Wound infection | |||
| Ventilator-associated pneumonia | [ | ||
| Sepsis | [ | ||
|
| Not reported | Non-applicable | |
|
| Ventilator-associated pneumonia | [ | |
| Urinary tract infection | [ | ||
| Bacteraemia | [ | ||
| Bloodstream infection | [ | ||
|
| Not reported | Non-applicable | |
|
| Not reported | Non-applicable | |
|
| Bacteraemia | [ | |
| Sepsis | |||
|
|
| Bacteraemia | [ |
|
| Not reported | Non-applicable | |
|
| Bloodstream infection | [ | |
|
| Catheter-related bloodstream infection | [ | |
| Bacteraemia | [ | ||
| Sepsis | [ | ||
|
| Bacteraemia | [ | |
| Pneumonia | |||
|
|
| Bacteraemia | [ |
| Sepsis | |||
|
| Not reported | Non-applicable | |
|
|
| Nosocomial pneumonia | [ |
| Surgical site infection | |||
| Bloodstream infection | [ | ||
|
|
| Sepsis | [ |
|
|
| Not reported | Non-applicable |
|
|
| Bloodstream infection | [ |
| Urinary tract infection | [ | ||
|
|
| Catheter-related urinary tract infection | [ |
| Bloodstream infection | |||
| Ventilator-associated pneumonia |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntibiotic Resistance in Bacteria · Bacterial Identification and Susceptibility Testing · Clostridium difficile and Clostridium perfringens research
1. Introduction
Historically, white gowns have been considered a symbol of authority, respect, cleanliness, neatness, commitment to health, and perceived patient safety [1,2,3,4]. In particular, the use of the white coat in healthcare dates to the late 19th century, where Joseph Lister encouraged its adoption as part of antiseptic practices during surgical procedures and thus promoting its use as a symbol of hygiene, safety, and purity [5,6]. Since then, white clothing has been an integral part of the image of healthcare professionals, including nurses, orderlies, laboratory assistants, and laboratory personnel; particularly, the white coat for medical staff has become more relevant because of its impact on the microbiological safety of the patient. Such is the concern about this issue, that its traditional symbol has begun to be questioned [7,8,9]. In this context, microbiological research, involving bacterial culture of the textiles of healthcare workers’ gowns, has shown that far from being protective and safety barriers, they can act as reservoirs of pathogenic and opportunistic microorganisms, contributing to the cross-transmission of bacteria between healthcare workers and patients, leading to the emergence of healthcare-associated infections (HAIs) [7,10].
From a microbiological perspective, in 2017, Gram-negative bacteria, primarily those of the ESKAPE group, classically defined as Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, and Enterobacter species, were recognized by the World Health Organization (WHO) as the leading causes of HAIs worldwide. However, a recent report in 2024 has included a broader range of clinically relevant genera, such as Escherichia coli, Salmonella Typhi, Shigella, Citrobacter, Proteus, Serratia, and Morganella. Therefore, in the critical priority list, members of the order Enterobacterales have been mandatorily included due to their increasing role in nosocomial infections and antimicrobial resistance mainly to fourth-generation cephalosporins and carbapenems, which can now be functionally integrated into the ESKAPE acronym, extending their epidemiological relevance beyond the original six pathogens [11,12].
As can be seen, this acronym has been dynamic in its microbiological composition. In this regard, De Rosa et al. highlighted that the ESKAPE group was never intended to be a closed list but rather a conceptual representation of organisms that “escape” the effects of antimicrobial agents due to their resistance mechanisms and adaptability in clinical settings [13]. Furthermore, debates within the scientific community have emphasized that the ESKAPE group, although originally defined as a fixed set of pathogens, should be interpreted as flexible and expandable, rather than a rigid acronym [14]. This evolving perspective reflects the growing recognition that other bacteria exhibit resistance mechanisms equivalent to those of classical ESKAPE members, including the production of ESBLs and carbapenemases. Several of these genera have been implicated in hospital outbreaks and clonal dissemination events. Therefore, the ESKAPE group should be interpreted as a flexible and expandable framework, rather than a rigid acronym. This allows for its adaptation to the changing landscape of antimicrobial resistance while recognizing that even less common but resistant Enterobacterales, although not always considered primary agents of HAIs, can serve as critical reservoirs of resistance determinants in healthcare settings.
ESKAPE group bacteria are not only relevant because they are the responsible for HAIs but also because they have the ability to acquire antimicrobial resistance mechanisms, such as plasmids, transposons, and integrons, which translates into difficult eradication to antimicrobial treatment [15]. In other studies, on pathways of transmission of in-hospital pathogens, healthcare staff gowns were identified as potentially contaminated by K. pneumoniae, a carbapenemase-producing ESKAPE member, after handling patients infected with this microorganism [16]. Such is the importance of this problem, that contamination of staff hands by A. baumannii has been found to be associated with an increased likelihood of contamination of staff gowns [17]. This highlights the possible relationship between contamination of healthcare staff gowns and the occurrence of HAIs and outbreaks in critical units. In the local context, in our working group, the presence of ESKAPE bacteria has been documented in different scenarios, such as contaminants of invasive medical devices, hands of health personnel, clonal dispersion of ESKAPE bacteria causing outbreaks in the COVID-19 period, and generators of collapse of the pulmonary microbiota, among others [18,19,20,21]. These findings not only demonstrate the problem of these bacteria in the hospital environment but also their possible persistence, where the gowns of healthcare personnel could play an important role in the chain of transmission of pathogens to the patient, as they are often inadvertent routes of transmission. It is important to note that the microbiological risk is not limited to antibiotic-resistant ESKAPE bacteria, as in patients with comorbidities and immunocompromised patients, such as those with cancer, HIV/AIDS, transplant recipients, or chronic diseases, bacteria considered commensal or opportunistic can cause severe infections such as pneumonia, bacteraemia, and sepsis [22,23,24,25].
The problem is exacerbated among healthcare staff in training: students, interns, trainees, and nurses in clinical practice, as these staff, often with less experience and training in infection control, often make prolonged and inappropriate use of gowns, wearing them outside the clinical setting and without regular laundering. This makes gowns potential vehicles for the spread of microorganisms. Therefore, the aim of this study was to perform a risk analysis associated with the microbiological contamination of the gowns of healthcare personnel at Hospital Juárez de México (HJM), with emphasis on Gram-negative ESKAPE bacteria and other Gram-negative bacteria. This was conducted through the phenotypic and genetic characterisation of the microorganisms identified from a focus on antimicrobial resistance to carbapenemics and cephalosporins. Implications for the presence of ESKAPE group bacteria and other Gram-negative bacteria on healthcare workers’ gowns and the associated risks are analysed and discussed.
2. Materials and Methods
2.1. Temporal–Spatial Location, Study Population
This study was observational, cross-sectional, and prospective and conducted from March to May 2025. A population of 321 unduplicated healthcare workers was selected from HJM, a tertiary-level hospital located north of Mexico City. Three inclusion criteria were considered for participants: use of long-sleeved white polyester and cotton gowns (70%/30%) at the time of analysis, participation on Fridays (considering that the gown was used throughout the week), and at 12:00 h, as this was the busiest time in the hospital. Microbiological monitoring was carried out in situ, i.e., in the workplace. Six areas were selected (a, b, c, d, e, and f), since most of the hospital services are concentrated there. In addition, a population of 91 participants was recruited consisting of medical students.
2.2. Quantification of Gram-Negative Bacteria on Healthcare Personnel Gowns
For the quantification of Gram-negative bacteria on the gowns of healthcare personnel, the areas that frequently come into contact with patients and are considered potential sources of cross-contamination were selected. The imprinting technique was used for the quantification of colony-forming units for each back cuff of both sleeves of the gown on Mac Conkey agar plates during 10 s of contact. This procedure was performed on an area of 28 cm^2^ for each cuff. The plates were incubated at 35 ± 2 °C for 24 and 48 h and were counted and reported as CFU/28 cm^2^. The selection of morphotypes of interest was based on microbiological criteria, such as appearance, colour, size, and use of lactose as a carbon source.
Morphotypes that were not of clinical interest were eliminated and not considered for further analysis. With the information obtained, an association analysis was performed by using contingency Tables (Chi^2^) and Mann–Whitney analysis (non-parametric Student’s t-test) to identify significant differences in bacterial loads in both cuffs of the gowns by sex. Conversely, ANOVA and Tukey’s post hoc test were performed to determine significant differences in bacterial loads by areas of analysis. A value of p < 0.05 was considered for the identification of significant differences between microbiological loads by sex and areas. For taxonomic assignment of the bacteria of interest, the typical colonial morphotypes for this type of bacteria were identified and were purified in LB-agar and grown in LB-broth then frozen in glycerol (50%) and stored at −70 °C for future experiments.
2.3. Bacterial Identification by Mass Spectrometry MALDI-TOF
Gram-negative isolates were identified to genus and species level by the direct analysis of whole bacterial cells using matrix-assisted laser desorption/ionization-time of flight mass spectrometry (MALDI-TOF MS). For this purpose, all strains were streaked in LB-agar and incubated overnight at 37 °C, and single colonies were subjected to identification by using a Bruker MALDI Biotyper (Bruker Daltonik, Bremen, Germany) according to the manufacturer’s instructions. The criterion to best match with the identification protocol was bacterial strains with score values above 2.0 (down to 3) for high-confidence identification. MBT Compass Library version 10.0 was used to assign genus and species to the isolates. With the microbiological identification data, graphs of taxonomic diversity and relative abundance by care areas were generated, and an Alluvial diagram was generated in RAW Graph 2.0.1 to know the distribution of the ESKAPE group by healthcare area of the health personnel [26].
2.4. Antimicrobial Resistance Profiles
Isolates that were classified within the ESKAPE group were tested for antimicrobial resistance as follows. The antimicrobial resistance profile was determined through the guidelines established by CLSI, 2024 according to the sensitivity discs set by Enterobacterales, Acinetobacter spp., and P. aeruginosa [27]. The classification of resistance level was conducted according to Magiorakos et al. [28]. P. aeruginosa ATCC 27853 and E. coli ATCC 25922 were used as controls. Results were inferred as susceptible, intermediate, or resistant by measuring the diameter of the inhibition zone. The frequency of antibiotic resistance was calculated and represented in percentages (%).
2.5. Carbapenemases and BLEE Production and Their Relationship with Genotypes
Carbapenem-resistant bacteria strains were subjected to the modified carbapenem inactivation method (mCIM) according to Pierce et al. [29]. Extended-spectrum β-lactamases (BLEE) were detected in solid media, using discs of ceftazidime (30 μg), cefotaxime (30 μg), ceftazidime/acid clavulanic (30 μg/10 μg), and cefotaxime (30 μg/10 μg) according to CLSI [27]. Klebsiella pneumoniae carrying the bla_NDM-1_ gene and K. pneumoniae ATCC 700603 were used as positive controls of carbapenemases [19] and BLEE producers, respectively. Finally, E. coli 25922 was used as a negative control.
2.6. Screening to Detect Resistance Genes
For carbapenemases and BLEE-producing strains, end-point PCR assays were performed to detect metallo-β-lactamases (bla_NDM_, bla_VIM_, and bla_IMP_), serine β-lactamases (bla_KPC_, bla_OXA-48_, bla_OXA-23_, and bla_OXA-40_), and BLEE (bla_SHV_, and bla_CTX-1_) genes using the primers shown in Table 1. Amplicons were run in 1 × TBE buffer, separated via horizontal electrophoresis in 2.0% agarose gels, visualized, compared with an appropriate molecular weight marker, and photographed under UV illumination. Controls for carbapenemases were obtained from Cortés-Ortíz et al. [19] and Loyola-Cruz et al. [20]; K. pneumoniae ATCC 700603 and E. coli BAA-3287 were used as bla_SHV-18_ and bla_CTX-1_ controls.
2.7. Molecular Typing of Pantoea eucrina by ERIC-PCR
Pantoea eucrina strains were subjected to genomic DNA extraction with the commercial Favorgen^®^ Genomic DNA Kit (Omega BIO-TEC, Norcross, GA, USA) according to the manufacturer’s instructions and quantified by fluorometry using the Qubit 4 Fluorometer (Thermo Fisher Scientific, Waltham, MA, USA). Additionally, they were visualised on horizontal 0.8% agarose gels. Molecular typing by ERIC-PCR was performed according to Versalovic et al. [32] as follows. The reaction volume was 50 μL and consisted of Molecular Biology grade water, 1 × PCR buffer, 20 nM MgCl_2_, 25 mM deoxyribonucleotide phosphate, 100 pM of each primer, 3 units Taq DNA polymerase, and 300 ng of template DNA. Cycling conditions were as follows: pre-denaturation at 95 °C for 7 min, denaturation at 90 °C for 30 s, annealing at 58 °C for 1 min, and extension at 65 °C for 8 min, with a final extension at 68 °C for 16 min at the end for 30 cycles. Genetic profiles were run 1 × TBE buffer, pH 8.3, and separated on horizontal electrophoresis in 1% agarose gels, visualised, and photographed under UV illumination.
Genetic profiles were analysed by intra-gel pattern comparison by using ImageLab 5.2.1. To confirm the reproducibility of assays, they were performed three times. Tenover criteria were used to establish the clonal relationship between isolates [33]. Finally, graphical relationship was performed through distance matrix by using a linear semilogarithmic method. The dendrograms were constructed by using the UPGMA algorithm, with the Dice similarity index. Genomic similarities were confirmed with a bootstrap test of 1000 repetitions by using the Past4 program (Version 4.09).
2.8. Risk Assessment by Using a Vester Matrix
With the microbiological and genetic findings, a Vester matrix was constructed to classify according to their degree of causality the problems associated with the contaminated gowns of the health personnel of HJM. Twenty-two risk scenarios were identified that could have an impact on various infectious health-risk outcomes. The causality of the scenarios was assessed individually and as a group by various health professionals, including 5 microbiologists, 3 infectious disease physicians, 3 epidemiologists, and 3 nurses. With the causality results (0, 1, 2, and 3), the most frequently occurring problems were considered to have the closest causality to reality and were transferred to the matrix to categorise them as active, passive, critical, or indifferent problems [34].
3. Results
3.1. Study Population and Related Hospital Services
Table 2 shows the study population categorised according to their professional role within the HJM. A total of 321 participants were recruited, distributed in 143 males and 178 females, respectively. The participants were distributed among 28 different hospital services, 8 of which were considered critical areas (adult, neonatal and paediatric intensive care units, operating theatres, peritoneal dialysis, haemodialysis, pneumology, and toxicology). The study population was distributed as resident physicians (48.9%), trainees (48.6%), and only 2.5%, which corresponded to assigned physicians. The group of medical students recruited (n = 91) consisted of 41 males and 50 females, respectively.
3.2. Analysis of Microbiological Contamination According to Sex
Microbiological analysis by imprinting of the back cuff of healthcare personnel revealed the presence of various morphotypes of clinical interest. Figure 1A shows representative images of microbiological findings with morphotypes of clinical interest and marked with blue arrows. Frequency analysis of microbiological contamination by Gram-negative bacteria showed that 87 (60.8%) and 109 (61.2%) male and female participants, respectively, showed evidence of contamination by Gram-negative bacteria, with maximum and minimum values of 60 and 37 CFU/28 cm^2^, respectively. The overall contamination rate was 61.05%, representing 196 participants. With this finding, a Chi-squared test (p ≤ 0.05) was performed, which showed that the sex of the health personnel is not associated with the degree of microbiological contamination by Gram-negative bacteria (p = 0.942). To validate the above observations, two additional tests were performed to determine the association. The first was the likelihood ratio, which showed no association between sex and bacterial growth (p = 1). A continuity correlation (p = 0.942) was performed, which showed that the observed frequencies were the same as expected, concluding that sex had no apparent effect on bacterial growth. The minimum number of samples required for the Chi-square test (n ≥ 5) was also exceeded. Likewise, the Mann–Whitney analysis confirmed the absence of association with the sex of health personnel (p = 0.9332) (Figure 1B).
3.3. Comparison of Microbiological Contamination of Gowns by Hospital Care Area
The results of the post hoc ANOVA test to compare the Gram-negative bacterial load (CFU/28 cm^2^) by hospital care areas, including the medical student population (monitoring 1), are shown in Figure 1C. The results show that some areas showed significant differences compared to others, suggesting important variations in the bacterial load of interest (p ≤ 0.05). The key areas with the highest bacterial contamination were 2 (general surgery, otorhinolaryngology, adult intensive care unit, neurosurgery, endoscopy, pneumology, operating rooms, obstetrics, and gynaecology), 3 (gastroenterology, infectology, geriatrics, neurology, toxicology, orthopaedics, ophthalmology, traumatology, and urology) and 4 (internal medicine, haematology, cardiology, rheumatology, nephrology, peritoneal, and haemodialysis). Figure 1C shows the results of the post hoc ANOVA analysis comparing the Gram-negative bacterial load (CFU/28 cm^2^) by the care areas of HJM.
3.4. Taxonomic Characterization of Microorganisms Isolated from Healthcare Gowns
Mass spectrometry analysis of the taxonomic diversity at genus and species level of the 184 isolates from the gowns revealed the presence of a total of 12 bacterial genera. Interestingly, the yeast genus and species Candida albicans was detected in the microbiological isolation (monitoring 1, 3, and 7). The analysis of number of species per bacterial genus was represented as follows: Pseudomonas (n = 13), Acinetobacter (n = 7), Pantoea (n = 5), Enterobacter (n = 2), Raoultella (n = 2), Mixta (n = 2), Serratia (n = 2), Agrobacterium (n = 1), Citrobacter (n = 1), Erwinia (n = 1), Ochrobactrum (n = 1), and Pseudoscherichia (n = 1). Analysis by focus area revealed the presence of 7, 15, 7, 16, 11, 22, and 7 different species in monitoring/areas 1, 2, 3, 4, 5, 6, and 7, respectively.
The most prevalent genus and species that was consistently identified across all surveys was P. eucrina with maximum and minimum relative abundances of 0.57 (survey 1) and 0.56 (survey/area 4) (Figure 2). Interestingly, 3 members of the ESKAPE group were detected, represented by A. baumannii, P. aeruginosa, and 12 Enterobacterales, such as P. eucrina, P. vagans, P. agglomerans, P. septica, P. antophilia, E. hormaechei, E. asburiae, R. ornithinolytica, S. rubidaea, C. koseri, and Erwinia persicina. Figure 2 shows the results of mass spectrometric identification of Gram-negative bacteria isolated from the gowns of healthcare personnel at HJM.
3.5. Flow of ESKAPE Bacteria on Healthcare Staff Gowns by Hospital Service
The distribution of bacteria belonging to the ESKAPE group isolated from the gowns of healthcare personnel across various hospital services was analysed. The bacteria considered in this analysis included A. baumannii, P. aeruginosa, Enterobacterales, and others. The results show clear flow patterns between ESKAPE bacteria and the hospital services where they are most prevalent. The flow diagram revealed that P. eucrina, in addition to having the highest frequency of isolation, has a notable flow to all areas analysed, with medical students being the population where the highest number of isolates was identified. However, in the eight critical areas of HJM (adult, neonatal, and paediatric intensive care units, operating theatres, peritoneal dialysis, haemodialysis, pneumology, and toxicology), it was also detected.
In particular, the two Acinetobacter species were found to be related to seven of the areas studied, with A. baumannii standing out in adult intensive care units, an area where cases of ventilator-associated pneumonia (VAP) are concentrated. Conversely, bacteria such as E. hormachei were identified in six hospital services, including the medical student population.
The results also show the presence of P. aeruginosa in area 4. Among other relevant findings, Pantoea showed a diverse distribution, occurring in services such as gastroenterology, paediatrics, and general surgery. Regarding outpatient services, other Gram-negative bacteria are more prevalent in outpatient areas (6 and 7) compared to high-specialty hospital services, suggesting external environmental contamination. Figure 3 shows the distribution flow of ESKAPE bacteria and others isolated from healthcare staff gowns in the different care areas of HJM.
3.6. Resistance Phenotypes in Isolates from HJM Healthcare Staff Gowns
Figure 4 shows the distribution of antimicrobial resistance phenotypes of interest (resistant and intermediate) in ESKAPE bacteria and others isolated from HJM healthcare staff gowns. As it can be observed, the population with the highest burden of antimicrobial “resistance” phenotypes was the Acinetobacter group (A. baumannii and A. lwoffii), represented by β-lactamases, cephalosporins, and folate metabolism inhibitors. Secondly, the genera Enterobacter and Pantoea showed resistance to the same β-lactamics. Interestingly, the genus Pseudomonas, although one of the least frequent resistant groups, showed resistance to carbapenemics (meropenem) and cephalosporins. Finally, the genus Citrobacter showed interesting resistance profiles, most notably to trimethoprim/sulfamethoxazole and ertapenem and cefotaxime/clavulanic acid. The genera Erwinia and Serratia showed profiles categorised as “intermediate resistance”.
3.7. Resistance to Cephalosporins and Carbapenemics in ESKAPE Bacteria and Others
The production of BLEE, carbapenemases, and resistance genotypes was assessed in all isolates that showed “resistant and intermediate” categorization profiles to cephalosporins and carbapenems according to CLIS, respectively. This evaluation revealed the presence of carbapenemases and BLEE in nine isolates of P. eucrina, where in one isolate the coexistence and/or production of both enzymes was detected. These phenotypes were conferred by serine β-lactamases type bla_KPC_ and β-lactamase type bla_CTX-1_ for carbapenemics and cephalosporins, respectively. For P. putida, carbapenemase production was identified in one isolate with the bla_KPC_ genotype. The genotype was not detected in E. asburiae and C. koseri. Table 3 summarizes the phenotype or carbapenemase and BLEE production findings and the associated genotype according to Table 1.
3.8. Analysis of Intergenic Consensus Reveals a Broad Diversity of P. eucrina
The decision to conduct clonal analysis on P. eucrina was driven by its predominance among the isolates recovered from healthcare personnel gowns. Genomic diversity analysis using the ERIC-PCR fingerprinting method revealed sizes of amplicons ranged from slightly more than 100 bp to about 800 bp. Intergenic region diversity of P. eucrina showed that the 23 isolates were grouped as unique strains. Therefore, clonal groups were not found. Figure 5 shows the genomic diversity of P. eucrina strains isolated from HJM healthcare personnel gowns, as assessed by dendrogram analysis using ERIC-PCR.
3.9. Identification of Problems Associated with Microbiological Contamination of Gowns
Using the microbiological and genetic findings, a Vester matrix was constructed to classify 22 microbiological situations according to their degree of causality to determine which resulted in the four types of microbiological problems associated with the contamination of HJM healthcare staff gowns (Figure 6A). The analysis revealed three indifferent problems (P6 to P9) of low influence and dependence, indicating that the sex of the health personnel and the level of academic training do not represent threats in terms of microbiological contamination of gowns. Thirteen passive problems (P9 to P22) were identified as having a higher dependence but lower influence. These items should be considered for the prevention of contamination of the gowns, although they do not have an immediate impact compared to the critical issues. Finally, four active problems (P2 to P5) were identified as the most significant problems, with high influence and high dependence, indicating that they have a high risk of contributing to microbiological contamination. These problems should be prioritized in interventions to control and prevent contamination of healthcare workers’ gowns.
4. Discussion
Classically, the epidemiological triad consists of the pathogen, the host, and the environment, and their interaction is essential in the development of HAIs [35]. Currently, epidemiological research has focused on the study of the agent and the host, but the environment, although often underestimated, has been shown to play a critical role in the chain of pathogen transmission, and its study is key to strengthening infection prevention and control strategies. In previous work by our working group, we have recognized that the “environment” factor includes not only hospital facilities but also medical devices, air, and inert surfaces [18,36,37]. However, a frequently forgotten element is the gown, which, despite being emblematically a symbol of authority and safety in the hospital field, has not been sufficiently considered as a reservoir and vector of pathogens. Therefore, the aim of this study was to assess the health risks associated with microbiologically contaminated gowns of HJM healthcare personnel and to propose infection control strategies focused on this garment, given its potential as a reservoir of antibiotic-resistant pathogens and its role in the transmission of infections. As can be observed in the results section, the microbiological analysis carried out on the gowns of healthcare personnel showed high rates of bacterial contamination by Gram-negative bacteria (61.05%). This finding is relevant, as healthcare staff gowns, which have traditionally been seen as a protective barrier, could be acting as reservoirs of microorganisms, favouring cross-transmission of bacteria between healthcare staff and patients [17,23]. The distribution of bacterial contamination was similar for males and females, indicating that gender did not significantly influence the bacterial load of the gowns (Figure 1B). This result is consistent with previous research that has shown that the gowns of male and female staff are similar [38,39]; however, some others have observed that microbiological contamination rates show an opposite behaviour and reveal higher microbiological contamination related to the sex of healthcare staff [40,41]. Regardless of this variable, these findings reinforce the hypothesis that bacterial contamination on gowns can be sources of transmission, especially when staff do not follow proper gown hygiene and maintenance protocols, including washing [7,8]. Although Gram-positive bacteria such as methicillin-resistant Staphylococcus aureus (MRSA) are well-known colonisers in healthcare settings, this study focused on Gram-negative organisms due to their epidemiological predominance at HJM. Surveillance data and prior studies have consistently identified multidrug-resistant Enterobacterales, P. aeruginosa, and A. baumannii as leading pathogens in nosocomial infections and surface contamination [18,20]. Future investigations will explore the role of MRSA and other Gram-positive species in gown-associated transmission.
Additionally, some Gram-negative isolates recovered in this study grouped in Enterobacterales were included in the risk analysis. These microorganisms referred to here as “other bacteria” were Citrobacter koseri, Erwinia persicina, Mixta, Ochrobactrum anthropic, and others. Despite being less frequent, these organisms exhibited resistance phenotypes to clinically important antibiotics and have been documented in the literature as opportunistic or emerging pathogens in healthcare settings (Table 4). Their detection in critical care areas underscores the importance of including them in the microbiological risk assessment, as they may act as reservoirs of resistance genes and contribute to nosocomial transmission chains.
It is important to note that although no significant difference by sex was observed, it is crucial to identify other variables, such as type of clinical activity and frequency of contact with patients, that could be contributing to contamination. A relevant aspect shown in Figure 1C is the identification of areas where healthcare staff showed higher contamination rates, highlighting areas 2 and 4, where critical patients such as ICU, peritoneal dialysis, and haemodialysis units are admitted (Table 2 and Figure 3). These areas are particularly special because of invasive procedures and the use of medical devices such as mechanical ventilators and catheters in susceptible patients. Interestingly, in one of these areas, A. baumannii was identified, a bacterium classified as ESKAPE and a generator of HAIs, with VAP being the most important in our hospital and causing high costs in its care [42].
Regarding bacterial identification by MALDI-TOF mass spectrometry, the technology allowed the identification of a wide diversity of bacterial genera and species (including yeasts such as C. albicans). Prevalent genera included Pseudomonas, Acinetobacter, Pantoea, Enterobacter, and Raoultella, microorganisms that have been directly linked to hospital-acquired infections. A summary of the extensive review of the scientific literature on the microbiological results of this study and their relationship to cases of nosocomial infections is shown in Table 4.
Specifically, P. eucrina stood out as the prevalent species, being detected in all areas analysed (Figure 2 and Figure 3). This finding is relevant since, to our knowledge, P. eucrina has been little studied in hospital settings, as all efforts in our hospital and elsewhere in the world are focused on the detection and characterisation of typical ESKAPE bacteria [26,95]; however, the presence of P. eucrina on staff gowns suggests that it could be playing an important role in the transmission of nosocomial infections. This hypothesis is reinforced because, in previous work in our working group, this microorganism was detected in the linen containers of adult ICUs during COVID-19 [18]. In this study, strain typing was performed exclusively on Pantoea eucrina isolates. This decision was based on the fact that P. eucrina was the most frequently recovered species and the only one consistently detected across all monitored hospital areas. Its widespread presence suggested the possibility of clonal dissemination or environmental persistence, which warranted deeper analysis. In contrast, other bacterial species were isolated less frequently or appeared in specific areas only, limiting the interpretative value of typing. Thus, the selection of P. eucrina for typing was strategic, aiming to understand its potential role as a persistent and underrecognized agent in hospital-associated microbial transmission.
Although P. eucrina is not classically categorized as a member of the ESKAPE group, we included it functionally in our analysis due to its consistent isolation across all hospital areas, its phenotypic resistance to critical antibiotics, and its clinical relevance as reflected in Table 4. As a genus within the Enterobacterales, Pantoea shares phylogenetic and resistance-related features with other established ESKAPE members. The dynamic nature of the ESKAPE framework, as discussed earlier, supports the consideration of non-traditional but increasingly relevant pathogens, especially those with nosocomial potential and antimicrobial resistance as part of an expanded ESKAPE concept. In this context, we propose that P. eucrina may be viewed as a potential ESKAPE-related pathogen, particularly in institutions where it demonstrates wide distribution and resistance traits, as shown in our data. This approach aligns with the evolving epidemiology of hospital-acquired infections and the need to adapt bacterial surveillance.
The identification results also showed the presence of bacteria typical of the ESKAPE group, such as A. baumannii and P. aeruginosa, known for their antibiotic resistance and their ability to cause serious infections in hospitalized patients, especially those with chronic diseases or immunocompromised [96]. On the other hand, C. albicans was not the main focus of the present study, its detection on healthcare personnel gowns is noteworthy given its known association with catheter-related infections and others in immunocompromised patients [61]. This incidental finding reinforces the importance of further exploring fungal contamination in future studies. Analysis of bacterial flow through the different areas of the hospital showed that P. eucrina had a widespread distribution across all hospital services, including the medical student population (monitoring 1), in addition to having the highest frequency of isolation and showed a remarkable flow towards critical areas (Figure 3). Furthermore, this analysis revealed that medical students had a higher prevalence of this microorganism on their gowns, suggesting that they may act as a vector of transmission (Figure 3). We initially speculated that lack of infection control training was one of the reasons for the high contamination rates. Nevertheless, the Vester matrix classified this situation as an indifferent problem, i.e., with little influence on the main problem. This finding is interpreted on the premise that some basic practices, such as avoiding the use of gowns outside the clinical setting or transferring them to toilets are activities considered obvious, even without formal infection control training. Nonetheless, we speculate that other factors may have a greater impact on gown contamination, such as prolonged unwashed gown use outside the hospital, the absence of institutional gown laundering programs, subjective perceptions of gown cleanliness and personal hygiene habits.
These factors may be more determinant than academic training in infection control. The patterns of antimicrobial resistance phenotypes and genotypes shown in Figure 4 and Table 3 are worrying, as cephalosporins and carbapenemics are the antibiotics used par excellence in therapy at HJM and were the “resistance” and “intermediate resistance” profiles identified in the isolates of the ESKAPE group. This situation compromises and hinders patient recovery from nosocomial infections, especially in immunocompromised patients [97]. The fact that Pantoea, Acinetobacter, Pseudomonas, Enterobacter, Serratia, Citrobacter, and Erwnia genera with “resistance” and “intermediate resistance” profiles on healthcare personnel gowns highlights the urgent need for control strategies that not only address the cleaning of surfaces and equipment but also include gown laundering protocols.
A notable finding was the existence and coexistence of carbapenemases and BLEE in P. eucrina strains, highlighting their ability to acquire resistance mechanisms to last-line antibiotics. The presence of these enzymes in this microorganism, which to some extent has been forgotten in the hospital environment, is alarming, as it would complicate its elimination in an infectious process. To our knowledge there are few works that have reported this bacterial genus producing bla_VIM_ and bla_OXA-48_ carbapenemases and carrying genes associated with the horizontal transfer machinery of extrachromosomal genetic material, which could explain our findings [98,99,100,101]. Finally, the tool for identifying the problems to attack was the Vester matrix.
The fact that four problems were classified as active highlights the urgency of taking measures to reduce microbiological contamination in the gowns of healthcare personnel, especially those in critical areas such as ICUs, operating theatres, and dialysis units, where the risk of transmission could have the greatest impact (Figure 6). Among these, this study identifies actions that may be obvious to some extent but are crucial: increasing the frequency of gown washing, changing gowns in the event of a contamination event (visible or not), and avoiding the use of gowns outside the clinical environment altogether. It is worth noting that, during the time this study was conducted, HJM did not have any formal institutional protocols in place for the management of healthcare personnel gowns. There were no standardized procedures regarding how gowns should be distributed, how often they should be washed, whether they are intended for single or multiple uses, or who is responsible for their maintenance. In practice, most healthcare workers acquire and care for their own gowns individually, often guided by personal habits or perceptions of cleanliness rather than evidence-based practices. This lack of structure creates an environment where the gowns originally intended as a symbol of professionalism and protection can inadvertently become vectors of microbial transmission. Our findings underscore the need to address this gap and to move toward institutional policies that consider gown management as an essential component of infection prevention strategies, especially in critical care settings.
Now, while there is information from other parts of the world where drastic measures have been taken to justify the elimination of gowns for medical staff for the purpose of infection control of Clostridioides difficile and methylcillin-resistant S. aureus [102,103], there are other studies that have shown that the elimination of gowns could affect the doctor–patient relationship, as well as showing impacts such as the disposal of thousands of white coats and even the “deterioration of the doctor’s image” [104]. Nevertheless, with the rise of multidrug resistance, extensive drug resistance, and pandrug resistance in ESKAPE pathogens, the appraisals of healthcare staff attire are outweighed by the cost–benefit of replacing gowns with short-sleeved uniforms in all hospital services. This hypothesis is reinforced through previous work by our working group, where we demonstrated that VAP can be up to nine times more costly when the causative agent is multidrug-resistant bacteria; not to mention the reduction in mortality [42].
5. Conclusions
The findings presented in this study show the importance of implementing infection control strategies that are not limited to the patient and the causative agent. The fact that P. eucrina and other medically important microorganisms with antimicrobial resistance are distributed on the gowns of healthcare personnel in training reinforces the idea of the need to improve the importance of this garment, as it has been shown to serve as a significant reservoir of pathogenic bacteria, particularly in critical areas of the hospital. Within our reach, we believe that by increasing the number and frequency of gown laundering, and ideally by having institutional gown laundering programs in place, we could ensure that every attending physician, resident physician, or medical student wears a “safe gown” when in contact with patients, the basis of healthcare personnel’s work.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gjerdingen D.K. Simpson D.E. Titus S.L. Patients’ and physicians’ attitudes regarding the physician’s professional appearance Arch. Intern. Med.19871471209121210.1001/archinte.1987.003700700230023606278 · doi ↗ · pubmed ↗
- 2Landry M. Dornelles A.C. Hayek G. Deichmann R.E. Patient Preferences for Doctor Attire: The White Coat’s Place in the Medical Profession Ochsner J.20131333434224052762 PMC 3776508 · pubmed ↗
- 3Kazory A. Physicians, their appearance, and the white coat Am. J. Med.200812182582810.1016/j.amjmed.2008.05.03018724974 · doi ↗ · pubmed ↗
- 4Mitchell K. Phillips K. Pocotte S. Lee C. The creation of a White Coat Ceremony J. Prof. Nurs.20203621822210.1016/j.profnurs.2020.01.00432819547 · doi ↗ · pubmed ↗
- 5Worboys M. Joseph Lister and the performance of antiseptic surgery Notes Rec. R Soc. Lond.20136719920910.1098/rsnr.2013.002824686323 PMC 3744349 · doi ↗ · pubmed ↗
- 6Michaleas S.N. Laios K. Charalabopoulos A. Samonis G. Karamanou M. Joseph Lister (1827–1912): A Pioneer of Antiseptic Surgery Cureus 202214 e 3277710.7759/cureus.3277736686094 PMC 9854334 · doi ↗ · pubmed ↗
- 7Treakle A.M. Thom K.A. Furuno J.P. Strauss S.M. Harris A.D. Perencevich E.N. Bacterial contamination of health care workers’ white coats Am. J. Infect. Control 20093710110510.1016/j.ajic.2008.03.00918834751 PMC 2892863 · doi ↗ · pubmed ↗
- 8Mishra S.K. Maharjan S. Yadav S.K. Sah N.P. Sharma S. Parajuli K. Sherchand J.B. Bacteria on Medical Professionals’ White Coats in a University Hospital Can. J. Infect. Dis. Med. Microbiol.20202020595728410.1155/2020/595728433178371 PMC 7644330 · doi ↗ · pubmed ↗