CNS Tumor with BCOR/BCORL1 Fusion: A Rare Tumor Entity
Jerry Lou, William Yong, Kenneth Aldape, Eleanor Chu, Caressa Hui, Frank P. K. Hsu, Michelle Zheng, Anatevka Ribeiro, Gianna Fote, Daniel Na, Carlen A. Yuen

TL;DR
A rare CNS tumor involving BCOR/BCORL1 fusion is described, with a new case showing successful treatment using radiation and temozolomide.
Contribution
The paper presents a new case of a rare CNS tumor with BCOR/BCORL1 fusion and highlights a novel treatment approach.
Findings
A 37-year-old woman with a BCOR/BCORL1 fusion tumor was successfully treated with radiation and temozolomide.
EMA showed focal strong dot-like perinuclear immunoreactivity, a feature not previously reported in these tumors.
The case supports the use of radiation and temozolomide for tumors in the BCOR/BCORL1 fusion methylation class without detectable fusion.
Abstract
Central nervous system (CNS) tumor with BCL6 corepressor gene BCOR/BCORL1 fusion is an extremely rare tumor entity, with fewer than 40 cases reported. These tumors are distinct from the WHO 2021-defined CNS tumor with BCOR internal tandem duplication. Even rarer are CNS tumors that match to the methylation class of CNS tumors with BCOR/BCORL1 fusion, but lack fusions and instead harbor truncating small nucleotide variants in BCOR. To our knowledge, only two other cases of this scenario have been previously reported. Due to their scarcity and morphological features that mimic oligodendrogliomas and ependymomas, the diagnosis of CNS tumor with BCOR/BCORL1 fusion can be challenging, and misdiagnoses are not uncommon. Histologic findings of Olig2 positivity with focal to absent GFAP warrant further evaluation for this tumor entity. Moreover, no standard of care therapy exists for these…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
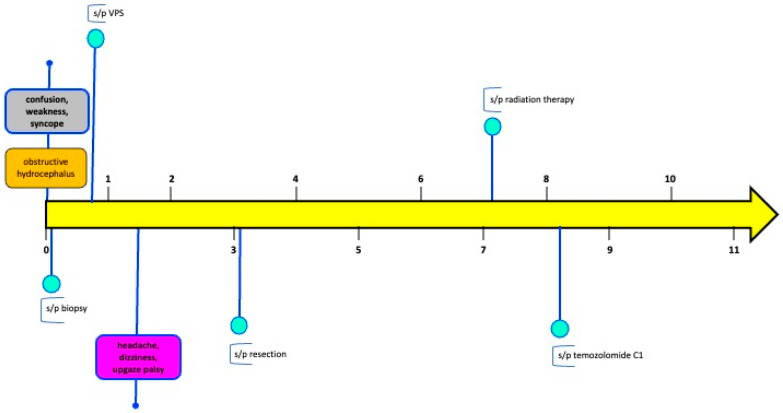 Figure 1
Figure 1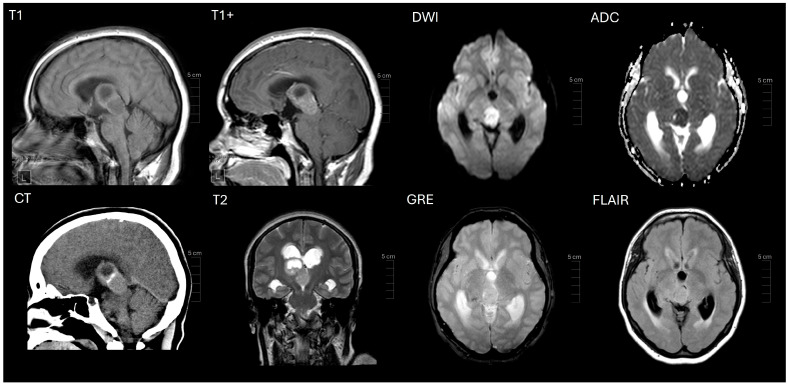 Figure 2
Figure 2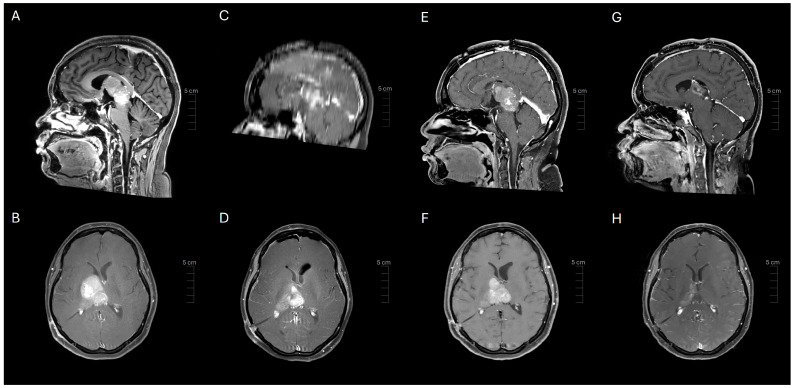 Figure 3
Figure 3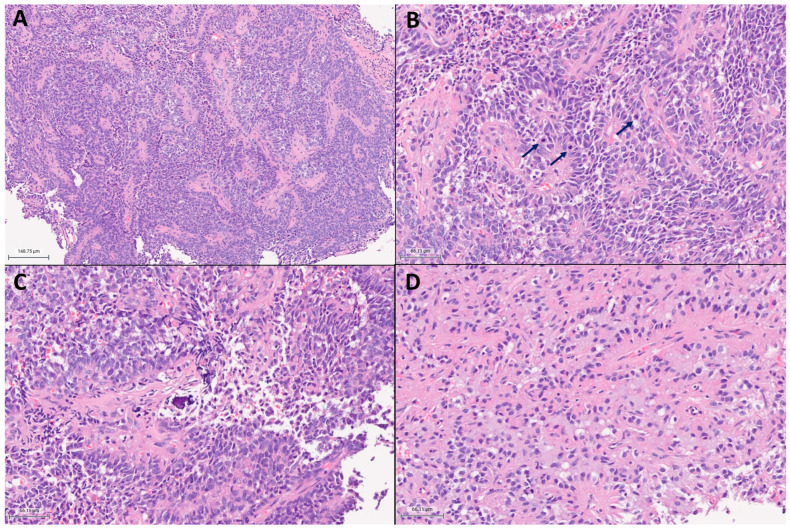 Figure 4
Figure 4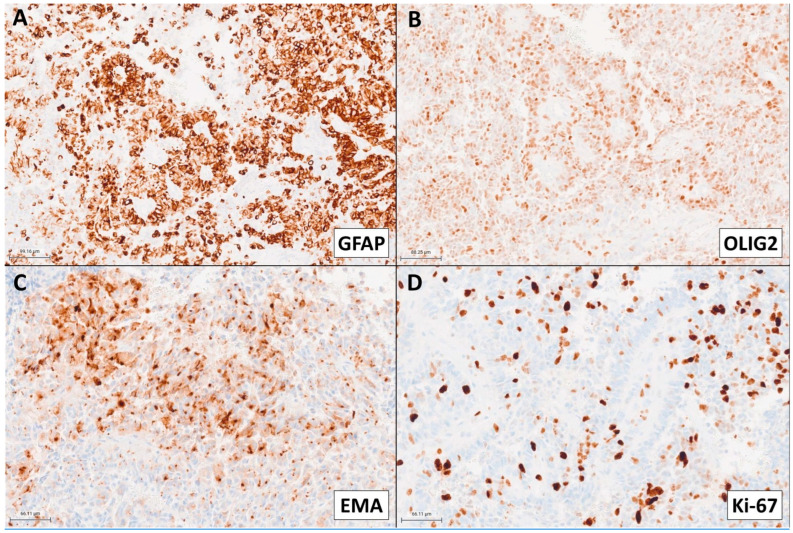 Figure 5
Figure 5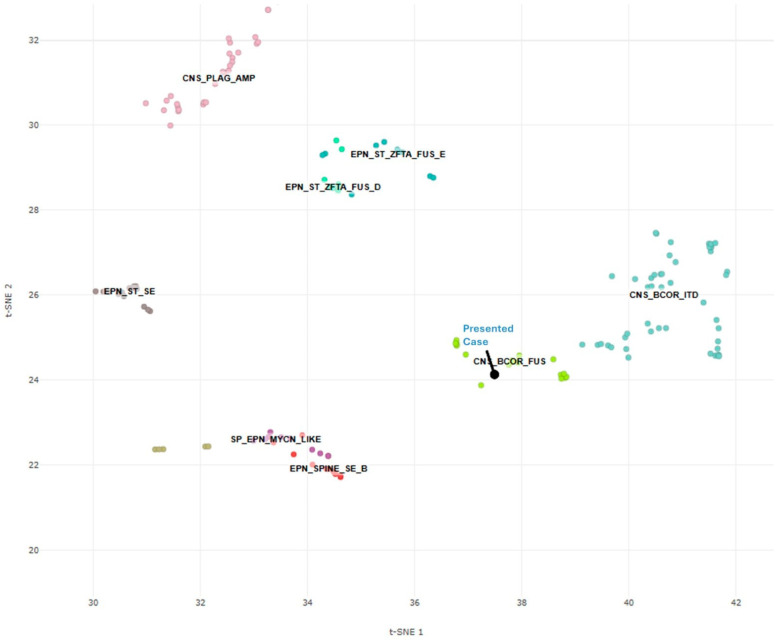 Figure 6
Figure 6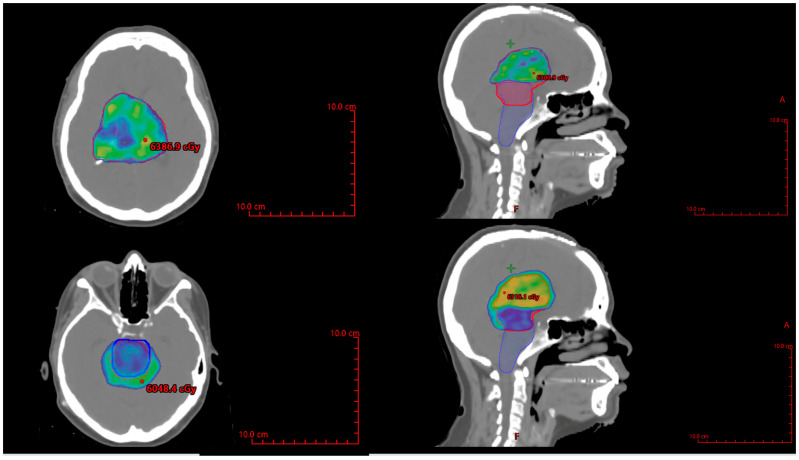 Figure 7
Figure 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlioma Diagnosis and Treatment · Brain Metastases and Treatment · Neuroblastoma Research and Treatments
1. Introduction
The World Health Organization (WHO)’s classification of central nervous system (CNS) tumors continues to undergo revisions to improve the diagnostic accuracy for CNS-primitive neuroectodermal tumors (PNETs). Each new iteration refines and expands upon the existing diagnostic categories. The 2021 WHO classification of CNS tumors defined a new CNS-PNET tumor entity: CNS tumor with BCL6 corepressor gene (BCOR) internal tandem duplication (ITD) [1,2,3]. The BCOR gene, located on Xq26.1, is a tumor suppressor gene and an epigenetic regulator that mediates cell differentiation and structural development, while contributing to polycomb repressive complexes (PRCs) [4,5,6,7,8,9,10]. PRC1 is a main regulator of cellular outcome and stem cell existence [10,11]. PRC1.1 alterations are associated with BCOR and BCOR(L1) [10]. Accordingly, a loss of function mutation in the BCOR gene interrupts tumor suppression functioning and thereby leads to tumorigenesis. Additionally, ITDs and oncogenic gene fusions are alternate drivers of tumorigenesis [3,12,13,14].
The updated WHO classification schemes have increasingly incorporated DNA methylation profiling as an ancillary diagnostic tool. A diagnosis of CNS tumor with BCOR-ITD can be designated by histologic criteria coupled with an ITD in Exon 15 of BCOR or DNA methylation profiling in unresolved cases [2]. CNS tumor with a BCOR or BCOR Like 1 (L1) fusion entity has a unique DNA methylation signature that is molecularly distinct from CNS tumor with BCOR-ITD and is not yet recognized in the WHO classification of CNS tumors [15]. BCOR-L1 is a BCOR homolog and is an intense transcriptional corepressor when tethered to a heterologous promoter [9,16]. Limited information exists for this exceptionally rare tumor that is characterized by the presence of a BCOR/BCOR(L1) fusion, copy number variations within chromosomes Xp11.4 and 22q12.31, or truncating small nucleotide variants [14,17]. Moreover, little is known about the relationship between BCOR-fusion tumors and BCOR-ITDs. However, biological differences have been reported between these tumors. In stark contrast to BCOR-ITD tumors, BCOR-fusion tumors more commonly occur in adults [14,18,19]. Evidence is conflicting for any sex differences [14,20]. The median age at presentation for patients with BCOR-fusion tumors is 27–30 years of age, but broadly presents between the ages of 5 and 72 years [14,20]. The median progression-free survival for these tumors is 16 months, but ranges from 1 to 86 months [14,18,19]. The median overall survival is 27 months and data suggest that patients with BCOR-fusion tumors portend better prognosis compared to BCOR-ITD [18,19,20].
On diagnostic imaging, CNS tumors with BCOR/BCOR(L1) fusion commonly arise within or adjacent to the ventricles and are characteristically T1-hypointense and T2-hyperintense [17,19]. These tumors can be well-demarcated or diffusely infiltrating and with or without enhancement [17,18].
CNS tumors with BCOR/BCOR(L1) fusion are mimickers of other diseases. Histology demonstrates intra- and inter-tumor heterogeneity, including oligodendroglioma-like, ependymoma-like, and embryonal features, frequently with focal calcifications and/or myxoid change [14,17]. Tumor cells show diverse cytology ranging from round to ovoid, and occasionally angulated nuclei with delicate to hyperchromatic chromatin and clear to eosinophilic cytoplasm, occasionally with intracytoplasmic vacuolation [14,17]. Malignant features include necrosis and elevated mitotic activity, and less commonly, microvascular proliferation [14,19]. Ependymoma-like perivascular pseudorosettes and/or oligodendroglioma-like chicken-wire vasculature are consistently encountered [14,17,19,21]. Olig2 is commonly expressed, and GFAP may be focally present or absent [14,17,19]. Accordingly, these tumors can be misdiagnosed as supratentorial ependymoma, oligodendroglioma, astrocytoma, glioblastoma, or ganglioglioma [14]. However, molecular advances have improved upon the classification of CNS tumors. The presence of MYCN amplification or fusions in ZFTA or YAP1 is suggestive of ependymoma [1]. The presence of mutations in IDH1, IDH2, 1p/19q, TERT promoter, CIC, FUBP1, and NOTCH1 is suggestive of oligodendroglioma [1].
Positivity for glial markers in the presence of a BCOR fusion justifies a provisional designation as glioma with BCOR fusion [14]. BCOR fusion or a matching methylation class distinguishes these CNS tumors from BCOR-ITD [14]. BCOR-fusion methylation class tumors are characterized by EP300 or CREBBP as BCOR/BCOR(L1)-fusion partners, an MEAF6::CXXC5 fusion, a BCOR stop mutation, or CNV breakpoints at the EP300 and BCOR loci on chromosomes X or 22 [14,17].
There are fewer than 40 reported cases, warranting further investigations into the clinical behavior and radiographic, pathologic, and genomic features of this rare tumor entity [17]. No standard of care therapy exists, further highlighting the need to deepen our understanding of CNS tumors with BCOR/BCOR(L1) fusion. Herein, we present a case of a 37-year-old female with a CNS tumor harboring a pathologic BCOR c.626del (p.S209Cfs*7) (Exon 4) variant that matched the same methylation class as CNS tumors with BCOR/BCOR(L1) fusion, but without a detectable fusion, who was successfully treated with radiation followed by adjuvant temozolomide.
2. Case Presentation
A 37-year-old female presented to an outside institution with syncope, altered mental status, and visual disturbance (Figure 1). Magnetic resonance imaging (MRI) and computed tomography (CT) demonstrated a 4.3 cm enhancing, diffusion restricting, partially calcified, partially cystic mass involving the tectum, right thalamus, third ventricle, and right lateral ventricle. Severe locoregional mass effect caused brainstem compression and obstructive hydrocephalus (Figure 2). A biopsy was performed with an initial diagnosis of craniopharyngioma. She responded with significant neurologic recovery following shunt placement and was discharged with steroids. The patient subsequently presented to our institution with bilateral lower extremity weakness and gait instability. Neurological examination revealed moon facies and bilateral hip flexor weakness. A brain MRI demonstrated interval tumor progression (Figure 3A,B) and she underwent a craniotomy for tumor debulking of the right thalamic component (Figure 3C,D).
Pathological examination demonstrated a densely cellular neoplasm with elevated mitotic activity and extensive perivascular pseudorosettes (Figure 4). Angulated hyperchromatic nuclei, focal calcifications, and focal myxoid change were present. Necrosis, microvascular proliferation, and oligodendroglioma-like features were not identified within the tissue sections available for histological examination. Olig2 showed strong to moderate immunopositivity in the majority of tumor nuclei (Figure 5B). GFAP was patchy positive with a subset of fragments demonstrating more prominent expression in perivascular regions (Figure 5A). EMA was patchy positive in a strong perinuclear dot-like pattern (Figure 5C). SOX10, synaptophysin, and CAM5.2 were negative. The estimated Ki-67 proliferative index was high (10–30%; Figure 5D). The morphology and intraventricular location bore similarities to supratentorial ependymoma. However, Olig2 positivity in the majority of tumor nuclei raised concern for an alternate diagnosis.
Further investigation with the Mayo Clinic Neuro-Oncology Expanded Gene Panel with Rearrangement revealed EGFR c.1088C>T (p.T363I) (Exon 9) and c.1793G>T (p.G598V) (Exon 15), clinically relevant variants, as well as a BCOR c.626del (p.S209Cfs*7) (Exon 4) variant. Variants of unknown significance were uncovered, including NOTCH1 c.3076G>A (Exon 19), FUBP1 c.263A>T (Exon 4), and MET c.3272C>T (Exon 15). The fusion assay did not detect a BCOR/BCOR(L1) fusion, prompting further analysis with DNA methylation profiling. The composite methylation profile on the Heidelberg classifier versions 11b6 and 12b6 and the NCI/Bethesda classifier versions 2.0 and 3.0 indicated a consensus match to CNS tumor with BCOR/BCOR(L1) fusion. Dimensionality reduction with UMAP (uniform manifold approximation and projection) and t-SNE (t-distributed stochastic neighbor embedding) also placed the tumor into the same class (Figure 6).
She subsequently developed a bilateral upgaze palsy. Her radiation planning brain MRI showed continued tumor progression (Figure 3E,F). Following a multi-disciplinary discussion coupled with lack of any actionable targets on expression profiling, the decision was made to proceed with external beam radiation therapy (59.4 Gy in 33 fractions) followed by six cycles of adjuvant temozolomide 150–200 mg/m^2^. The planning target volume overlapping the brainstem was significant and was prescribed to receive 54 Gy through dose painting to respect brainstem tolerance (Figure 7). The patient tolerated the treatment well, with improvement in her bilateral upwards gaze palsy and headaches within 2 weeks of starting radiation therapy. She completed radiation treatment with Grade 1 fatigue.
Following three cycles of temozolomide, her MRI brain showed response to treatment with significant tumor reduction (Figure 3G,H). Her symptoms resolved, and she remains alive at 11-month follow-up. Ethical guidelines set out by the Declaration of Helsinki were followed in the preparation of this report, and the patient provided written consent.
3. Discussion
The updated WHO classification of CNS tumors improves upon the prior classification schemas by incorporating histologic, molecular, and epigenetic characteristics into an integrated diagnosis [22]. DNA methylation profiling has emerged as an effective means to identify new CNS tumor entities with distinct genetic and epigenetic features within the CNS-PNET group. BCOR-ITD is a newly identified tumor among CNS-PNETs, wherein a match to this methylation class on DNA methylation profiling is an essential criterion for unresolved cases.
BCOR alterations occur in a variety of tumors, including CNS tumors with BCOR/BCOR(L1) fusion, CNS tumors with BCOR-ITD, gliomas, medulloblastomas, and specific sarcomas [3,14,17,23]. CNS tumors with BCOR/BCOR(L1) fusion are characterized by the presence of a BCOR fusion, often paired with EP300 as the typical fusion partner, with or without hallmark CNV within chromosomes 22q12.31 and Xp11.4 [17]. However, CNS tumors without BCOR/BCOR(L1) fusion that instead harbor copy number variations within chromosome Xp11.4 and 22q12.31 or truncating small nucleotide variants can match to the same methylation class as those with BCOR/BCOR(L1) fusion [14,17]. To our knowledge, this is the third reported case of a CNS tumor with BCOR/BCOR(L1) fusion matching the methylation class with a BCOR small nucleotide variant (BCOR c.626del (p.S209Cfs*7) (Exon 4)) instead of a fusion. These cases are exceptionally rare, but share similar molecular characteristics [14]. BCOR deletions hinder PRC1.1 tumor suppressor functioning and incomplete PRC1.1 dysfunction may be sufficiently adequate to promote tumorigenesis [10,24].
CNS tumors with BCOR/BCOR(L1) fusion predominantly occur in adults [14,18,19], consistent with the age of our patient at diagnosis of 37 years. In keeping with the reported radiographic features of CNS tumors with BCOR/BCOR(L1) fusion and predilection for the ventricular region, our patient’s tumor involved the lateral ventricle and demonstrated T1 hypointensity and T2 hyperintensity [17]. These tumors can appear well-demarcated or diffusely infiltrating and with or without enhancement [17,20]. Our patient’s tumor was well-demarcated, enhancing, diffusion-restricting, partially calcified, and partially cystic.
Collectively, the histomorphologic examination of our patient’s tumor corroborates other reported cases of CNS tumors with BCOR/BCOR(L1) fusion, which exhibit diverse histologic findings including oligodendroglial-like chicken-wire vasculature and/or ependymomal-like perivascular pseudorosettes [17,19]. With the exception of supratentorial ZFTA fusion-positive ependymomas which can show patchy Olig2 positivity, extensive Olig2 and patchy GFAP positivity are otherwise atypical in ependymomas [19] and should prompt further consideration for an alternative diagnosis such as CNS tumors with BCOR/BCOR(L1) fusion, as substantiated in our case. Malignant features, including necrosis and elevated mitotic activity are frequently observed in these tumors [19]. Microvascular proliferation is less commonly demonstrated [19]. Our patient’s tumor was highly proliferative with frequent mitotic activity and an estimated Ki-67 ranging from 10–30%. Notably, EMA showed focal strong dot-like perinuclear immunoreactivity, which has not been previously reported in these tumors.
Our patient’s tumor also harbored EGFR p.G598V and p.T363I pathologic variants. In glioblastoma, EGFR p.T363I has been reported in cases of glioblastoma in a single tumor sector [25]. In contrast, EGFR p.G598V is one of the most common extracellular domain missense mutations [26]. EGFR p.G598V is not known to be associated with survival [26]. However, preclinical data suggest that glioblastoma with EGFR missense mutants may be responsive to EGFR kinase inhibitors [27,28,29]. The presence of these EGFR missense mutations in our patient’s tumor may be therapeutically relevant for second-line therapy in the setting of recurrence [26,28]. However, treatment resistance [29] has also been demonstrated in certain cases [28].
In view of the limited evidence on therapies for this extremely rare tumor that matched the methylation class of CNS tumors with BCOR/BCORL1 fusion without a detectable fusion, we reasoned that radiation therapy was warranted given the high proliferative activity. Temozolomide was also selected for its efficacy in CNS tumors with BCOR/BCORL1 fusion and its favorable toxicity profile [16,30,31]. Bevacizumab, carboplatin, ifosfamide, cisplatin, and etoposide also have proven efficacy, but carry greater risks of toxicities [16,19,30] (Table 1).
We acknowledge that several limitations exist in this study. The nature of a single case may not reflect the broader population of CNS tumors with BCOR/BCORL1 fusions in their entirety or those tumors matching to the same methylation class. The short follow-up in our patient limits the understanding of the durability of this treatment regimen and the sustainability of the response to therapy.
Future investigations should be directed at deepening our understanding of the clinical and biological behavior of these tumors. Evidence suggests that these tumors are unique and distinguishable from CNS tumors with BCOR-ITD. Therapeutics represent an open area of investigation, and forthcoming studies should be directed at identifying effective therapies for these tumors. As we cultivate our understanding of CNS tumors with BCOR/BCORL1 fusions, the management for these patients will also continue evolve.
Our case adds to the limited but growing body of evidence for a new CNS tumor type or subtype that may be incorporated into the future WHO classification of CNS tumors. Substantial evidence, including therapeutic options, remains to be uncovered for CNS tumors with BCOR(L1) fusions.
4. Conclusions
A CNS tumor with BCOR/BCOR(L1) fusion is a rare tumor entity, not yet defined in the 2021 WHO classification of CNS tumors. Our case adds to the growing body of evidence for definitive radiation and temozolomide for the treatment of this rare tumor entity.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Louis D.N. Perry A. Wesseling P. Brat D.J. Cree I.A. Figarella-Branger D. Hawkins C. Ng H.K. Pfister S.M. Reifenberger G. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary Neuro Oncol.2021231231125110.1093/neuonc/noab 10634185076 PMC 8328013 · doi ↗ · pubmed ↗
- 2Louis D.N. Wesseling P. Aldape K. Brat D.J. Capper D. Cree I.A. Eberhart C. Figarella-Branger D. Fouladi M. Fuller G.N. c IMPACT-NOW update 6: New entity and diagnostic principle recommendations of the c IMPACT-Utrecht meeting on future CNS tumor classification and grading Brain Pathol.20203084485610.1111/bpa.1283232307792 PMC 8018152 · doi ↗ · pubmed ↗
- 3Sturm D. Orr B.A. Toprak U.H. Hovestadt V. Jones D.T.W. Capper D. Sill M. Buchhalter I. Northcott P.A. Leis I. New Brain Tumor Entities Emerge from Molecular Classification of CNS-PNE Ts Cell 20161641060107210.1016/j.cell.2016.01.01526919435 PMC 5139621 · doi ↗ · pubmed ↗
- 4Astolfi A. Fiore M. Melchionda F. Indio V. Bertuccio S.N. Pession A. BCOR involvement in cancer Epigenomics 20191183585510.2217/epi-2018-019531150281 PMC 6595546 · doi ↗ · pubmed ↗
- 5Huynh K.D. Fischle W. Verdin E. Bardwell V.J. B Co R, a novel corepressor involved in BCL-6 repression Genes. Dev.2000141810182310.1101/gad.14.14.181010898795 PMC 316791 · doi ↗ · pubmed ↗
- 6Gearhart M.D. Corcoran C.M. Wamstad J.A. Bardwell V.J. Polycomb group and SCF ubiquitin ligases are found in a novel BCOR complex that is recruited to BCL 6 targets Mol. Cell Biol.2006266880688910.1128/MCB.00630-0616943429 PMC 1592854 · doi ↗ · pubmed ↗
- 7Junco S.E. Wang R. Gaipa J.C. Taylor A.B. Schirf V. Gearhart M.D. Bardwell V.J. Demeler B. Hart P.J. Kim C.A. Structure of the polycomb group protein PCGF 1 in complex with BCOR reveals basis for binding selectivity of PCGF homologs Structure 20132166567110.1016/j.str.2013.02.01323523425 PMC 4003909 · doi ↗ · pubmed ↗
- 8Choi W.I. Jeon B.N. Yoon J.H. Koh D.I. Kim M.H. Yu M.Y. Lee K.M. Kim Y. Kim K. Hur S.S. The proto-oncoprotein FBI-1 interacts with MBD 3 to recruit the Mi-2/Nu RD-HDAC complex and B Co R and to silence p 21WAF/CDKN 1A by DNA methylation Nucleic Acids Res.2013416403642010.1093/nar/gkt 35923658227 PMC 3711425 · doi ↗ · pubmed ↗