The Angiography Pattern of Buerger’s Disease: Challenges and Recommendations
Bahare Fazeli, Pavel Poredos, Aaron Liew, Edwin Stephen, Abul Hasan Muhammad Bashar, Matija Kozak, Mariella Catalano, Mussaad Mohammaed Al Salman, Louay Altarazi, Pier Luigi Antignani, Sanjay Desai, Evangelos Dimakakos, Dilek Erer, Katalin Farkas, Marcus Fokou, Emad Hussein

TL;DR
This paper discusses the diagnostic criteria for Buerger’s Disease and highlights challenges in identifying its unique angiography patterns.
Contribution
The paper clarifies typical angiography features of Buerger’s Disease and recommends further studies for better differentiation from other vasculitides.
Findings
Segmental occlusion and corkscrew collaterals are key angiography features of Buerger’s Disease.
Differentiating BD from other vasculitides using angiography remains limited due to insufficient data.
Long-term follow-up studies on BD patients are recommended to improve diagnostic accuracy.
Abstract
In 2023, the VAS international working group on Buerger’s Disease (BD) recommended two diagnostic criteria based on a prior Delphi study: “definitive” and “suspected”. The “definitive” criteria are history of smoking, typical angiography, and typical histopathological features. All three features are mandatory to confirm a “definitive” diagnosis of BD. The conundrum is—what features should be considered typical of BD angiography? According to this review, segmental occlusion of infrapopliteal arteries, corkscrew collaterals that appear to continue the occluded arterial segment (Martorell’s sign) or bypass the segmental occlusion, absence of atherosclerotic plaque or aneurysm could differentiate BD from ASO. Hence, for “typical” BD angiography, these manifestations should certainly be considered. However, data for differentiating angiography patterns of BD from the small- and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1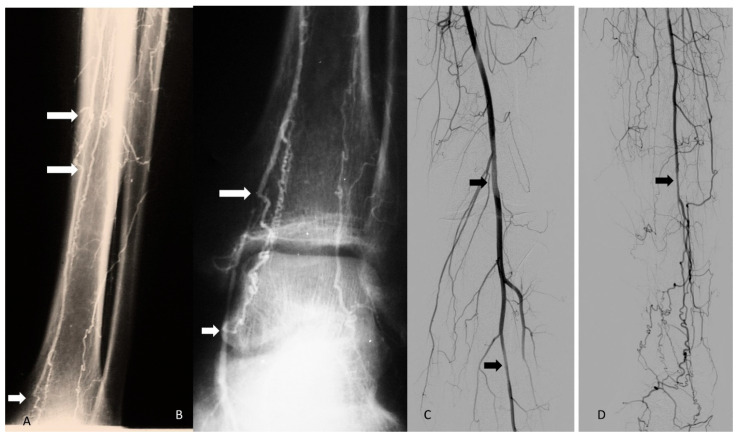 Figure 2
Figure 2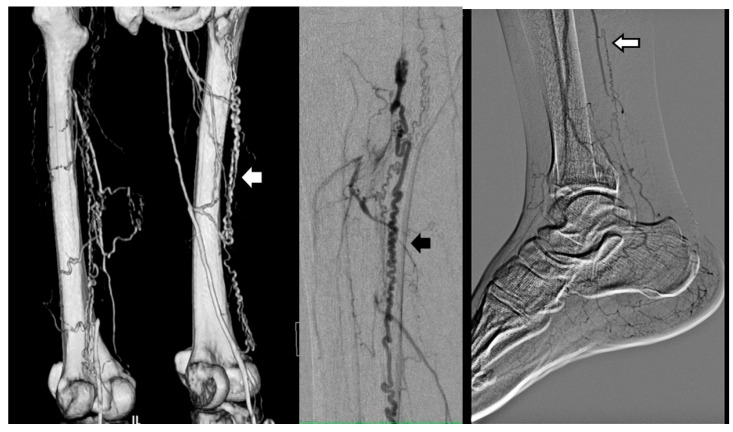 Figure 3
Figure 3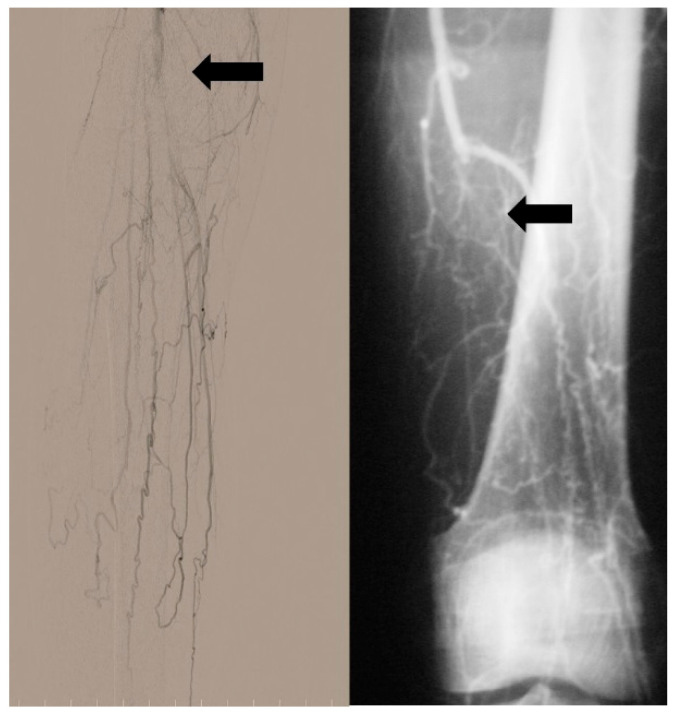 Figure 4
Figure 4 Figure 5
Figure 5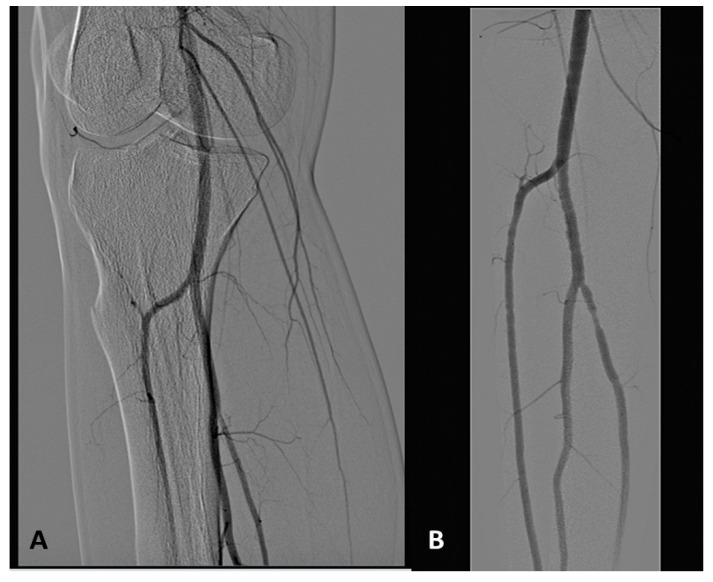 Figure 6
Figure 6 Figure 7
Figure 7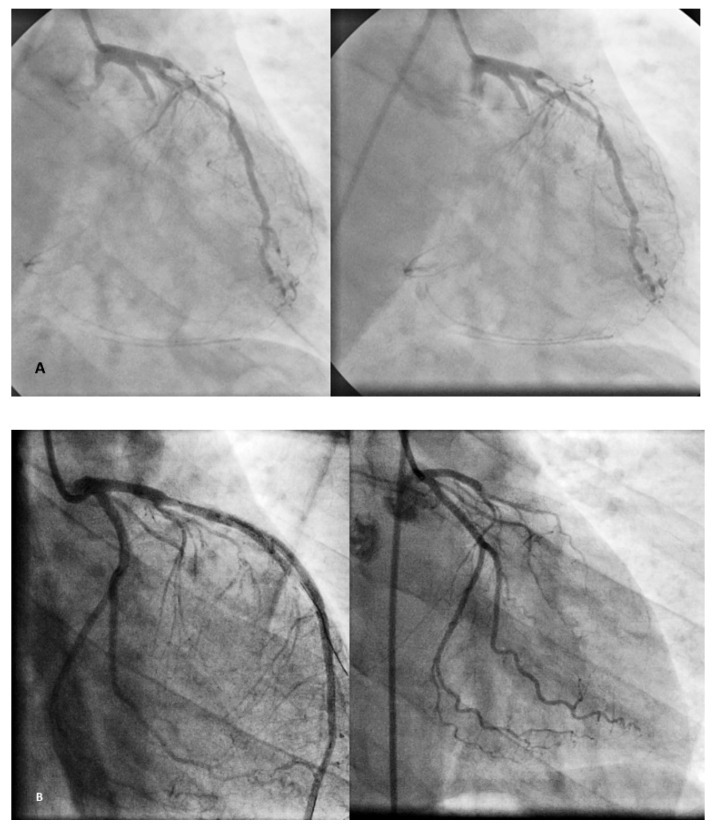 Figure 8
Figure 8Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeripheral Artery Disease Management · Systemic Sclerosis and Related Diseases · Vasculitis and related conditions
1. Introduction
Buerger’s disease (BD) is a relapsing–remitting segmental, inflammatory, thrombotic occlusive, and peripheral vascular disease with unknown etiology which usually involves the medium- and small-sized neurovascular bundle of predominantly young male smokers [1]. Recurring and sharp segmental inflammation and intraluminal thrombus, along with endothelial cell proliferation, may lead to the occlusion of small- to medium-sized arteries in the extremities, causing tissue gangrene or limb loss.
Exacerbation and prognosis of BD have been shown to be closely related to tobacco smoking [1]. However, the etiological role of tobacco smoking in BD development is challenging; because it is unknown why, amongst millions of smokers, only a small number develop BD. It also remains unknown why, of the BD patients who continue smoking, only half of them show aggravation and undergo amputations. Therefore, the exact etiology of BD is unclear [1].
BD has a geographical distribution and it is more prevalent in the Middle East, Far East, Southeast Asia, and Southern America in comparison with Northen America and Western Europe [1]. Notably, the geographical distribution of BD has changed in the past decades and in some countries like Japan, Thailand, and USA, the prevalence of BD has declined without any reasonable changes in the prevalence of smokers [1].
Until recently, there was no definitive biomarker for BD diagnosis due to its unknown etiology. Several diagnostic criteria have been suggested for BD diagnosis [2]. In the countries that BD is more common, the diagnosis is usually made based on clinical features of the disease with or without investigating the common laboratory risk factors for ASO. However, in the regions that BD seems to be a rare disease, the diagnosis is made by ruling out other types of vascular diseases and vasculitis using imaging and specialized laboratory tests.
BD is usually considered a rare disease. Therefore, multi-central studies are very important for better understanding the nature of BD and consequently finding a better approach for BD treatment.
However, before any global studies are conducted, data harmonization among the centers for BD diagnosis is essential. On the other hand, diagnostic criteria that could be acceptable in any region despite the prevalence of BD should be the first step.
In 2023, the international working group on BD of VAS independent foundation in Angiology/Vascular Medicine by 28 countries from different regions recommended two diagnostic criteria based on a prior Delphi study: “definitive” and “suspected”. The “suspected” criteria could be used in daily practice for screening, early diagnosis, and data harmonization on the prevalence or treatment of BD. The “suspected” criteria includes history of tobacco smoking with four out of five findings of disease onset being less than 45 years, ischemic involvement of both lower limbs, ischemic involvement of any of the upper limbs, thrombophlebitis migrans, and Buerger’s color on edematous toes/fingers.
However, the “definitive” diagnosis can be made in a patient with atypical clinical presentation (the age of disease onset being more than 50 years, suffering from diabetes or hyperlipidaemia) or when we want to link a laboratory finding or an unreported clinical presentation to Buerger’s disease. The “definitive” criteria are history of smoking, typical angiography, and typical histopathological features. All three features are mandatory to confirm a diagnosis of BD [3].
Therefore, the next steps of our investigation are what features are the most important and should be considered as typical BD angiography and typical histopathology?
In this review, we evaluate the angiography patterns of lower/upper limbs, and visceral vessels in patients with a BD diagnosis and atypical cases of BD from 1953 to recent times to discuss the main features necessary to confirm a diagnosis of BD based on the frequency of the reported findings.
1.1. Angiography Pattern of Lower Limbs in BD Patients
Leo Buerger attempted to differentiate BD from atherosclerosis obliterans (ASO) in 1953 [1]. Although BD is an inflammatory vascular disease, there are fewer challenges in differentiating BD from other types of vasculitis. Several publications address the conundrum of whether BD is a distinct entity or a premature ASO [4,5,6,7]. Several findings have been addressed in BD angiography since 1953 to date:
- A.Normal aortoiliac and femoropopliteal arteries
Several studies have emphasized the absence of atherosclerotic plaque and aneurysms in proximal arteries in the angiography of BD patients, particularly in the non-affected limb [1,8,9,10]. This absence of atherosclerotic plaque in the involved limb has been found in 90% of the patients with a diagnosis of BD; besides this, abrupt occlusion of the femoropopliteal segment has been found in 40% of the patients in addition to infrapopliteal arterial occlusion [11,12].
The occlusion of iliac arteries in addition to infrapopliteal arterial occlusion (Figure 1) has also been reported in BD patients [13,14,15,16]. BD diagnosis for those patients with atherosclerotic lesions, iliac or femoropopliteal occlusion in arteriography was based on clinical manifestation and histopathology features of arteries harvested from amputees [1,11,12,17].
The literature has questioned the involvement of proximal arteries as being secondary to early stages of atherosclerosis due to the progression of BD OR proximal arteries by intima thickening and inflammatory processes in the wall of the large vessel before complete occlusion [4,5]. However, normal vessels without any irregularities in non-affected limbs of BD patients have been noticed [1,11,12,17].
In short, it has been emphasized that the presence of obliterative lesions in the infrapopliteal arteries, with normal femoral or iliac arteries, is a specific finding of BD. However, the involvement of proximal arteries may not exclude a BD diagnosis.
B.Segmental occlusions
In BD patients, the multi-segment occlusion of the infrapopliteal arteries and veins, so-called “skip lesions”, has been noticed in angiography [13,14,15,16,17,18,19]. Notably, the peroneal artery seems frequently patent, and it is usually involved less severely and less frequently as compared to the anterior tibial and posterior tibial arteries [20,21]. (Figure 2)
Also, segmental vasoconstriction had also been reported, which led to occlusion within two years [22]. Segmental occlusions in the femoropopliteal level appear to be rare [18,23]. Since arterial lesions in ASO are diffuse rather than segmental, this finding has been highlighted to differentiate BD from ASO [4,17,18,23].
C.Collaterals
In 1951, Martorell described direct tortuous small vessels that followed the course of the thrombosed artery without any visualized termination and a no-refill phenomenon of the original vessel in the angiography (Figure 3). He implied that his finding was pathognomonic for BD [1,24,25]. Later, Mckuscik in 1962 emphasized abundant tortuous collaterals in these patients and described them as “corkscrew” and “spider legs” or “tree roots” [26]. In further studies, it was noticed that corkscrew-like collaterals could bypass the segmental occlusions (so-called corkscrew channels) or directly follow the occluded artery (Martorell’s sign). Also several corkscrew-like collaterals beyond the popliteal occlusion (tree roots) usually observed in distal arteries [1,6,12,15,16,17,19,27,28,29,30] (Figure 4).
Several concepts attempting to explain corkscrew formation have been proposed by angiologists, moving away from the categorization of corkscrew collaterals. Some consider tortuous collaterals with large helical signs as corkscrews while some consider only the tortuous collaterals with tiny helical signs [28]. Maybe, that is the reason that some authors consider corkscrews as one of the criteria for BD diagnosis, while others imply that observing corkscrew collaterals alongside the clinical manifestation of the patient and the absence of atherosclerotic plaque in angiography could support BD diagnosis because corkscrews may also be present in diabetes, atherosclerosis, repetitive embolization (Figure 5), scleroderma, and lupus erythematosus [4,31,32,33,34].
In addition to the challenges on the value of corkscrew collaterals in BD diagnosis, corkscrews have been important for a better understanding of BD pathophysiology (from 1962 to 1980). In the past, corkscrews were considered as thrombosis recanalization of the occluded vessel [17,26,27,28]. Suzuki in 1982 emphasized that corkscrews were dilated vasa vasorum of the occluded main artery and not recanalization of its occluded portion [11]. However, Bas reported corkscrew collaterals at the knee level of BD patients to originate from the vasa nervorum of the tibial nerve rather than the vasa vasorum of the occluded popliteal artery [35]. Nowadays, Martorell’s sign is losing its significance.
D.Vasospasm
Diffuse arterial narrowing and generalized vasospasm have been observed in about 15% of angiography in BD patients [11,12,36] (Figure 5). Segmental vasoconstriction of the arteries about two years before their occlusion has been reported [37]. Most authors believe that circular vasoconstriction has been induced by irritation from the contrast medium. However, Kohler implied that this appearance might be due to diffuse intimal thickenings and not the consequence of vasoconstriction [38].
Moreover, several ring-like circular segments of stenosis, like goose trachea in the process of arteriography during the 1960s and 1970s were reported and the sensitivity of the arteries of BD patients to the catheter was addressed as its reason (Figure 6). Since goose trachea appearance has been rarely reported in ASO, it was concluded that the arteries of BD patients are more sensitive to stimuli than ASO patients [3,4,8,14].
E.Early venous opacification
Early venous opacification seen on angiography in about 20% of BD patients is attributed to arteriovenous shunting in a few studies [11,12].
1.2. Phlebography of Lower Limbs in BD Patients:
In 1976, Chopra evaluated the phlebography of this subset and reported segmental occlusion of major deep veins, diffusely narrow small veins, collaterals, and irregular tortuosity of the veins [39].
1.3. Angiography Pattern of Upper Limbs of BD Patients:
The most commonly reported findings are occlusions of the ulnar or radial artery, or both, at or above the wrist, tortuous collaterals, but not corkscrews, in particular around the wrist and interphalangeal joints (Figure 7) without any evidence of atherosclerotic plaque [7,12,40,41,42,43].
1.4. BD Diagnosis According to Angiography in Atypical Cases:
Atypical cases of BD are usually individuals with risk factors of ASO (age > 50 years, diabetes, and dyslipidaemia) or in non-smokers. Absence of atherosclerotic plaque in the proximal arteries, abrupt occlusion, segmental occlusions of infrapopliteal arteries, and tree-root collaterals (but not corkscrews) are the most common findings seen on the angiography of such cases [44,45,46,47,48,49,50,51].
1.5. Angiography Pattern of Visceral Vessels in the Patients with Previous BD Diagnosis:
According to the case reports of visceral involvement in BD patients, the angiography pattern of visceral vessels is usually not as typical as that of the lower extremities’ corkscrew collaterals around the occluded vessel with less tortuosity compared to the lower extremities, and abrupt occlusion of the mesenteric or coronary arteries has been reported without any evidence of atherosclerosis. In most of the case reports, stenosis, multiple filling defects or total occlusion of the involved artery without corkscrew collaterals (Figure 8) have been noticed [6,15,18,22,52,53,54]. Therefore, differentiating BD from ASO according to such stenosis appears very difficult and in many cases such stenosis was considered as due to atherosclerotic plaque. In particular, atherosclerotic lesions of the visceral vessels have been identified via the autopsy of the patients with BD diagnosis [4,6,18]. Interestingly, Hong et al. in 2005 demonstrated that the stenosis of the coronary artery of a BD patient completely resolved in the follow-up angiography after two months without any intervention [51].
2. Discussion
There is no consensus on whether the angiography pattern of BD is diagnostic [55]. Some authors have implied that the angiographic patterns of BD are non-pathognomonic; they have concluded that the diagnosis should be established alongside the clinical course of the patient [31,32,33]. However, based on this concept, BD diagnosis in patients with atypical clinical presentations would be challenging.
The next challenge is the definition of “typical” angiographic pattern for BD patients. For years, the typical BD angiographic pattern has been described as normal-proximal arterial structure, absence of atherosclerotic plaque, lack of aneurysm, infrapopliteal arterial occlusion, corkscrew collaterals, and skip lesions [1,8,9,10]. However, the duration between the disease onset and performing the angiography could influence the pattern(s) seen. For instance, corkscrew collaterals may not be completely developed in the early manifestation of the disease [28,29,30,31,32,33]; in a patient suffering from BD for years, the involvement of femoropopliteal arteries or even atherosclerotic plaques in the affected limb could be observed [1,11,12,13,14].
Unfortunately, the literature about angiographic patterns in early presentation of BD or in patients with long-term suffering from the disease are limited. Therefore, we need a functional or mechanistic explanation of the angiographic pattern of BD alongside the statistical data from different studies to be able to define “typical” angiographic pattern.
Segmental occlusions of the infrapopliteal arteries, so-called “skip lesions”, have been reported in BD [1]. In 1984, Hagen reported multiple segmental involvement of infrapopliteal arteries in all his 44 patients [12]. This appears to be due to segmental intima thickening or segmental scar tissue surrounding the infrapopliteal arteries. Notably, segmental vasoconstriction of the arteries about two years before their occlusion has been noticed [22]. Multiple occlusions in diabetic patients suffering from ASO, but not the segmental occlusions, have been observed [13,14,15,16,17,19].
Corkscrew collaterals in BD are usually less than 1.5 mm and they follow the course of the original vessel without refilling the vessel (Martorell’s sign) or they bypass the segmental occlusions of infrapopliteal arteries. Corkscrew collaterals have also been reported in ASO. However, in ASO, the small corkscrew collaterals (less than 1.5 mm) have been observed around patent arteries [1,28].
Diffuse arterial narrowing and generalized vasospasm have been observed in about 15% of the angiography of BD patients, which might be due to inflammation of sympathetic ganglia [11,12,36]. However, we could not find any report of generalized vasospasm in ASO. Therefore, generalized vasospasm could be supportive of a BD diagnosis.
According to this review, atherosclerotic plaque has been reported in about 10% of the angiography of BD patients when their disease had been confirmed by histopathology of arterial lesions [11,12]. Therefore, absence of atherosclerotic plaque would be supportive for BD diagnosis but the existence of atherosclerotic plaque alongside clinical and other arteriography features of BD would not exclude it.
Although abrupt occlusion has been emphasized as one of the characteristics of BD angiography, it depends on the stage of the disease. Also, this feature could also be observed due to arterial emboli [11,12].
An aneurysm in the peripheral arteries of the lower limbs has been reported in only one case report according to our literature review [54]. The absence of an aneurysm could be supported by the intact internal elastic lamina of vascular wall in BD histopathology [1,8]. Therefore, the absence of an aneurysm is supportive for BD diagnosis.
3. Conclusions
Until recently, ASO has been the prominent differential diagnosis of BD. Such an attempt to differentiate BD from ASO might be due to different treatment approaches of these peripheral vascular diseases. For instance, ASO patients usually benefit more from angioplasty procedures and statins than BD patients. Also, ASO could be predictable in patients with risk factors of atherosclerotic plaque formation. The atherosclerotic risk factors could also be controlled more appropriately for preventing or managing ASO. However, a small number of smokers might develop BD and complete smoking cessation for heavy smokers is not an easy process.
Usually for BD diagnosis, the typical clinical presentation of BD alongside ruling out the presence of atherosclerotic plaque by either imaging such as duplex or CT angiography has appeared enough [18,56,57].
However, in BD cases with risk factors of atherosclerosis but not smoking, a typical angiography could be helpful for differentiating BD from ASO.
According to this review, segmental occlusion of infrapopliteal arteries, corkscrew collaterals that appear to continue the occluded arterial segment (Martorell’s sign) or bypass the segmental occlusion, absence of atherosclerotic plaque or an aneurysm could differentiate BD from ASO. Hence, for “typical” BD angiography, these manifestations should certainly be considered.
This “typical” BD angiography has been suggested based on the frequency of angiography findings in the literature from 1953 to recently, and it received the consensus of the VAS BD working group.
However, according to this review, there are some more points that should be considered.
First of all, atherosclerotic plaque in the affected limb of a BD patient, in particular in the patients with long-term clinical manifestation of BD might not rule out a BD diagnosis.
Moreover, most of the studies about BD angiographic pattern were conducted on the patients who had been reported to have critical limb ischemia. There are a lack of studies about BD angiographic patterns in early clinical presentation of BD. Perhaps, investigating the angiography pattern in early and late presentation of BD, particularly in the patients with long-term follow up could help us in better understanding BD pathophysiology.
Although BD is an inflammatory vascular disease, small- and medium-sized vasculitis are less considered as the differential diagnosis of BD. Unfortunately, data for differentiating the angiography pattern of BD from small- and medium-sized vasculitis including Behcet’s disease, scleroderma, hepatitis associated vasculitis, and anti-phospholipid syndrome are limited.
All these lacunae and queries leave room for ongoing research and need for collaborative efforts by treating physicians/surgeons/angiologists all over the world, especially from regions where the disease is more frequently seen.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fazeli B. Poredos P. Patel M. Klein-Weigel P. Catalano M. Stephen E. AL Salman M.M. Altarazi L. Bashar A.H. Chua B. Milestones in thromboangiitis obliterans: A position paper of the VAS-European independent foundation in angiology/vascular medicine Int. Angiol.20214039540810.23736/S 0392-9590.21.04712-X 34236154 · doi ↗ · pubmed ↗
- 2Fazeli B. Ligi D. Keramat S. Maniscalco R. Sharebiani H. Mannello F. Recent Updates and Advances in Winiwarter-Buerger Disease (Thromboangiitis Obliterans): Biomolecular Mechanisms, Diagnostics and Clinical Consequences Diagnostics 202111173610.3390/diagnostics 1110173634679434 PMC 8535045 · doi ↗ · pubmed ↗
- 3Fazeli B. Poredos P. Kozak M. Pecsvarady Z. Catalano M. AL Salman M.M. Altarazi L. Ali A.A. Bashar A.H. Bozkurt K. Diagnostic criteria for Buerger’s disease: International Consensus of VAS—European Independent Foundation in Angiology/Vascular Medicine Int. Angiol.20234239640110.23736/S 0392-9590.23.05098-838010012 · doi ↗ · pubmed ↗
- 4Wessler S. Buerger’s disease revisited Surg. Clin. N. Am.19694970371310.1016/S 0039-6109(16)38862-44890183 · doi ↗ · pubmed ↗
- 5Wessler S. Ming S.C. Gurewich V. Freiman D.G. A critical evaluation of thromboangiitis obliterans. The case against Buerger’s disease N. Engl. J. Med.19602621149116010.1056/NEJM 19600609262230113844117 · doi ↗ · pubmed ↗
- 6Schatz I.J. Fine G. Eyler W.R. Thromboangiitis obliterans Br. Heart J.196628849110.1136/hrt.28.1.845904753 PMC 459043 · doi ↗ · pubmed ↗
- 7Iwai T. Kume H. Koizumi S. Sakurazawa K. Honma K. Ogasawara H. Takemura T. Kishino M. Kagayama T. Buerger Disease: Pathological Changes in Elderly Patients Ann. Vasc. Dis.202215293610.3400/avd.oa.21-0014235432646 PMC 8958396 · doi ↗ · pubmed ↗
- 8Olin J.W. Thromboangiitis obliterans (Buerger’s disease)N. Engl. J. Med.200034386486910.1056/NEJM 20000921343120710995867 · doi ↗ · pubmed ↗