No-Touch Aorta Off-Pump LIMA-Radial Artery Y-Graft CABG as a Safe Strategy for All-Comers: Long-Term Survival
Tomasz Plonek, Dominik Mendyka, Frank R. Halfwerk

TL;DR
This study shows that a specific heart bypass surgery technique is safe and effective for a wide range of patients, including older individuals.
Contribution
The study demonstrates the long-term safety and effectiveness of a no-touch aorta, total arterial off-pump CABG technique for all-comers.
Findings
In-hospital mortality was 0.6% with no significant differences across age groups.
Five-year survival was 90% overall, with the youngest group having 98% and the oldest 65%.
The mean number of grafts per patient was 3.7, consistent across age groups.
Abstract
Objectives: To assess the long-term survival outcomes of patients undergoing no-touch aorta, total arterial off-pump coronary artery bypass grafting (OPCAB) using a left internal mammary artery (LIMA)–radial artery (RA) Y-graft configuration. This approach was applied uniformly to all-comers undergoing isolated CABG between 2004 and 2021, irrespective of preoperative risk profile. Methods: We included all patients treated with total arterial OPCAB using the LIMA–RA Y-graft without additional concomitant procedures. Patients were stratified into five age groups (<50, 50–59, 60–69, 70–79, and >80 years). Survival at 5 years was analyzed using Kaplan–Meier curves and Cox regression analysis. Results: A total of 2174 patients were analyzed, with a median follow-up of 3266 days. In-hospital mortality was 0.6%, whereas postoperative stroke was 0.3% without residual trauma and 0.2% with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
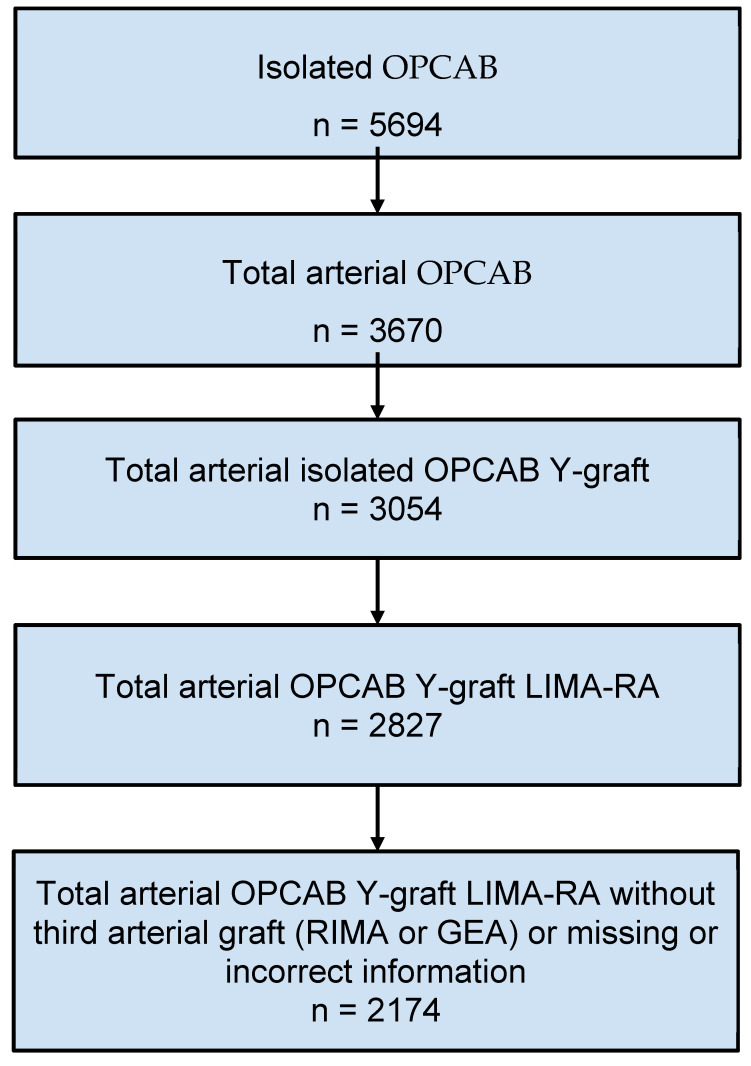 Figure 1
Figure 1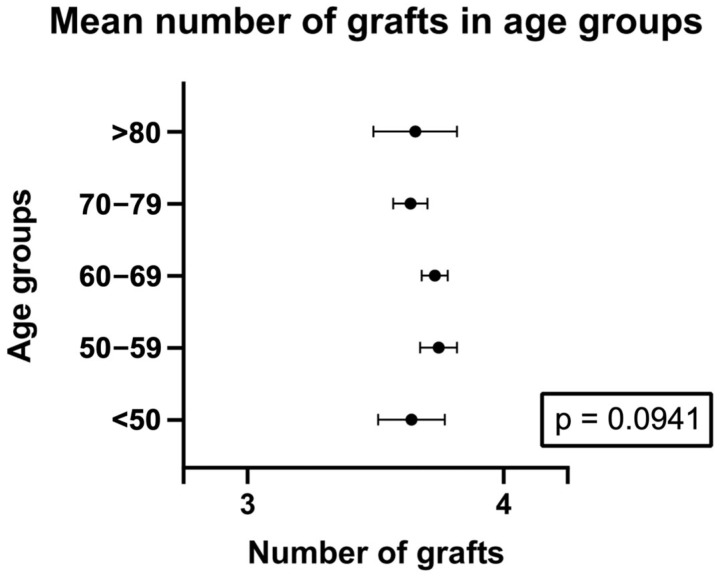 Figure 2
Figure 2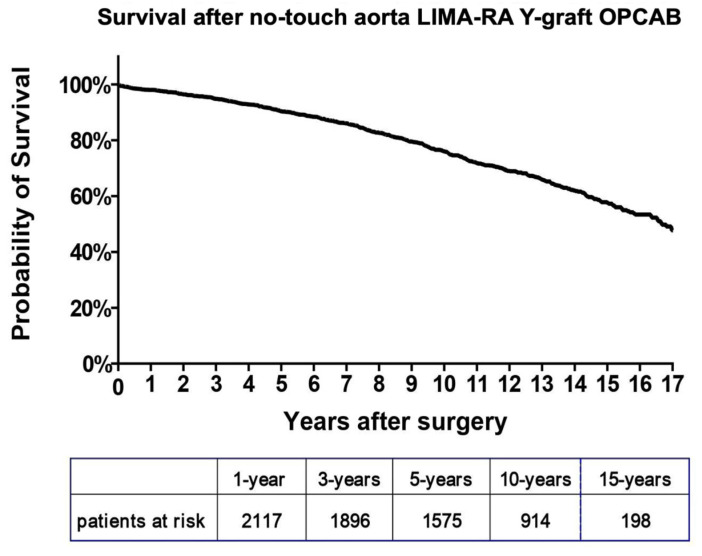 Figure 3
Figure 3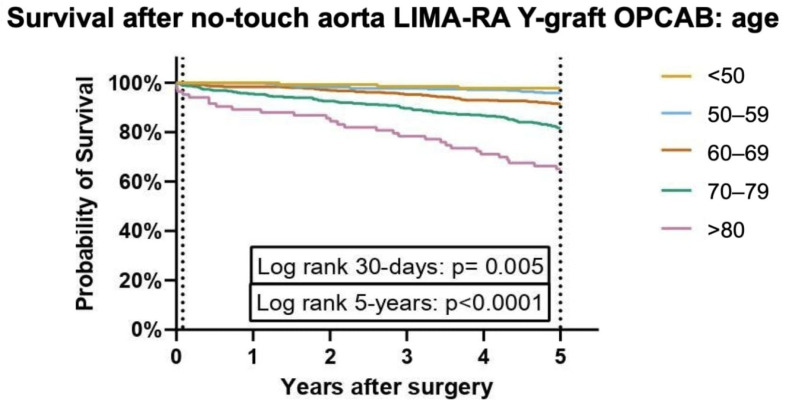 Figure 4
Figure 4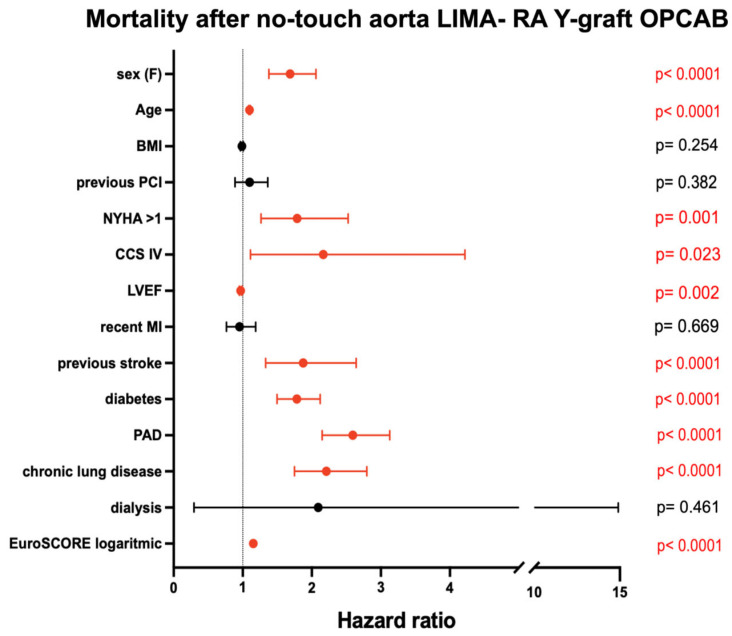 Figure 5
Figure 5- —Cardiac Research at Thoraxcentrum Twente
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac and Coronary Surgery Techniques · Aortic aneurysm repair treatments · Aortic Disease and Treatment Approaches
1. Introduction
Coronary artery bypass grafting (CABG) can be performed either with cardiopulmonary bypass (on-pump CABG) or without it (off-pump CABG, OPCAB), using various vascular graft configurations. The optimal surgical technique remains a matter of ongoing debate. According to the 2018 ESC/EACTS guidelines on myocardial revascularization, OPCAB offers particular advantages in patients with severe calcification of the ascending aorta [1]. However, randomized controlled trials to date have not demonstrated a clear superiority of off-pump over on-pump CABG. This controversy is partly fueled by concerns over methodological limitations in these trials, notably the inclusion of surgeons with relatively limited off-pump experience [2]. Moreover, one of the major advantages of OPCAB—the no-touch or anaortic technique—was not specifically evaluated in these trials. Later evidence has shown that no-touch aortic strategies can reduce the risk of postoperative stroke by nearly 60% compared to techniques using aortic side clamps [3,4].
There is broad consensus that the left internal mammary artery (LIMA) is the gold standard graft for CABG [1,5,6]. In multivessel disease, additional grafts are required, most commonly the saphenous vein, right internal mammary artery (RIMA), or radial artery (RA). For patients with high-grade coronary stenoses, current guidelines recommend complete arterial revascularization. The RA is believed to be particularly suitable for vessels with high-grade proximal stenosis, limited competitive flow, and for revascularization within the left coronary territory [1].
In our practice, the RA is the preferred second conduit because of its adequate length, durability, excellent long-term patency, and the advantage of simultaneous harvesting with the LIMA. In contrast, the RIMA is often too short to reach the right coronary artery branches, particularly in patients with dilated ventricles, and is more fragile. Furthermore, the use of bilateral internal mammary arteries has been associated with an increased risk of sternal wound complications, as reported in the ART trial [7].
Since its inception in 2004, our center has adopted the off-pump LIMA–RA Y-graft with a no-touch aortic strategy as the standard revascularization approach for all patients, irrespective of age, coronary anatomy, or the presence of left main disease—that is, for “all-comers.” The aim of this study is to present the short- and long-term outcomes of our 17-year experience with no-touch aorta OPCAB using the LIMA–RA Y-graft configuration.
2. Materials and Methods
This retrospective, single-center study included patients who underwent isolated off-pump coronary artery bypass grafting (OPCAB) with a no-touch aorta LIMA–radial artery (RA) Y-graft at Thorax Centrum Twente, Enschede, The Netherlands, between September 2004 and October 2021. The study adhered to the STROBE guidelines for observational research [8]. Patients who underwent surgery using cardiopulmonary bypass, underwent concomitant non-revascularisation related interventions, received venous or RIMA grafts, or those who had undergone previous cardiac surgeries were excluded from the analysis. Radial artery grafts were routinely harvested endoscopically [9].
The study was exempted from the Medical Research Involving Human Subjects Act by the Institutional Review Board of Medisch Spectrum Twente (K22-33), with a waiver for informed consent.
Baseline and procedural data were extracted from electronic patient records, and risk stratification was based on EuroSCORE I, EuroSCORE II, and Netherlands Heart Registration definitions [10]. Given the study’s “all-comer” design, selection bias was minimized, enhancing the generalizability of the findings. No formal sample size calculation was performed.
The primary endpoint was to assess short- and long-term survival, specifically 30-day and late survival rates. The secondary endpoint involved identifying hazard factors associated with postoperative 5-year survival, as well as conducting age-stratified survival analyses (categorized as <50 years, 50–59 years, 60–69 years, 70–79 years, and ≥80 years).
2.1. Surgical Technique
All procedures were performed via median sternotomy. The LIMA was harvested under direct vision using electrocoagulation, and the RA was harvested using an endoscopic technique. Distal anastomoses were completed with the aid of suction stabilization devices. Postoperatively, all patients received calcium-channel blockers, such as amlodipine, to prevent radial artery spasm, and single or dual antiplatelet therapy depending on the guidelines applicable at the time.
2.2. Statistical Analysis
Continuous variables were assessed for normal distribution using skewness/kurtosis measures and visual inspection of histograms. Normally distributed continuous variables are presented as means ± standard deviation, while non-normally distributed variables are reported as medians with interquartile ranges (25th–75th percentiles). Categorical variables were analyzed using the Fisher Exact test, and Chi-squared tests were employed where necessary due to hardware limitations. The Kruskal–Wallis test was applied to compare ordinal and non-parametric continuous variables across age groups, while one-way ANOVA was used for comparisons of normally distributed continuous variables.
Kaplan–Meier analysis and the log-rank test were used to evaluate survival times for the primary endpoint. For secondary analyses, hazard ratios (HR) were calculated using Cox regression models to determine factors associated with postoperative survival. Proportional hazards assumptions for the Cox regression model were assessed using Schoenfeld residuals. Age-stratified analyses were conducted for groups categorized by decades (<50, 50–59, 60–69, 70–79, and ≥80 years). Missing data were not imputed. Several important clinical variables had substantial proportions of missing data, including NYHA class (available in 848 of 2174 cases), EuroSCORE II (1153/2174), and preoperative serum creatinine level (800/2174).
Statistical significance was set at p < 0.05.
3. Results
A total of 2174 patients underwent total arterial OPCAB with LIMA–RA Y-graft without any concomitant intervention (Figure 1). A total of 392 patients were excluded due to non-physiological values (e.g., implausible follow-up times or age due to entry errors) recorded in the database or lack of follow-up data. The median follow-up time for survival was 3266 days.
The mean age of the population was 65 ± 9.3 years, ranging from 36 to 87 years, with 85% of patients being male. Surgery was elective in 41% of patients, urgent in 58%, and emergent or salvage in 1%. All baseline characteristics are provided in Table 1 and Supplementary Table S1. In general, comorbidities increased with age. Survival follow-up was available for 99% of patients, with 13 patients lost to follow-up.
On average, 3.7 ± 0.79 distal arterial anastomoses were performed (Table 2, Figure 2). No differences in the number of anastomoses were observed between age groups. Notably, 58% of patients received four or more arterial anastomoses (Supplementary Table S3).
3.1. Survival
In-hospital mortality was 0.6%. Postoperative stroke without residual deficit occurred in 0.3% of patients and stroke with residual deficit in 0.2%, with no significant differences between age groups (Table 3, Supplementary Table S2).
The primary endpoint, 30-day survival, was 99%, and survival at five years was 90% (Figure 3, Supplementary Table S4).
3.2. Survival per Age Group
A statistically significant difference in survival probability was observed between age groups, with older patients showing progressively lower survival curves (Figure 4). Survival probabilities by group are presented in Supplementary Table S4. Mortality rates increase progressively with age across multiple time intervals, with the highest rates consistently observed in the >80 age group. At 30 days, mortality is lowest in the <50 years group (0%) and gradually increases with age, reaching 3.4% in the >80 group (p = 0.005). By 1 year, the >80 group exhibits the highest mortality rate at 7.8% (p < 0.001). This trend continues, with the >80 age group demonstrating the highest mortality at each follow-up. At 3 years, 17.8% of individuals in the >80 group have died, compared to just 1.5% in the <50 group. At 5 years, 34.9% of the >80 group has died, compared to just 2.3% in the <50 group. The gap widens further at 10 years, where 84.1% of individuals over 80 have died, compared to only 10.7% in the <50 group. By 15 years, the >80 group has a 100% mortality rate, while the <50 group remains significantly lower at 42.9%. Detailed data on these mortality rates across the different age groups and time intervals are presented in Supplementary Table S3.
3.3. Mortality Predictors After No-Touch Aorta LIMA–RA Total Arterial OPCAB
Cox regression hazard ratio analysis identified several significant predictors of mortality after no-touch aorta LIMA–RA total arterial OPCAB (Figure 5). Female sex, older age, NYHA class > 1, CCS class IV, reduced left ventricular ejection fraction (LVEF), previous stroke, diabetes, peripheral artery disease (PAD), chronic lung disease, and higher EuroSCORE were all significantly associated with increased mortality (all p < 0.05). In contrast, body mass index (BMI), previous percutaneous coronary intervention (PCI), recent myocardial infarction (MI), and dialysis were not significantly associated with mortality.
4. Discussion
This study demonstrates that total arterial off-pump coronary artery bypass grafting (OPCAB) using the LIMA–RA Y-graft technique is a safe and effective revascularization strategy, offering excellent early and long-term outcomes across a broad patient population. In a large, single-center cohort of 2174 patients, we observed remarkably low in-hospital mortality (0.6%) and a minimal incidence of postoperative stroke, with consistent results across age groups. Thirty-day survival reached 99%, and five-year survival was 90%, confirming the durability and safety of this approach. These findings reinforce the benefits of total arterial grafting and suggest that, when performed in experienced hands, OPCAB can be applied widely without compromising outcomes, even in elderly or high-risk patients. The short- and mid-term mortality in our cohort was better than those reported in the landmark ART randomized controlled trial [7], 0.6 vs. 1.2% at 30 days and 10% vs. 12.2–12.7% at 5 years.
We deliberately excluded patients who received a third arterial graft (e.g., RIMA or GEA) or a venous graft in order to minimize the confounding influence of known additional morbidities associated with these conduits, such as mediastinitis with bilateral internal mammary artery use, abdominal complications with GEA, or wound issues with saphenous vein grafts. Instead, we focused the analysis on outcomes associated with our preferred strategy: the LIMA–RA Y-graft configuration.
However, as expected, there was a clear age-dependent trend in long-term survival. Patients in older age groups had progressively lower survival rates at each follow-up interval. While the <50 years group had a near-zero mortality rate at 30 days, the >80 years group experienced a significantly higher mortality rate, starting at 3.4% at 30 days and escalating to 100% by 15 years. These findings are consistent with previous studies demonstrating that advancing age is one of the most robust predictors of mortality after coronary artery bypass grafting (CABG) [11,12]. However, it seems obvious that long-term survival in octogenarians is expected to be low and not necessarily attributed to coronary artery disease. These patients still benefit from low short-term mortality and a low risk of a devastating complication of postoperative stroke.
Age-related mortality differences observed in this study align with the results from the Cox regression hazard ratio analysis, which identified older age, female sex, poor functional status (NYHA class > 1, CCS class IV), comorbidities such as diabetes and peripheral artery disease (PAD), and a reduced left ventricular ejection fraction (LVEF) as significant predictors of mortality. These factors have been widely recognized as risk factors for poor long-term outcomes in CABG patients and emphasize the importance of a comprehensive preoperative assessment to identify high-risk individuals [13,14]. Interestingly, factors such as body mass index (BMI), previous percutaneous coronary intervention (PCI), recent myocardial infarction (MI), and dialysis were not found to be significantly associated with mortality in this cohort, which may suggest that the benefits of total arterial grafting are not attenuated by these conditions.
In terms of surgical technique, the use of total arterial grafting, specifically the LIMA–RA Y-graft, remains associated with favorable long-term outcomes, even in older patients. The LIMA graft, in particular, is known for its long-term patency and is considered the gold standard in coronary artery bypass surgery [1].
In experienced centers, off-pump coronary artery bypass (OPCAB) can be safely performed in all patients regardless of age or left ventricular function. The key is surgical expertise and performing OPCAB routinely in all patients. We occasionally use an intraaortic balloon pump or extracorporeal circulation (ECC-assisted CABG) in hemodynamically very unstable patients.
Importantly, this approach allows for extensive revascularization. In our cohort, the mean number of distal anastomoses was 3.7 per patient (58% of patients receiving four or more arterial anastomoses), demonstrating that no-touch total arterial OPCAB does not have to compromise the “completeness” of the revascularisation, especially in experienced hands.
These findings support the use of no-touch aorta, total arterial OPCAB as a universally effective revascularization strategy. Particularly in older patients, the technique offers excellent short-term outcomes with remarkably low perioperative stroke rates—a critical factor in this high-risk population. The approach demonstrates safety and efficacy across all age groups, making it an attractive default strategy rather than one limited to selected cases.
This study has several limitations inherent to its retrospective and single-center design. Although the large cohort and standardized surgical technique strengthen the findings, the absence of a control group (e.g., on-pump or hybrid CABG patients) limits direct comparisons. As such, it does not allow for definitive conclusions regarding the superiority or equivalence of the no-touch aorta LIMA–RA Y-graft OPCAB technique relative to on-pump CABG or alternative revascularization strategies. While this limits comparative inference, the strength of the study lies in its large, unselected patient cohort and consistent application of a standardized surgical technique over a 17-year period. The findings should be interpreted as real-world outcome data from a high-volume center with extensive experience in total arterial OPCAB. These results must be interpreted with caution and may not be generalizable or reproducible in centers with limited experience in this surgical approach. Furthermore, data on certain postoperative variables, such as neurocognitive outcomes and long-term quality of life, were not systematically collected. The all-comers strategy improves generalizability, but selection bias cannot be entirely excluded due to the exclusion of patients with missing graft data. Finally, while long-term survival was robustly analyzed, cause-specific mortality was not available for most patients, which limits interpretation of graft-related vs. non-cardiac death over time. It may have had an impact on the results, especially in the elderly, frail, and multi-morbid patients. Moreover, the data on the history of smoking, dyslipidemia, or hypertension were not reliably reported and thus not presented and analyzed in this study.
In conclusion, no-touch aorta, total arterial OPCAB using the LIMA–RA Y-graft performed in a high-volume off-pump coronary artery bypass grafting center is a safe and effective revascularization strategy for a broad spectrum of patients, including those with advanced age and comorbidities. However, we underline the importance of establishing a structured OPCAB program to perform it safely in all patient groups.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Neumann F.J. Sousa-Uva M. Ahlsson A. Alfonso F. Banning A.P. Benedetto U. Henderson R. 2018 ESC/EACTS Guidelines on myocardial revascularization Eur. Heart J.20194087165 Erratum in Eur. Heart J. 2019, 40, 3096. https://doi.org/10.1093/eurheartj/ehy 39410.1093/eurheartj/ehz 507 · doi ↗
- 2Puskas J.D. Gaudino M. Taggart D.P. Experience Is Crucial in Off-Pump Coronary Artery Bypass Grafting Circulation 20191391872187510.1161/CIRCULATIONAHA.119.03958430986108 · doi ↗ · pubmed ↗
- 3Wang C. Jiang Y. Jiang X. Chen S. On-pump beating heart versus conventional on-pump coronary artery bypass grafting on clinical outcomes: A meta-analysis J. Thorac. Dis.2021134169418410.21037/jtd-21-56834422346 PMC 8339771 · doi ↗ · pubmed ↗
- 4Pawliszak W. Kowalewski M. Raffa G.M. Malvindi P.G. Kowalkowska M.E. Szwed K.A. Borkowska A. Kowalewski J. Anisimowicz L. Cerebrovascular Events After No-Touch Off-Pump Coronary Artery Bypass Grafting, Conventional Side-Clamp Off-Pump Coronary Artery Bypass, and Proximal Anastomotic Devices: A Meta-Analysis J. Am. Heart Assoc.20165 e 00280210.1161/JAHA.115.00280226892526 PMC 4802438 · doi ↗ · pubmed ↗
- 5Schmitto J.D. Rajab T.K. Cohn L.H. Prevalence and variability of internal mammary graft use in contemporary multivessel coronary artery bypass graft Curr. Opin. Cardiol.20102560961210.1097/HCO.0b 013e 32833 f 049820881486 · doi ↗ · pubmed ↗
- 6Flather M. Dimagli A. Benedetto U. Lees B. Gray A. Gerry S. Naik A. Cook J. Gaudino M. Little M. Bilateral Versus Single Internal Thoracic Coronary Artery Bypass Grafting: The ART RCT National Institute for Health and Care Research Southampton, UK 202337931047 · pubmed ↗
- 7Andenbroucke J.P. von Elm E. Altman D.G. Gøtzsche P.C. Mulrow C.D. Pocock S.J. Poole C. Schlesselman J.J. Egger M. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration Epidemiology 20071880583510.1097/EDE.0b 013e 318157751118049195 · doi ↗ · pubmed ↗
- 8Sandker S.C. Mecozzi G. van Buiten A. Mariani M.A. Buikema H. Grandjean J.G. Adventitial dissection: A simple and effective way to reduce radial artery spasm in coronary bypass surgery Interact. Cardiovasc. Thorac. Surg.20131778478910.1093/icvts/ivt 31223883477 PMC 3805201 · doi ↗ · pubmed ↗