Interpupillary Distance and Peripapillary Myopic Changes: A Pilot Study in a Glaucomatous Cohort
Sameer Butt, Adèle Ehongo

TL;DR
This study investigates whether interpupillary distance affects myopic changes around the optic nerve in glaucoma patients, finding no significant link.
Contribution
The study is the first to explore the relationship between interpupillary distance and peripapillary myopic changes in a glaucomatous cohort.
Findings
Interpupillary distance showed no significant correlation with optic disc ovality or gamma peripapillary atrophy width.
Axial length was strongly correlated with optic disc ovality and gamma peripapillary atrophy.
Biomechanical forces from interpupillary distance do not appear to influence optic nerve head remodeling in myopia.
Abstract
Background/Objectives: Myopia is associated with peripapillary changes, namely, gamma peripapillary atrophy (γPPA) and optic disc ovalization, estimated by the ovality index (OI). These changes have been suggested to be promoted by adduction. Recent studies highlight that near reading significantly contributes to the development and progression of myopia and that the interpupillary distance (IPD) influences vergence amplitudes. While both adduction and convergence are involved during near reading, a potential link between IPD and myopic peripapillary changes has not yet been explored. We, therefore, sought to determine whether IPD is related to the OI or γPPA width. Methods: In this monocentric cross-sectional study, 100 eyes from 100 adults (mean age of 62.6 ± 13.7 years) were analyzed. Axial length (AL), refractive error, and IPD were recorded. The OI and γPPA width were assessed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
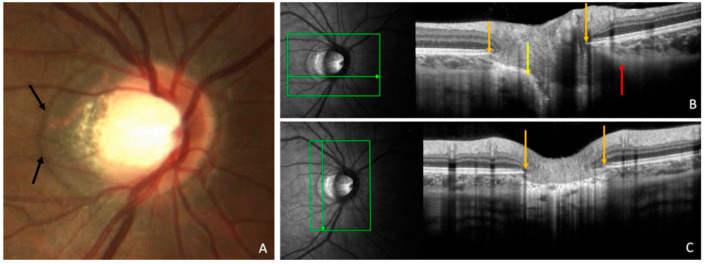 Figure 1
Figure 1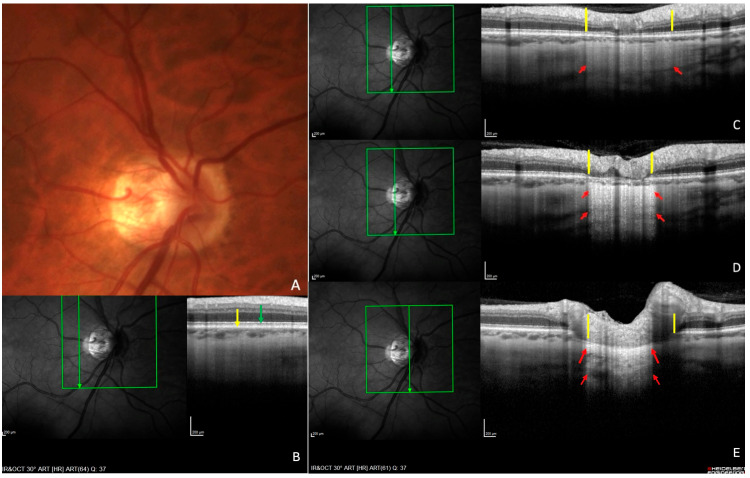 Figure 2
Figure 2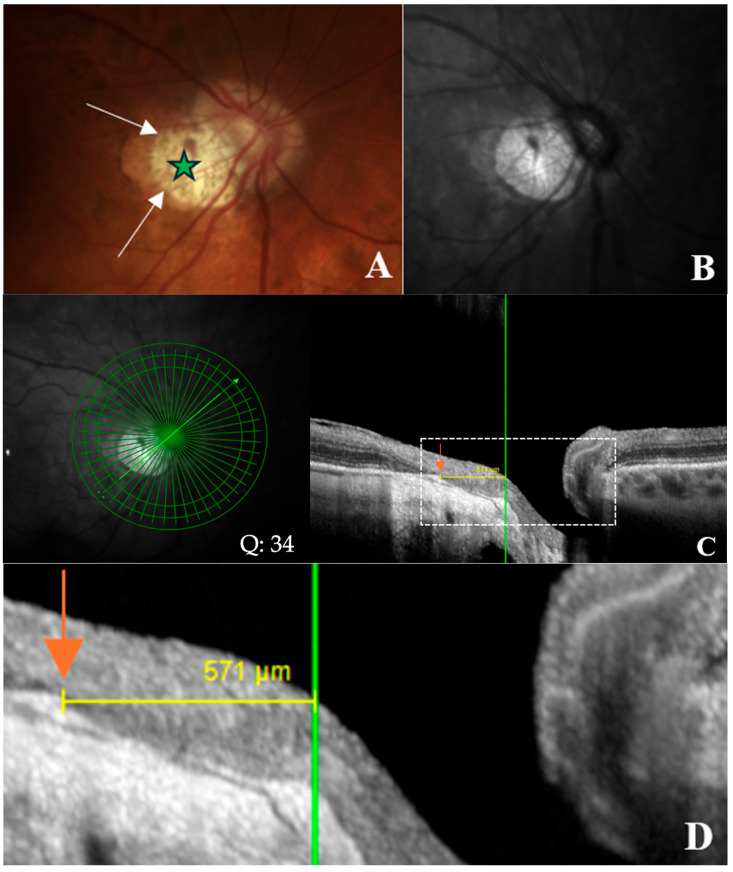 Figure 3
Figure 3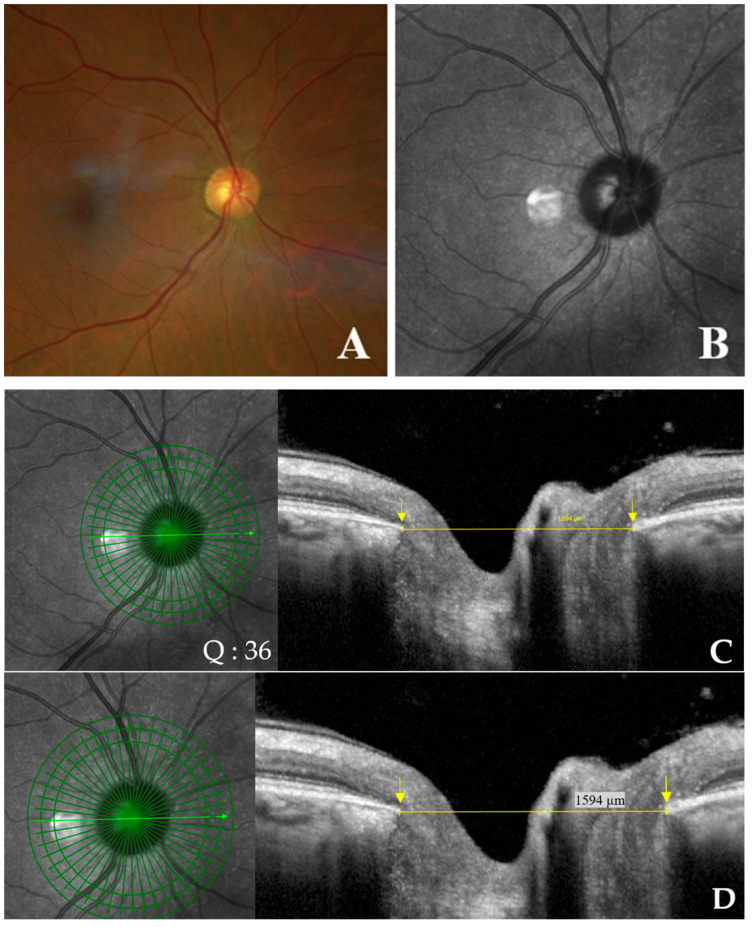 Figure 4
Figure 4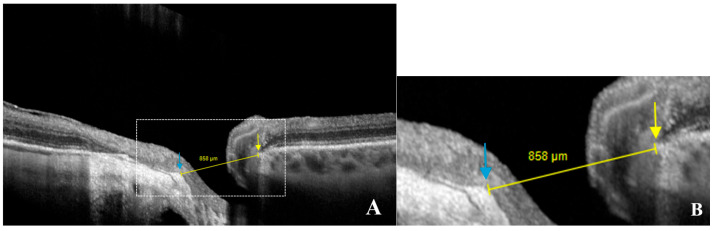 Figure 5
Figure 5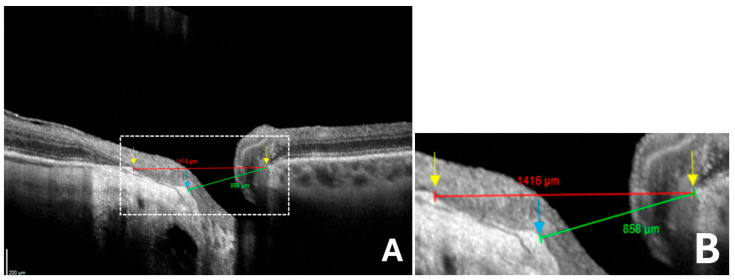 Figure 6
Figure 6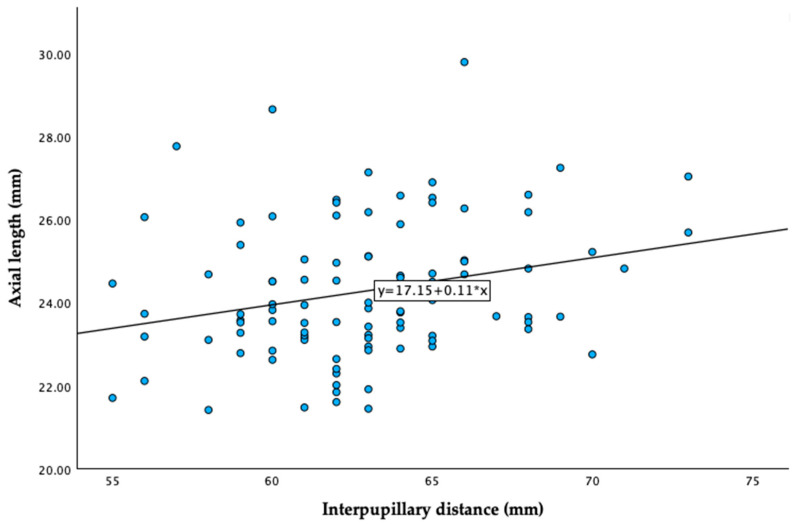 Figure 7
Figure 7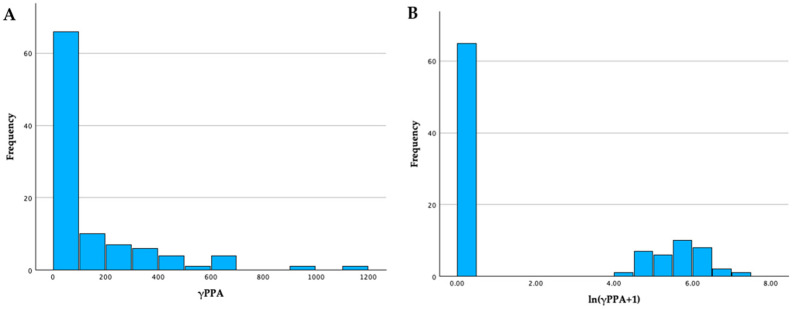 Figure 8
Figure 8Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlaucoma and retinal disorders · Ophthalmology and Visual Impairment Studies · Corneal surgery and disorders
1. Introduction
Myopia is an emerging global health issue, with projections estimating that by 2050, 50% of the world’s population will be myopic and 10% will develop high myopia [1]. This growing prevalence, accentuated by behavioral changes particularly during the COVID-19 pandemic, is expected to increase visual impairment and impose significant socioeconomic burdens [2,3].
In myopia, the elongation of the eyeball induces structural eye changes, including in the peripapillary region [4]. This includes the ovalization of the optic disc [5], along with the presence and increased prominence of gamma peripapillary atrophy (γPPA), which is characterized by an atrophic region adjacent to the optic disc, most commonly located temporally in myopic eyes, and is thought to result from a mismatch between the termination of Bruch’s membrane and the optic disc opening [4,6].
As illustrated in Figure 1, γPPA represents the zone between the end of Bruch’s membrane and the optic disc border [7].
Histological and Optical Coherence Tomography (OCT) imaging studies confirm the absence of Bruch’s membrane in γPPA [8,9], which extends from the edge of Bruch’s membrane opening (BMO) to the anterior scleral opening (ASO).
Two other types of peripapillary atrophy (PPA) have been distinguished through histological analyses. Unlike γPPA, both retain an intact Bruch’s membrane. Alpha PPA (αPPA) is characterized by irregularities in the retinal pigment epithelium (RPE) cells, and beta PPA (ßPPA), shows a complete loss of the RPE. These changes are also well visualized with OCT [10]. Figure 2 illustrates the three main types of PPA. In highly elongated eyes, delta PPA represents a subtype of γPPA presenting the thinning of the peripapillary scleral flange [10].
The degree of optic disc deformation is approached by the ovality index (OI), calculated as the ratio of the shortest to the longest disc diameters [11]. Both the OI and γPPA are proposed to quantify myopic structural peripapillary changes.
A recent biomechanical hypothesis suggests that the traction force exerted by the optic nerve sheaths (ONSs) may contribute to axial elongation in myopia [12]. This hypothesis draws on prior research demonstrating that the ONSs’ traction force aligns with the magnitude of forces generated by the extraocular muscles and acts in the axial direction. Such traction is proposed to induce significant peripapillary forces, particularly during adduction movements exceeding 26 degrees [13].
Such forces have been implicated in a spectrum of clinically relevant peripapillary myopic complications, in particular visual impairment or associated visual field defects mimicking those of glaucomatous optic neuropathy [14,15,16,17]. However, the factors that determine these peripapillary complications remain to be clarified.
Importantly, recent studies have highlighted that near-reading activities and increased digital screen time are particularly associated with greater myopia progression [18]. During such near-reading activity, the eyes not only adduct but also converge.
Interestingly, interpupillary distance (IPD) has been shown to influence vergence amplitudes [19]. Although near activities involve both adduction and convergence, to our knowledge, no study has examined whether IPD might be linked with structural peripapillary changes related to myopia through its role in vergence mechanisms.
Therefore, we aimed to investigate a potential correlation between IPD and two quantitative markers of structural peripapillary changes in myopic eyes: the OI and γPPA.
2. Materials and Methods
This was an observational, cross-sectional, monocentric study approved by the Ethics Committee of Erasmus Hospital (Brussels, Belgium) (reference P2024/450) and the Institutional Review Board (reference SRB2024239). This study complied with the tenets of the Declaration of Helsinki, and written informed consent was acquired from all participants.
2.1. Inclusion Population
Participants were approached during their routine visits to our glaucoma outpatient clinic and were consecutively recruited over a two-month period (January–February 2025). A target of at least 50 myopic eyes was set, given that this is a pilot study and the correlation between IPD and both the OI and γPPA has never been studied before.
2.2. Inclusion Criteria
Participants aged 18 years or older with no history of strabismus, strabismus surgery, posterior segment surgery, or trabeculectomy were included. An OCT signal quality score of at least 25 was also required.
2.3. Exclusion Criteria
Participants were excluded if they were younger than 18 years, had a history of ocular trauma, glaucoma surgery, posterior segment surgery, or strabismus surgery. Eyes with optic nerve anomalies unrelated to myopia or glaucoma or with an OCT signal quality score below 25 were also excluded.
2.4. Myopic Group
The classification of myopia was primarily based on the spherical equivalent (SE ≤ −0.50 D), in accordance with the International Myopia Institute [20]. In cases where refractive error (RE) data were missing or deemed unreliable, axial length (AL) was used as a secondary criterion. Specifically, if AL was ≥26.0 mm, the eye was classified as myopic. If AL was <26.0 mm, the eye was classified as “undefined” with respect to RE. This approach enabled classification even in the absence of reliable refractive data, as in the following scenarios: (a) eyes with a history of refractive surgery, for which preoperative refraction was not available for analysis; (b) eyes with a history of cataract surgery without available preoperative remote refraction from cataract documentation; and (c) eyes with unoperated but clinically significant cataract at the time of inclusion, for which no reliable pre-cataract refraction could be retrieved.
This strategy was also chosen to ensure that eyes with moderate or low myopia were not misclassified as non-myopic due to shorter axial lengths. Relying solely on axial length could have led to the underrepresentation of these patients, especially since axial elongation does not always correlate linearly with refractive error [20]. Therefore, the spherical equivalent was prioritized when available, as it better captures the full range of myopia severity.
The use of a 26.0 mm threshold aligns with the established definition of high myopia as a subgroup of eyes with a high degree of myopic refractive error. High myopia is distinct from pathologic myopia, which is defined by complications of myopia that may also occur in eyes without high myopia [21].
2.5. General and Ocular Data
Age and gender were recorded for each subject. Data from the comprehensive ophthalmic examination were retrieved for both eyes of the subjects. For each eye, the following parameters were recorded: RE in SE, AL values using IOL Master^®^ (Carl Zeiss Meditec, Jena, Germany), and IPD measurements with auto-refraction (TONOREF II, model RKT-2014; NIDEK Co., Ltd., Tokyo, Japan). Color fundus pictures using a Clarus^®^ non-mydriatic cameras (PRO NM Carl Zeiss Meditec, Jena, Germany) and spectral-domain OCT imaging using a Spectralis^®^ S3300 model, version 6.16.2 (Heidelberg Engineering GmbH, Heidelberg, Germany), were analyzed.
2.6. Color Fundus Photographs
These images were used to exclude eyes with retinal or optic nerve anomalies unrelated to myopia or glaucoma, in order to eliminate potential confounding factors in the interpretation of structural findings.
2.7. Eye Selection
Although a full ophthalmic examination was available for both eyes of each participant, only the right eye was included in the study unless it met an exclusion criterion, in which case the left eye was used instead. This approach was adopted to account for inter-eye correlation.
2.8. OCT Imaging
Radial OCT section acquisition using the commercialized Glaucoma Premium Edition module of the Spectralis^®^ performed for routine glaucoma documentation was used, specifically the 48 radial line B-scans centered on the optic disc of each participant for the tomographic analyses of the peripapillary region.
2.9. OCT Analysis
OCT sections and infrared images were opened in display mode; then, γPPA width and the OI were measured.
Measurement of width of γPPA
The width of γPPA, which is the PPA without Bruch’s membrane [8,9], was assessed using radial OCT. This atrophic zone extends from the BMO to the ASO (Figure 3A–D). The measurement of the γPPA width was performed along the minor axis, from the BMO indicated by the orange arrow, to the ASO, indicated by the vertical green line (Figure 3C,D).
OI measurement
The degree of disc deformation was quantified using the OI, calculated as the ratio of the shortest (minor axis) to longest (major axis) disc diameters [11] (Figure 4A–D). In the absence of γPPA, the diameter was measured from the BMO to the BMO [22] (Figure 4C,D).
In the presence of γPPA resulting from the temporal shifting of the BMO relative to the ASO, the diameter was measured from the ASO (temporal) to the BMO (nasal) (Figure 5A,B).
A standard minor axis measurement between BMO (nasal) and BMO (temporal) would overestimate its length, leading to an artificially high OI (Figure 6).
2.10. Analysis Procedure
OCT images from all eyes were analyzed by the investigator (Butt Sameer, B.S.), who performed the measurements. These measurements were subsequently reviewed and verified by the principal investigator, an experienced ophthalmologist (Ehongo Adèle, E.A.), to ensure accuracy.
2.11. Statistical Analyses
Descriptive statistics were presented as means, standard deviations (SDs), and ranges for continuous variables and as proportions and percentages for categorical variables. The Mann–Whitney U test was used to compare continuous variables between two groups. Due to the small sample sizes resulting from subgroup divisions, non-parametric tests were preferred. Statistical analyses were performed using IBM SPSS Statistics version 30.0. Pearson correlation analyses and multivariable regression models were conducted. The three outcome variables, namely, γPPA, OI, and AL, were analyzed separately as dependent variables. IPD was used as the main independent variable in all models, which were adjusted for age, gender, and myopia. Finally, a binary variable indicating the presence or absence of γPPA was included as a control variable in regression models where γPPA width was the dependent variable. A p-value < 0.05 was considered statistically significant.
3. Results
3.1. Sample Characteristics
Overall, 100 eyes of 100 subjects, 60 of whom were females, were included. The sample comprised 96 right eyes and 4 left eyes. The mean age ± SD was 62.6 ± 13.7 years, within a range of (20–83). The demographic and ocular features of the sample population are summarized in Table 1. A total of 83 eyes had reliable RE data.
Of the 17 eyes with unreliable refractive error, 10 eyes had a history of phacoemulsification with unavailable remote pre-cataract refractive data. Similarly, refractive data were excluded from five eyes with unoperated but clinically significant cataract, for which no prior refraction was available. Finally, two eyes with a history of refractive surgery were identified, and their refractive data were excluded, as no preoperative refraction was available.
Among the 17 eyes without reliable RE and excluded for refractive data, 7 were classified as myopic based on AL ≥ 26.0 mm, and 10 could not be classified due to AL < 26.0 mm. Ultimately, 52 eyes were classified as myopic and 38 as non-myopic, and 10 remained unclassified (Table 2).
The mean age and IPD were not significantly different between myopic and non-myopic groups. In contrast, all other parameters showed statistically significant differences. Participants with unclassified myopic status were significantly older and had a significantly shorter AL compared with those in the myopic group (Table 2).
Among the 100 eyes included in the study, 35 presented with γPPA. There was no statistically significant difference in mean age and IPD between participants with and without γPPA. In contrast, all other measured parameters demonstrated statistically significant differences between the two groups (Table 3).
3.2. Correlation Analyses
Pearson correlation analyses revealed no significant correlation between IPD and the OI (r = 0.001, p = 0.989), nor between IPD and γPPA width (r = −0.028, p = 0.782).
A significant but weak positive correlation was found between IPD and AL (r = 0.256, p = 0.011) (Table 4, Figure 7). Additionally, a significant correlation was observed between γPPA width and the OI, and both parameters showed significant correlations with AL (Table 4).
3.3. Multivariable Regression Analyses
Multivariable linear regression models were performed, including age, gender, myopia, and the presence or the absence of γPPA as control variables.
No significant association was found between IPD and γPPA width after adjustment (β = −3.814; 95% CI: −13.67 to 6.04; p = 0.44). Similarly, no significant association was observed between IPD and the OI (β = −0.001; 95% CI: −0.006 to 0.005; p = 0.85). A marginal trend toward significance was noted between IPD and AL (β = 0.078; 95% CI: −0.003 to 0.160; p = 0.059).
3.4. Sensitivity Analyses
Complementary analyses were conducted, including a logarithmic transformation of γPPA and Spearman correlation testing, both of which yielded similar results. These additional analyses are presented in Appendix A.
4. Discussion
Structural changes in the ONH and peripapillary region in myopic eyes have become a major focus of current research [23], given their clinical relevance, particularly their potential to mimic or overlap with glaucomatous visual field defects, including those seen in normal-tension glaucoma [14,17]. To our knowledge, this is the first study to investigate the relationship between IPD and myopic peripapillary changes, namely, the OI and γPPA width. Our findings showed no significant correlation between them, suggesting that IPD-related adduction forces may not play a major role in shaping ONH morphology in myopic eyes.
In contrast, we observed significant correlations between AL and both the OI and γPPA width. These findings support the established role of axial elongation as a major driver of myopic structural changes [4,24,25]. Moreover, the strong correlation between the OI and γPPA suggests that the change in optic disc shape and peripapillary changes are closely related, likely due to a shared underlying mechanism. Previous studies have shown that these deformations develop simultaneously during ocular elongation [4,24]. It is important to emphasize that myopic complications result from several structural deformations that develop simultaneously as the eye elongates. Changes such as optic disc obliquity and γPPA often occur together and may interact with other anatomical alterations. This cumulative remodeling process likely underlies more complex forms of myopic damage, including peripapillary intrachoroidal cavitation [17,26].
Structurally, myopic eyes have a longer AL. This increased AL compromises the sclera’s structure, reduces its rigidity and changes its biomechanical properties, making it more susceptible to deformation [27]. In eyes with marked AL, the traction on the optic disc may result from a short ONS or reduced sheath elasticity, both of which could restrict full ocular adduction [28].
Despite the weak correlation observed between IPD and AL (r = 0.256, p = 0.011), potentially reflecting shared developmental pathways influencing craniofacial and ocular growth [29], this relationship did not translate into the OI and γPPA after adjusting for confounding factors. After adjusting for AL, age, and gender, the correlation between IPD and the OI (β = −0.001, p = 0.85), as well as that between IPD and γPPA (β = −3.814, p = 0.44), remained statistically non-significant. These results suggest that axial elongation exerts a predominant influence, potentially overshadowing any biomechanical effects associated with IPD.
Although the subjects in this study were recruited from a glaucoma clinic, the optic disc changes underpinning the diagnosis of glaucomatous optic neuropathy (GON) are well established and follow a characteristic pattern, primarily involving loss of the neuroretinal rim, the hallmark of GON [10]. It is important to note that our study did not aim to assess the neuroretinal rim. Instead, we focused on γPPA (the PPA lacking Bruch’s membrane) and on the OI. To estimate the OI, Bruch’s membrane opening as the optic nerve border was considered. Unlike αPPA, which is present in almost all eyes [30], and ßPPA, which tends to enlarge with glaucoma progression, both of which were beyond the scope of this study, γPPA is associated with axial elongation in myopia. Therefore, GON-related changes do not represent a confounding factor in our analysis of γPPA. Moreover, the distinct histological characteristics of each PPA subtype can be clinically distinguished by OCT imaging [10], reducing the risk of misinterpretation.
Sclerosis of the lens may be a potential confounding factor affecting the refractive error data in this study. However, it is noteworthy that the mean age of the myopic group was slightly lower than that of the non-myopic group (although this difference did not reach statistical significance), suggesting that lens sclerosis is unlikely to be the determining factor in the negative refractive values observed in the myopic group.
The advanced mean age of our cohort (62.6 ± 13.7 years) was considered a potential confounding factor in the analysis of γPPA, given the positive correlation between age and cumulative myopic exposure, due to the progressive nature of axial elongation over time [31]. Accordingly, γPPA analyses were adjusted for age using linear regression. Interestingly, age did not differ significantly between myopic and non-myopic groups. Similarly, no significant age difference was observed between eyes with and without γPPA.
Overall, adjustments were made for the parameters age, gender, and myopia to account for potential confounding factors. Age was included because peripapillary changes naturally worsen with aging, independent of myopia [32]. Gender was controlled for, as women generally exhibit a smaller IPD compared with men, and this anatomical difference could indirectly influence outcomes [33]. Myopia was adjusted for, as its severity (assessed via axial elongation) is a major driver of ONH deformations [34].
Regarding the sample size, it is important to note that this study aimed to include eyes exhibiting both γPPA and an oval disc configuration. Since these changes are commonly associated with myopia, we initially planned to recruit 50 myopic eyes and a similar number of non-myopic eyes as controls. Ultimately, we included 52 myopic eyes and 35 eyes presenting γPPA. As a pilot study, these findings provide useful data for refining sample size calculations in future research, helping to address the sample size limitations of the present work.
Retinal image magnification varies with ocular biometry, so lateral (retina-parallel) measurements obtained on OCT are inherently affected [35,36]. The Spectralis^®^ OCT platform mitigates this automatically: its HEYEX software (v6.16.2), built on the Gullstrand schematic eye, applies an individualized lateral scaling factor based on each eye’s biometry [37,38]. Even so, some investigators propose adding an extra correction for AL, while others contend that entering a patient’s mean keratometry during scan acquisition offers a more accurate adjustment than the default setting [38]. Conversely, very recent work by Kirik et al. indicates that with Spectralis^®^ OCT, further AL compensation is unnecessary [39]. Therefore, we did not perform any corrections.
Myopia is of concern to most ophthalmic subspecialties due to its increasing prevalence, early onset, and diverse complications. We briefly reviewed its classification according to RE and AL in the Materials and Methods Section [20]. AL allows for a practical division of the myopic population into two subgroups: high myopes and non-high myopes. However, although pathological myopia (defined as myopia with ocular complications) is frequently associated with high myopia, such complications, including posterior staphyloma, may also occur in eyes with a normal AL [21]. These observations suggest that axial length alone may not be sufficient to identify myopes at risk of complications. In the future, it would be interesting to compare groups with and without high myopia, within the broader myopic population, in terms of IPD. A significant difference in IPD between these groups could help identify subgroups of myopic individuals at higher risk of developing high and/or pathological myopia.
Despite advances in our understanding of myopia-related complications [10,40], many questions remain unanswered, which justifies the need for continued research. Near work has been consistently associated with both the onset and progression of myopia. Demonstrating a potential link between IPD and structural markers such as the OI or γPPA could open avenues for new preventive strategies. One such approach might involve the use of prisms in reading glasses to reduce the convergence demand, thereby limiting myopia progression. Further studies addressing the limitations of the present work are warranted.
Limitations
First, this was a cross-sectional pilot study. This design limitation warrants future confirmatory and longitudinal investigations.
Second, differences in nasal bridge anatomy may influence the extent of the visual field. Specifically, flatter nasal bridges have been shown to allow for greater visibility in the nasal field during extreme gaze, due to reduced occlusion [41]. This anatomical variation may partly explain population-level differences in ONH changes associated with myopia. In our study, the nasal bridge structure was not assessed. Yet, for comparable IPD, differences in nasal anatomy, such as flatter bridges, may permit greater adduction, potentially contributing to the observed disparities in myopic ONH changes across populations. Including direct measurements of nasal morphology or stratifying analyses by ethnicity would have strengthened the interpretation of our findings.
Third, it is plausible that individuals with larger IPD require greater ocular movement amplitudes to maintain binocular vision, which could theoretically impact the binocular visual field. However, this adaptation largely depends on individual’s vergence capacity. Dag et al. have suggested that individuals with larger IPD may exhibit reduced vergence amplitudes, potentially indicating a less stable binocular fusion [19]. While findings remain inconclusive, this raises the possibility that structural variations such as IPD might influence binocular visual performance. As we did not assess binocular visual fields in this study, we cannot determine whether differences in IPD, γPPA width, or the OI translate into functional differences in binocular vision. Future studies should include binocular visual field testing to explore these potential correlations.
Fourth, measurements were performed by a single investigator and reviewed by a senior ophthalmologist. Independent double grading should be implemented in future studies.
Fifth, the study cohort was ethnically homogeneous, composed almost exclusively of individuals of Caucasian descent, with negligible representation of other populations. This lack of diversity may limit the generalizability of our findings to other ethnic populations, where myopic ONH changes are not only more prevalent but also tend to be more severe [42]. This limitation was not accounted for in the study design and should be addressed in future studies through more inclusive sampling or stratified analyses.
Sixth, as this was a pilot study, we arbitrarily enrolled 100 eyes, 52 of which were myopic. A larger sample may have allowed for the detection of significant correlations. Therefore, future research may build upon these preliminary findings to better define sampling needs in myopic populations.
Seventh, participants were recruited from a tertiary care clinic, involving a relatively homogeneous group that may not be representative of the general population.
5. Conclusions
This study is the first to investigate the relationship between IPD and structural changes in the peripapillary zone in myopia, specifically focusing on the OI and γPPA. Although previous studies have suggested that IPD may influence vergence amplitude and that duction movements could promote optic nerve deformations, no significant correlation was found between IPD and either the OI or γPPA width after adjusting for confounding variables. These findings highlight the dominant role of axial elongation in driving myopic ONH and peripapillary reshaping, outweighing any potential biomechanical influence of IPD. Future studies should consider longitudinal designs, include more ethnically diverse populations, and assess the binocular visual field extent to further elucidate the complex interplay of ocular structure, craniofacial features, and visual biomechanics.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Holden B.A. Fricke T.R. Wilson D.A. Jong M. Naidoo K.S. Sankaridurg P. Wong T.Y. Naduvilath T.J. Resnikoff S. Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050 Ophthalmology 20161231036104210.1016/j.ophtha.2016.01.00626875007 · doi ↗ · pubmed ↗
- 2Sankaridurg P. Tahhan N. Kandel H. Naduvilath T. Zou H. Frick K.D. Marmamula S. Friedman D.S. Lamoureux E. Keeffe J. IMI Impact of Myopia Investig. Ophthalmol. Vis. Sci.202162210.1167/iovs.62.5.233909036 PMC 8083082 · doi ↗ · pubmed ↗
- 3Wang J. Li Y. Musch D.C. Wei N. Qi X. Ding G. Li X. Li J. Song L. Zhang Y. Progression of Myopia in School-Aged Children After COVID-19 Home Confinement JAMA Ophthalmol.202113929330010.1001/jamaophthalmol.2020.623933443542 PMC 7809617 · doi ↗ · pubmed ↗
- 4Kim T.W. Kim M. Weinreb R.N. Woo S.J. Park K.H. Hwang J.M. Optic disc change with incipient myopia of childhood Ophthalmology 20121192126.e 310.1016/j.ophtha.2011.07.05121978594 · doi ↗ · pubmed ↗
- 5Dai Y. Jonas J.B. Ling Z. Sun X. Ophthalmoscopic-Perspectively Distorted Optic Disc Diameters and Real Disc Diameters Investig. Ophthalmol. Vis. Sci.2015567076708310.1167/iovs.14-1603326536062 · doi ↗ · pubmed ↗
- 6Kim M. Kim T.W. Weinreb R.N. Lee E.J. Differentiation of parapapillary atrophy using spectral-domain optical coherence tomography Ophthalmology 20131201790179710.1016/j.ophtha.2013.02.01123672970 · doi ↗ · pubmed ↗
- 7Ehongo A. Optical Coherence Tomography Analysis of Peripapillary Intrachoroidal Cavitation Ph D. Thesis Université Libre de Bruxelles Brussels, Belgium 2024
- 8Dai Y. Jonas J.B. Huang H. Wang M. Sun X. Microstructure of parapapillary atrophy: Beta zone and gamma zone Investig. Ophthalmol. Vis. Sci.2013542013201810.1167/iovs.12-1125523462744 · doi ↗ · pubmed ↗