Development of a Risk Model to Identify and Prevent Factors Influencing Erectile Dysfunction After Robotic Radical Prostatectomy
Hakan Karaca, Resul Sobay, Metin Mod, Ahmet Tahra, Hasan Samet Güngör, Abdurrahman İnkaya, Eyüp Veli Küçük

TL;DR
This study develops a risk model to predict and prevent erectile dysfunction after prostate cancer surgery, using patient data and surgical factors.
Contribution
The novel contribution is a nomogram that predicts erectile dysfunction outcomes after robotic prostatectomy using specific clinical and anatomical variables.
Findings
Older age and higher comorbidity index correlate with increased risk of erectile dysfunction.
Bilateral nerve-sparing procedures are associated with better erectile function outcomes.
Surgical technique significantly influences postoperative erectile function.
Abstract
Background/Objectives: Prostate cancer ranks as the second-most prevalent cancer globally, and is the fifth-ranking cause of cancer-related mortality. Radical prostatectomy presents a significant risk of postoperative sequelae, including erectile dysfunction. Postoperative erectile dysfunction adversely affects the patient’s quality of life and can severely impact total treatment satisfaction. Nomograms have demonstrated efficacy in forecasting diverse outcomes in urology. We sought to create a nomogram to facilitate a more precise, evidence-based, and individualized prediction of erectile function outcomes following radical prostatectomy. Between January 2018 and January 2022, one hundred and eleven prostate cancer patients had robot-assisted radical prostatectomy, excluding those who had undergone prior transurethral prostatectomy, radiotherapy, or hormone therapy. Demographics,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
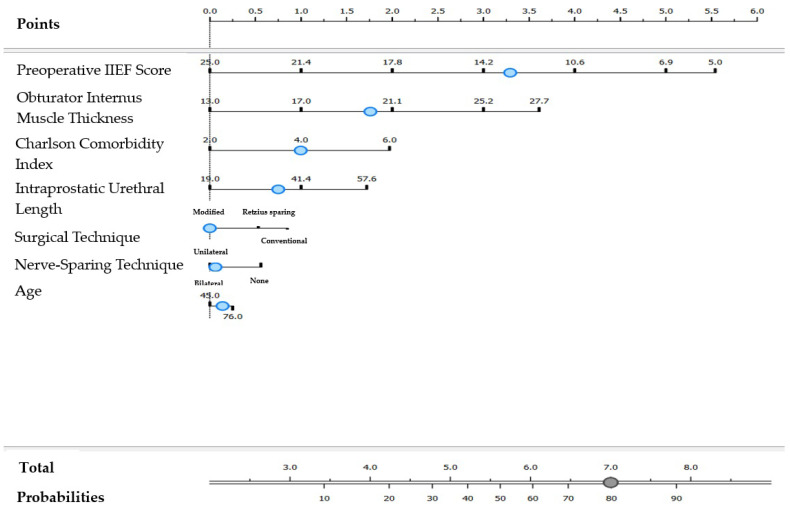 Figure 1
Figure 1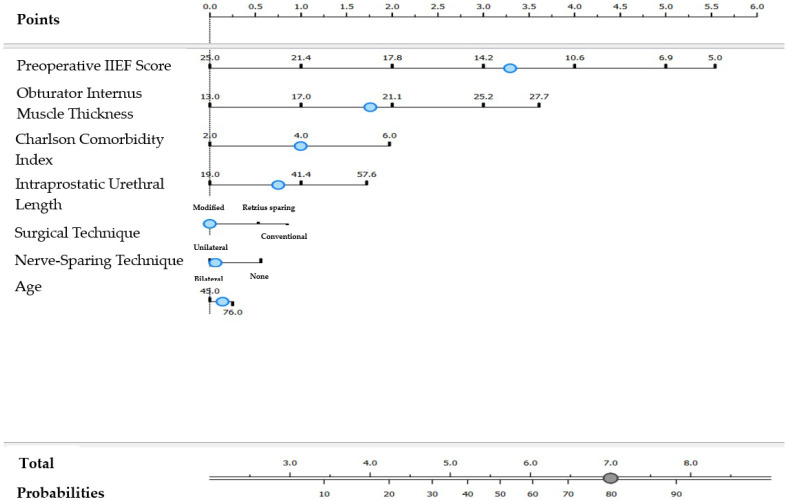 Figure 2
Figure 2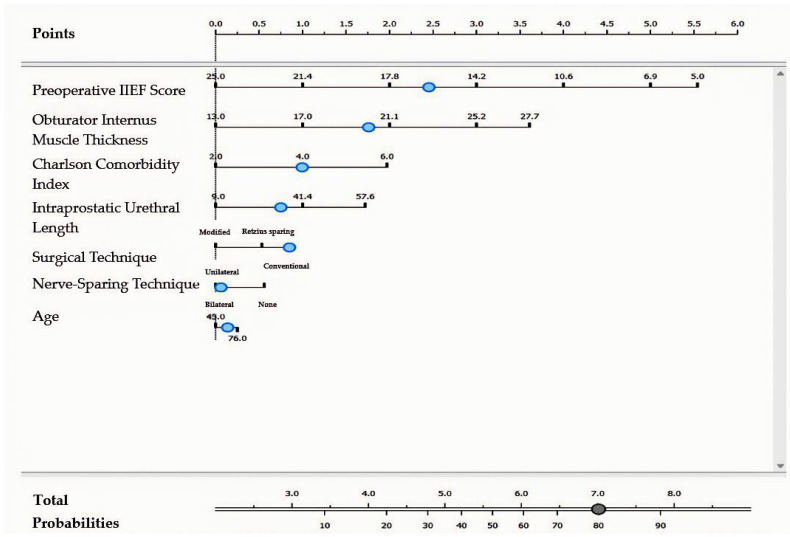 Figure 3
Figure 3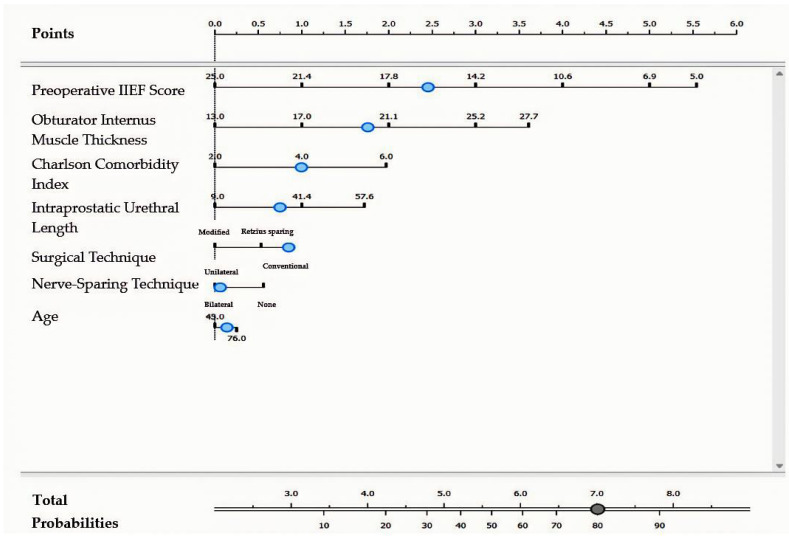 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSexual function and dysfunction studies · Prostate Cancer Diagnosis and Treatment · Genital Health and Disease
1. Introduction
Prostate cancer ranks as the second-most prevalent cancer in men globally, with approximately 1.4 million diagnoses reported in 2020. It is the fifth-ranking cause of cancer-related mortality, contributing to an estimated 375,000 deaths [1]. Incidence and mortality rates exhibit considerable variation across different geographic locations. Identifying risk factors for prostate cancer development is essential for primary and secondary prevention [2].
Radical prostatectomy (RP) is a widely utilized therapeutic approach for managing prostate cancer. This surgical approach results in positive outcomes in terms of disease-free and overall survival rates; however, it is linked to several potential complications, particularly postoperative erectile dysfunction (ED) and urinary incontinence. The declining average age at diagnosis has rendered the preservation and recovery of postoperative erectile function a critical issue in urology [3,4]. A diverse array of ED rates subsequent to RP has been documented. Tal et al. conducted a meta-analysis on ED rates post-RP, revealing significant variability in outcomes, with incidence rates between 14% and 90%. This extensive variability restricts the applicability of these findings in informing clinical decision-making and delivering effective postoperative counseling for patients with prostate cancer [5]. Mulhall similarly reported significant variability in the incidence of erectile dysfunction following radical prostatectomy, with rates between 12% and 96%. Higher ED rates were observed in multi-center, multi-surgeon studies, compared to those conducted at single centers by individual surgeons, indicating the impact of surgical technique and institutional factors on postoperative outcomes [6]. Resnick et al. reported findings from the Prostate Cancer Outcomes Study (PCOS), a population-based cohort study that prospectively tracked men diagnosed with prostate cancer over a 15-year period starting in 1991 [7]. In a study involving 1655 participants evaluated at baseline and at 2, 5, and 15 years after receiving either RP or radiation therapy, individuals who underwent prostatectomy exhibited a significantly higher incidence of ED at both the 2-year and 5-year marks post-treatment. During the follow-up periods, 78% to 87% of men reported experiencing erections inadequate for sexual intercourse [7]. Johansson found that among 173 men, 146 (84%) experienced ED following RP [8].
ED is assessed using the International Index of Erectile Function (IIEF) questionnaire. Patients with an IIEF score of 17 or higher are classified as having preserved erectile function, while those with a score below 17 are categorized as having complete erectile dysfunction.
The nomogram has demonstrated efficacy in predicting diverse outcomes within the field of urology [9,10]. Predictive models have demonstrated superiority over clinician estimations. The complication profile associated with a specific treatment strategy can impact the patient’s decision-making process, and the realistic expectations that develop can influence the patient’s satisfaction with the chosen treatment [11,12]. In this study, we sought to create a nomogram to facilitate more precise, evidence-based, and individualized predictions of erectile function (EF) outcomes following RP.
2. Materials and Methods
2.1. Compliance with Ethical Standards
Ethical approval for the study was obtained from the Ethics Committee of Health Science University Umraniye Research and Training Hospital, with approval number 0.01/275.
2.2. Study Design
The study comprised 111 patients who received robot-assisted radical prostatectomy (RARP) for prostate cancer carried out by a single surgeon between January 2018 and January 2022. All patients had no previous history of transurethral prostatectomy, radiotherapy, or hormone therapy. The demographic features, medical records, and preoperative and postoperative erectile function statuses of the patients were analyzed.
Multiparametric MRI assessments were conducted by two experienced urologists and subsequently evaluated in conjunction with a radiologist possessing substantial clinical expertise in urology.
Preoperative age, Charlson Comorbidity Index, preoperative IIEF score, preoperative smoking history, preoperative PSA levels, Gleason grade group in biopsy, prostate volume, presence of median lobe, bladder neck invasion, interval between biopsy and surgery, surgical technique employed, duration of surgery, extent of nerve preservation, perioperative blood loss, presence of lymph node dissection, thickness of obturator internus, length of membranous urethra, angle with prostate axis, intraprostatic urethra length, urethral width, postoperative pathological stage, positivity of postoperative surgical margins, duration of postoperative catheterization, early and late use and duration of PDE5 inhibitors postoperatively, and early and late application and duration of intracavernous vasoactive agents postoperatively were all assessed. A nomogram was developed utilizing criteria recognized as major indicators of the risk for postoperative erectile dysfunction.
During the postoperative phase, all patients were instructed to engage in penile rehabilitation using either daily oral tadalafil 5 mg or tadalafil 20 mg administered three times weekly after catheter removal. At the 6-month follow-up, patients who could not attain erections received intracavernosal injection of vasoactive drugs. The IIEF score was utilized to evaluate erection status at the 6-month follow-up.
All procedures in the study were conducted transperitoneally with the Da Vinci Xi robotic system. The nerve-sparing procedure was implemented in accordance with the previously described ultrapreservation anterior-sparing method [13].
2.3. Statistical Analysis
Statistical Package for the Social Sciences (SPSS) version 27 was utilized for statistical analysis. Descriptive statistical techniques (mean, standard deviation, median, frequency, percentage, minimum, maximum) were employed in the analysis of the study data. The normality of distribution for quantitative data was assessed utilizing the Shapiro–Wilk test and graphical analyses. For continuous variables with normal distribution, Student’s t-test was employed for comparisons between two groups. For continuous variables lacking normal distribution, the Mann–Whitney U test was utilized. For categorical variables, Pearson’s chi-square test was used when expected cell frequencies were adequate (≥5), while Fisher’s exact test or Fisher–Freeman–Halton test were employed when expected cell frequencies were inadequate (<5). One-way analysis of variance and Bonferroni-adjusted pairwise comparisons were employed for comparisons among multiple groups of normally distributed quantitative variables, whilst Student’s t-test was utilized for comparisons between two groups. For quantitative variables lacking a normal distribution, Kruskal–Wallis and Dunn–Bonferroni tests were employed for comparisons across many groups, whilst the Mann–Whitney U test was utilized for comparisons between two groups. The Wilcoxon signed-ranks test was utilized for within-group comparisons of quantitative variables lacking a normal distribution. Logistic regression analysis and nomograms were employed in multivariate evaluations. Statistical significance was defined as p < 0.05.
3. Results
In the initial year of the trial, out of 111 participating patients, 73 exhibited complete ED, whilst 38 maintained EF. All demographic and preoperative variables potentially influencing postoperative EF were assessed, revealing associations with age, Charlson Comorbidity Index, and IIEF score (Table 1).
The multiparametric MRI data of the patients were evaluated, revealing a link that suggests obturator internus muscle thickness and intraprostatic urethral length influence post-prostatectomy erectile function (Table 2).
In patients with intact erectile function, the adoption rate of the modified surgical technique—ultrapreservation anterior-sparing RARP—was markedly elevated (p = 0.002; p < 0.01). Implementation of the bilateral nerve-sparing approach resulted in a statistically significant enhancement in this group. (p = 0.003; p < 0.01) (Table 3).
A logistic regression analysis was performed to ascertain the risk factors affecting erectile dysfunction and to create a nomogram.
The impacts of age, preoperative IIEF score, obturator internus thickness, intraprostatic urethral length, Charlson Comorbidity Index, nerve-sparing technique, and surgical technique on erectile dysfunction were evaluated using logistic regression analysis.
The model exhibited statistical significance.
(Chi-Square = 56.038; p = 0.001; p < 0.01), with an explanatory power (Nagelkerke R^2^) of 82%. Model 1Surgical TechniqueModified (Ultrapreservation Anterior-Sparing)Nerve-Sparing TechniqueBilateral ScorePreoperative IIEF ScoreCut Off: <13.1ODDS: 3.34.79Obturator Internus Muscle ThicknessCut Off: ≥20.2ODDS: 1.72.47Charlson Comorbidity Index Cut Off: ≥4ODDS: 11.45Intraprostatic Urethral LengthCut Off: ≥35.8ODDS: 0.751.09AgeCut Off: ≥62ODDS: 0.140.20
Score****10
For patients undergoing a modified surgical technique combined with a bilateral nerve-sparing technique, the formula for predicting complete erectile dysfunction was as follows (Figure 1): Model 2Surgical TechniqueModified
Nerve-Sparing TechniqueUnilateral ScorePreoperative IIEF ScoreCut Off: <13.1ODDS: 3.34.86Obturator Internus Muscle ThicknessCut Off: ≥20.2ODDS: 1.72.43Charlson Comorbidity Index Cut Off: ≥4ODDS: 11.43Intraprostatic Urethral LengthCut Off: ≥35.8ODDS: 0.751.07AgeCut Off: ≥62ODDS: 0.140.21
Score****10
For individuals undergoing a modified surgical technique with unilateral nerve-sparing approach, the nomogram for complete erectile dysfunction was as follows: [Preoperative IIEF (<12.9)] × 4.86 + [Obturator Internus Thickness (≥20.2 mm)] × 2.43 + [Charlson Comorbidity Index (≥4)] × 1.43 + [Intraprostatic Urethral Length (≥35.8 mm)] × 1.07 + [Age (≥62 years)] × 0.20 (Figure 2). Model 3Surgical TechniqueConventional
Nerve-Sparing TechniqueBilateral ScorePreoperative IIEF ScoreCut Off: <15.9ODDS: 2.54.11Obturator Internus Muscle ThicknessCut Off: ≥20.2ODDS: 1.762.79Charlson Comorbidity Index Cut Off: ≥4ODDS: 11.64Intraprostatic Urethral LengthCut Off: ≥35.8ODDS: 0.751.23AgeCut Off: ≥62ODDS: 0.140.23
Score****10
For patients who underwent a conventional surgical technique and bilateral nerve-sparing technique, the formula for complete erectile dysfunction was as follows: [Preoperative IIEF (<16.1)] × 4.11 + [Obturator Internus Thickness (≥20.2)] × 2.79 + [Charlson Index (≥4)] × 1.64 + [Intraprostatic Urethra Length (≥35.8)] × 1.23 + [Age (≥62)] × 0.23 (Figure 3). Model 4
Surgical TechniqueConventional
Nerve-Sparing TechniqueUnilateral ScorePreoperative IIEF ScoreCut Off: <15.9ODDS: 2.54.11Obturator Internus Muscle ThicknessCut Off: ≥20.2ODDS: 1.762.79Charlson Comorbidity Index Cut Off: ≥4ODDS: 11.64Intraprostatic Urethral LengthCut Off: ≥35.8ODDS: 0.751.23AgeCut Off: ≥62ODDS: 0.140.23
Score****10
For patients who underwent a conventional surgical technique with unilateral nerve-sparing, complete erectile dysfunction was predicted by the following model: [Preoperative IIEF (<16.1)] × 4.11 + [Obturator Internus Thickness (≥20.2 mm)] × 2.79 + [Charlson Comorbidity Index (≥4)] × 1.64 + [Intraprostatic Urethral Length (≥35.8 mm)] × 1.23 + [Age (≥62 years)] × 0.23 (Figure 4).
4. Discussion
Prostate cancer ranks among the most prevalent cancers in the male population. The prevalence of screening methods has led to earlier-stage diagnoses of prostate cancer. The increasing incidence of prostate cancer in younger men has heightened concerns regarding post-cancer EF.
RP is the most commonly executed therapeutic approach for localized or locally progressed prostate carcinoma. RARP has emerged as a prevalent method in the surgical management of prostate cancer.
Due to the heterogeneity in EF outcomes documented in the literature, clinicians conducting preoperative consultations encounter a conundrum. The multitude of factors affecting post-prostatectomy EF, along with the intricate interrelations among these parameters, leads to variability in predicting erectile outcomes. Consequently, a nomogram that offers an evidence-based, individualized prediction would be exceedingly advantageous.
Brajtbord et al. documented erectile recovery following RP in two age categories: ≤60 years and >60 years. Older males exhibited an increased probability of clinically significant deterioration in EF [14]. Alemozaffar et al. reported in a study on a prediction model for postoperative ED that advancing age correlated with a diminished likelihood of maintaining EF, even after controlling for baseline performance [15]. In our study, consistent with prior research, we noted a rise in ED with increasing age. The results indicate that advancing age is a notable risk factor for ED.
Salter et al. demonstrated that a history of smoking may be linked to ED three months post-RP [16]. Our investigation, however, revealed no statistically significant difference in smoking rates among the cases based on IIEF scores. Variations in the timing of postoperative EF assessment, as well as in the duration and level of cigarette consumption, may account for discrepancies between studies. Given the rising popularity of electronic cigarette usage, future studies may investigate the effects of these products on erectile function post-RP.
The application of a modified surgical technique (ultrapreservation anterior-sparing RARP) was markedly more prevalent among patients who maintained EF (p = 0.002; p < 0.01), while the conventional technique was notably more common among individuals with complete ED (p = 0.007; p < 0.01).
Bhat et al. indicated that a greater extent of nerve sparing correlated with enhanced EF outcomes [17]. Zhao et al. indicated that postoperative potency levels, both early and late, were superior in patients who received intrafascial RP compared to those who received non-intrafascial RP [18]. In accordance with the existing literature, our investigation revealed that use of the bilateral nerve-sparing technique was much greater in instances of retained EF.
Our investigation revealed no statistically significant variations in Gleason grade groups based on IIEF levels. A study by Pikramenos et al. reported a potential correlation between high Gleason scores and preoperative IIEF levels; however, no statistically significant relationship with postoperative IIEF values was observed [19]. This result may be ascribed to the sample size. Research involving bigger cohorts may uncover statistically significant disparities.
The primary limitations of this study are its retrospective design and small sample size. Although RARP was performed by a single highly experienced surgeon (with over 1000 RARPs) in our study, we believe that implementation of RARP by various surgeons is warranted. Additionally, the single-center nature of our study may be regarded as a limitation.
A principal strength of our study is its comprehensive evaluation of all patient-related factors, surgical procedures, and parameters that may affect EF post-RP, with patients being meticulously tracked during the postoperative period. Before now, no studies in the literature have investigated the correlation between post-prostatectomy ED and factors such as membranous urethral length, the angle between the membranous urethra and the prostate axis, obturator internus thickness, levator ani thickness, urethral width, and intraprostatic urethral length. Our study is the first to establish that patients with complete ED exhibit a statistically significant increase in obturator internus thickness compared to those with preserved erectile function (p = 0.040; p < 0.05), as well as a significantly greater intraprostatic urethral length (p = 0.039; p < 0.05).
We created four nomograms with variable cut-off values based on the extent of nerve sparing and the surgical procedure used. These nomograms provide a tailored methodology for forecasting ED based on individualized patient treatment. In comparison to the initial nomogram established by Mulhall et al. [20], we noted that age, extent of nerve sparing, preoperative IIEF score, and comorbidity score are shared factors. Nonetheless, our analysis incorporates supplementary mpMRI parameters. Given its practical application, this model has the potential to aid clinicians in daily practice by facilitating individualized risk assessment of postoperative ED. This may thereafter empower both clinicians and patients to undertake suitable preventive or rehabilitative actions promptly.
5. Conclusions
Our study revealed that advanced age is a substantial risk factor for postoperative erectile dysfunction in patients receiving robot-assisted radical prostatectomy, and that bilateral nerve-sparing surgery is an advantageous method for preserving erectile function. The parameters we assessed, including surgical method, age, preoperative IIEF score, comorbidity index, obturator internus muscle thickness, and intraprostatic urethral breadth, demonstrated a statistically significant influence on erectile function. The nomogram we created offers individualized prognostic data to evaluate postoperative erectile function prior to surgery, based on these characteristics. Further large-scale, multi-center investigations are essential to enhance the accuracy and generalizability of these results and nomograms.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sung H. Ferlay J. Siegel R.L. Laversanne M. Soerjomataram I. Jemal A. Bray F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries CA Cancer J. Clin.20217120924910.3322/caac.2166033538338 · doi ↗ · pubmed ↗
- 2Bergengren O. Pekala K.R. Matsoukas K. Fainberg J. Mungovan S.F. Bratt O. Bray F. Brawley O. Luckenbaugh A.N. Mucci L. 2022 Update on Prostate Cancer Epidemiology and Risk Factors—A Systematic Review Eur. Urol.20238419120610.1016/j.eururo.2023.04.02137202314 PMC 10851915 · doi ↗ · pubmed ↗
- 3Stolzenburg J.U. Graefen M. Kriegel C. Michl U. Martin Morales A. Pommerville P.J. Manning M. Büttner H. Henneges C. Schostak M. Effect of surgical approach on erectile function recovery following bilateral nerve-sparing radical prostatectomy: An evaluation utilising data from a randomised, double-blind, double-dummy multicentre trial of tadalafil vs. placebo BJU Int.201511624125110.1111/bju.1303025560809 · doi ↗ · pubmed ↗
- 4Bratu O.G. Diaconu C.C. Mischianu D.L. Constantin T. Stanescu A.M. Bungau S.G. Ionita-Radu F. Marcu R.D. Therapeutic options in patients with biochemical recurrence after radical prostatectomy (Review)Exp. Ther. Med.2019185021502510.3892/etm.2019.791631798723 PMC 6880385 · doi ↗ · pubmed ↗
- 5Tal R. Alphs H.H. Krebs P. Nelson C.J. Mulhall J.P. Erectile function recovery rate after radical prostatectomy: A meta-analysis J. Sex. Med.200962538254610.1111/j.1743-6109.2009.01351.x 19515209 PMC 4097184 · doi ↗ · pubmed ↗
- 6Mulhall J.P. Defining and reporting erectile function outcomes after radical prostatectomy: Challenges and misconceptions J. Urol.200918146247110.1016/j.juro.2008.10.04719084865 · doi ↗ · pubmed ↗
- 7Resnick M.J. Koyama T. Fan K.H. Albertsen P.C. Goodman M. Hamilton A.S. Hoffman R.M. Potosky A.L. Stanford J.L. Stroup A.M. Long-term functional outcomes after treatment for localized prostate cancer N. Engl. J. Med.201336843644510.1056/NEJ Moa 120997823363497 PMC 3742365 · doi ↗ · pubmed ↗
- 8Johansson E. Steineck G. Holmberg L. Johansson J.E. Nyberg T. Ruutu M. Bill-Axelson A. SPCG-4 Investigators Long-term quality-of-life outcomes after radical prostatectomy or watchful waiting: The Scandinavian Prostate Cancer Group-4 randomised trial Lancet Oncol.20111289189910.1016/S 1470-2045(11)70162-021821474 · doi ↗ · pubmed ↗