Natural Language Processing for Identification of Hospitalized People Who Use Drugs: Cohort Study
Taisuke Sato, Emily D Grussing, Ruchi Patel, Jessica Ridgway, Joji Suzuki, Benjamin Sweigart, Robert Miller, Alysse G Wurcel

TL;DR
This study shows that natural language processing improves the identification of hospitalized people who use drugs, especially those from underrepresented groups.
Contribution
The study introduces NLP as a more accurate method for identifying PWUD in electronic medical records compared to traditional billing codes.
Findings
NLP had a 54% positive predictive value, outperforming ICD codes and other traditional methods.
NLP significantly enhanced identification when integrated with other methods.
Racially and ethnically minoritized individuals had lower rates of PWUD-related documentation.
Abstract
People who use drugs (PWUD) are at heightened risk of severe injection–related infections. Current research relies on billing codes to identify PWUD—a methodology with suboptimal accuracy that may underestimate the economic, racial, and ethnic diversity of hospitalized PWUD. The goal of this study is to examine the impact of natural language processing (NLP) on enhancing identification of PWUD in electronic medical records, with a specific focus on determining improved systems of identifying populations who may previously been missed, including people who have low income or those from racially and ethnically minoritized populations. Health informatics specialists assisted in querying a cohort of likely PWUD hospital admissions at Tufts Medical Center between 2020‐2022 using the following criteria: (1) ICD-10 codes indicative of drug use, (2) positive drug toxicology results, (3)…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
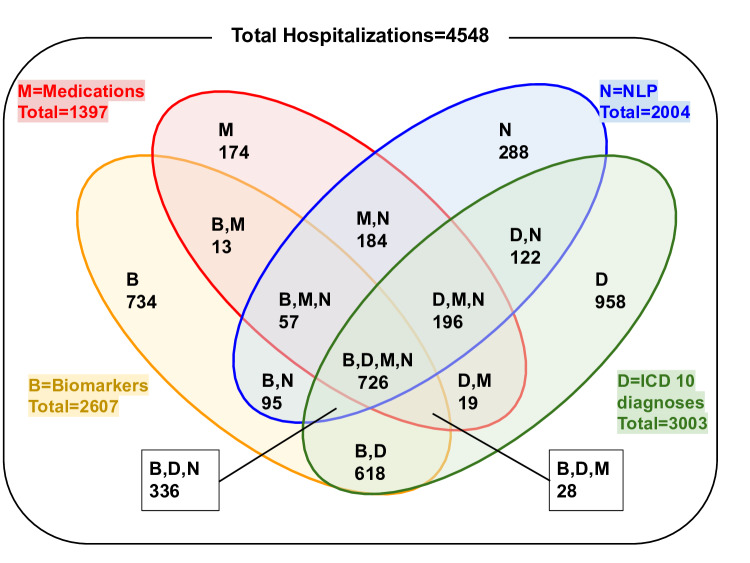 Figure 1
Figure 1| Parent code | Description |
|---|---|
|
| Opioid-related disorders |
|
| Cocaine-related disorder |
|
| Other stimulant–related disorders |
|
| Poisoning by opium, heroin, other opioids, methadone, synthetic narcotics, cocaine, unspecified narcotics and psychostimulants. |
|
| Hepatitis C |
|
| Chronic viral hepatitis C |
| Variables | Criteria for entering cohort | Unadjusted OR | Adjusted OR | ||
|---|---|---|---|---|---|
| Encounters (N=4548) | Encounters-BDMN (n=726) | Encounters-NLP | |||
| Age (years), mean (SD) | 47.9 (13.8) | 43.3 (10.7) | 45.6 (14.5) | – | – |
| Sex, n (%) | |||||
| Male | 2837 (62.4) | 457 (62.9) | 155 (53.8) | – | – |
| Female | 1711 (37.6) | 269 (37.1) | 133 (46.2) | – | – |
| Race/Ethnicity, n (%) |
|
|
|
|
|
| Racially/Ethnically minoritized | 1583 (34.8) | 176 (24.2) | 114 (60.4) | 1.00 (Ref) | 1.00 (Ref) |
| Black | 773 (17) | – | – | – | – |
| Hispanic | 469 (10.3) | – | – | – | – |
| Asian | 122 (2.7) | – | – | – | – |
| Asian Indian | 24 (0.5) | – | – | – | |
| Hawaiian | 1 (0.02) | – | – | – | – |
| Other | 22 (0.5) | – | – | – | – |
| Unknown | 172 (3.8) | – | – | – | – |
| White/non-Hispanic | 2965 (65.2) | 550 (75.8) | 174 (39.6) | 2.04 (1.53, 2.73) | 2.07 (1.54, 2.79) |
| Length of hospitalization, mean (SD) | 38.7 (26.3) | 41.5 (25.7) | 34.7 (26.4) | – | – |
| Social variability index (quartiles) |
|
|
|
|
|
| 3rd-4th | 2462 (54.1) | 461 (63.5) | 163 (56.6) | 1.34 (1.01, 1.77) | 1.41 (1.06, 1.88) |
| 1st-2nd | 2070 (45.51) | 262 (36.1) | 124 (43.1) | 1.00 (Ref) | 1.00 (Ref) |
| Missing | 16 (0.4) | 3 (0.4) | 1 (0.4) | – | – |
| Urine toxicology, n (%) | |||||
| Opiate | 658 (14.5) | 136 (18.7) | 0 | – | – |
| Fentanyl | 1313 (24.9) | 430 (59.2) | 0 | – | – |
| Oxycodone | 369 (8.1) | 66 (9.1) | 0 | – | – |
| Methadone | 272 (5.9) | 224 (30.9) | 0 | – | – |
| Cocaine | 622 (13.7) | 258 (35.5) | 0 | – | – |
| Amphetamine | 323 (7.1) | 153 (21.1) | 0 | – | – |
| Primary language, n (%) |
| ||||
| English | 4296 (94.5) | 703 (96.8) | 270 (93.8) | – | – |
| Spanish | 123 (2.7) | 23 (3.2) | 11 (3.8) | – | – |
| Cohort | Hospitalizations in the cohort, n | Charts reviewed, n | Charts confirmed as true PWUD | Positive predictive value (%) |
|---|---|---|---|---|
| D (diagnostic codes present) | 958 | 93 | 40 | 43 |
| N (NLP present) | 288 | 99 | 53 | 54 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPharmacovigilance and Adverse Drug Reactions
Introduction
In the absence of harm reduction tools, people who use drugs (PWUD) are at increased risk of disease, hospitalization, and death [1-3]. Gaps in the provision of guideline-concordant care to hospitalized PWUD occur, especially among individuals from racially and ethnically minoritized communities [4-6]. Barriers to optimization of health care for hospitalized PWUD include undertreatment of pain and substance use disorders, which have been linked to discharges before medical optimization and higher rates of readmission and mortality [7-9]. Best practices for managing PWUD in a hospitalized setting include addiction care itself as well as treatment and prevention of life-threatening infections [10].
Effective identification of hospitalized PWUD is essential for epidemiological tracking, resource allocation, and evaluating interventions. However, current methodologies often fail to accurately capture this population. The “gold standard” for identifying PWUD hospitalizations is human-guided chart review, a highly regulated and time-intensive process with potential consequences for breach of confidentiality [1112]. Administrative billing codes (also known as International Classification of Disease codes, ICD codes) have been used for PWUD identification. Unlike several other common conditions such as cardiovascular diseases for which ICD-10 codes are highly accurate [1314], a systematic review found that for identification of PWUD, ICD-9/10 codes had high specificity but limited sensitivity ranging from 47%‐83% [1516]. Indicators for substance use tend to be noted in the social history section of the electronic medical record (EMR) rather than a formal diagnosis. Some researchers have used the hepatitis C virus (HCV) codes as a marker of drug use, although there are a substantial number of people with HCV who do not currently use drugs or have ever used drugs [1617].
The barrier to identifying PWUD can potentially be addressed with natural language processing (NLP), to leverage artificial intelligence (AI) algorithms for interpretation of the written text in a context-relevant manner [18]. NLP has been effectively applied to medical examiners’ reports to increase the accuracy of identifying substance use disorder-related deaths [19], identify substance use disorders in outpatients with HIV [20], and enhance preventive care for hospitalized patients with HIV [17]. In particular, regular expression (RegEx), a rule-based text-matching framework, has been used to identify text patterns [21]. RegEx has recently been used as a tool for identification of encounters with people with opioid use disorder (OUD) [22]. A few studies have examined the application of NLP to identify hospitalized PWUD admitted for bloodstream infections; however, these efforts were single-center evaluations, focused only on injection drug use [23-26]. Despite its innovative capacity to identify PWUD, the field of NLP methodology is nascent. The goal of this study was to evaluate the impact of NLP on the creation of a cohort of hospitalized PWUD and to evaluate disparities in documentation.
Methods
Definition of PWUD
As “drug use” is a broad term, it is worth emphasizing that “PWUD” in this study includes the use of cocaine, methamphetamine, fentanyl, and heroin. We use the term PWUD to describe people in the cohort, rather than “people who inject drugs”—another term used to describe this population—because these drugs can be consumed intravenously, smoked, or snorted. We do not use the term substance use disorder (SUD), as some PWUD do not meet diagnostic criteria for SUD and may not identify as having an SUD. Although drug use can also include cannabis and alcohol, we did not include these substances in the definition of drug use.
Overview of Cohort Creation
Tufts Medical Center (TuftsMC) is a tertiary health care center located in Boston, Massachusetts, with a strong history of clinician-researcher partnerships to improve care for PWUD [52728]. A health informatics specialist (RM) queried hospitalizations likely involving PWUD at TuftsMC between January 1, 2020, and April 1, 2022, guided by specific criteria (see below). The unit of measurement was hospitalization encounters, not individual patients, even if from the same patients, which requires separate clinical considerations and presents a distinct opportunity for the implementation of evidence-based practices such as introducing medications for OUD.
The presence of any of the following criteria (ie, abbreviated with the letters B, D, M, and N) were used to qualify the hospitalizations for inclusion in the PWUD cohort:
B (Biomarkers): In line with a previous study, positive urine toxicology for drugs or medications for SUD (eg, cocaine, amphetamine, methadone, suboxone, fentanyl, opiate, oxycodone), positive HCV antibody with positive or quantifiable HCV viral load [29]D (Diagnostic codes): Presence of ICD-9 and or ICD-10 code for overdose, substance use disorders, substance-related disorders, and Hepatitis C, considering historical diagnoses and those retained in EMRs and inactivated diagnoses that did not migrate with the transitionM (Medications for opioid use disorder): Sublingual buprenorphine (suboxone or subutex) or oral methadone listed as medications in outpatient medication reconciliation, given during hospitalization, or prescribed at discharge. We noted that methadone for OUD is not a medication prescribed at discharge, but is included via discharge reconciliation [30].N (Natural language processing): An iterative list of keywords that are commonly used to describe PWUD in EMR (Table 1, Textbox 1) was refined by the study team and then provided to the health informatics specialists [31]. The RegEx patterns were used to identify keywords in the EMRs, accounting for misspellings and variations in context, with incorporation of tokenizing and parsing syntax, context embedding, and approximate string matching. These features enabled context-specific word detection that accounted for minor misspellings or aggregated words. The algorithm was run on the entire EMR, including but not limited to nursing notes, physician notes, discharge summaries, and emergency room records.
Textbox 1.List of words programmed into NLP to detect PWUD encounters.IVDU, FENTANYL, Methadone, heroin, suboxone, IVDA, drug abuse, SUD, Substance use disorder, opioid use disorder, opioid abuse, OUD, opioid overdose, illicit drugs, addicted, addict, drug addict, injection drug use, intravenous drug use, uses fentanyl, Uses heroin, PWID, abuses drugs, injects heroin, injects drugs, injects fentanyl.
In addition to the above data, each encounter also had linked demographics data (eg, age, race, ethnicity, gender), length of hospitalization, and social vulnerability index (SVI). The SVI is a tool developed by the Centers for Disease Control and Prevention, used to assess the community’s susceptibility to disasters and emergencies; it uses 16 census-based data points to help assess local communities’ need for aid before and after the disaster [32]. It evaluates factors such as socioeconomic status, disability, minority status, and areas that may need additional support during crises. It is a holistic way to represent the social and economic stability of neighborhoods. The SVI was provided as a quartile (eg, 1, 2, 3, 4), with 1 representing the highest level of social vulnerability. Using the Stata software (version; StataCorp), we examined the association between key indicators (ie, race and SVI) and the level of documentation for SUDs.
Data Analysis
Hospitalizations were classified based on the combination of domains (ie, B, D, M, N). A percentage of charges from the D-only and N-only group was selected for chart review by two research members (EDG, TS). The number of charts reviewed was determined by feasibility and proportion to the entire cohort. Coders reviewed each chart for information that indicated drug use (excluding alcohol and cannabis). The process for determining whether a hospitalization event occurred with PWUD included: (1) assessing three types of notes in each chart—emergency department admission note, history of present illness, and discharge summary and (2) using the Epic search bar—a tool that allows for keyword search within a person’s EMR profile—for keywords (Textbox 1).. The coders conducted intercoder reliability testing after completing their first 20 chart reviews, which showed consistency. A logistic regression was performed to examine factors for drug use associated with high documentation, introduced into the cohort by the presence of all of the 4 domains (B, D, M, N) versus low documentation (NLP only).
Ethical Considerations
The study has been approved by the Health Sciences Institutional Review Board of the TuftsMC with waiver of consent granted (approval no. 2450). Identifiable data was only accessed by IRB approved study staff with approrpiate training. Identifiable data was stored on a secure file. As this was a retrospective study, there was no compensation provided to the cohort.
Results
The Venn diagram illustrates how 4548 hospitalizations involving PWUD entered the cohort based on inclusion criteria (Figure 1). The study participants’ characteristics are shown in Table 2, along with results of the multivariable logistic regression. People who identified as White or non-Hispanic had higher odds of entering the cohort through NLP alone (adjusted odds ratio [aOR]=2.07; 95% CI 1.54, 2.79). Notably, individuals from the most socioeconomically disadvantaged quartiles (1st and 2nd SVI quartiles) were also significantly more likely to enter the cohort through NLP alone (aOR=1.41; 95% CI 1.06, 1.88). The subcohorts with the highest number of hospitalizations were those with ICD codes only (D-group, n=958), biomarkers only (B-group, n=734), and NLP with all four criteria (B, D, N, M group, n=726). Approximately 10% (n=93) individuals in the D-only group and 35% (n=99) in the N-only group underwent chart review. As shown in Table 3, the positive predictive value (PPV) of the NLP-only cohort was 54%, outperforming the diagnostic codes-only cohort, which had a PPV of 43%. This demonstrates NLP’s ability to enhance identification of PWUD hospitalizations beyond traditional methods.
Venn diagram illustrating the total number of hospitalizations in each cohort. B: biomarkers; D: diagnostic codes; M: medications for opioid use disorder; N: natural language processing.
Discussion
Our study augments previous work by integrating NLP with diverse identification methods, including urine toxicology and medication records, while simultaneously addressing observed demographic disparities in documentation [23]. NLP has the potential to uncover hospital encounters with PWUD that may have previously been missed. Although NLP had greater PPV than diagnostic codes, its PPV remained low. We found that PWUD from racially and ethnically minoritized communities and those who had low income were more likely to be represented in the minimally documented cohort (ie, entry with NLP-only), rather than the maximally documented cohort.
Largely a result of stigma and racism, PWUD still do not have universal access to evidence-based treatment. Black PWUD tend to enter treatment with a more severe prognosis compared to their White counterparts, partly due to economic barriers in accessing treatment earlier [33]. Black, Latino, and Native American individuals also face additional challenges in accessing treatment for SUD due to geographic barriers, health care access, and potential community characteristics or rapport with clinicians [34]. We found that such a lack of rapport may be represented at the level of documentation for SUD; lack of SUD documentation was strongly associated with racially or ethnically minoritized identity (aOR=2.07).
Identification of PWUD who access medical care is important for several reasons. Best practice guidelines for hospitalized PWUD include management of substance use disorder, pain, and acute infection, testing and management for HIV and HCV, vaccinations for hepatitis or other relevant infections, and prevention of HIV with medications [1035]. In this study, we applied NLP retrospectively. Following previous studies that identified low HIV testing rates, we plan to use NLP to augment PWUD cohort creation in a study examining patterns of HIV testing [2736]. NLP could indeed become a valuable tool for identifying PWUD before discharge, facilitating intervention during hospitalization if EMRs could use NLP to trigger clinical decision support tools that trigger clinicians to consider SUD treatment, prescribe overdose prevention medications at discharge, order labs to prepare for pre-exposure prophylaxis, or offer vaccine services.
As we consider this study in the larger context of improving health equity, we believe that the next step would be refining the NLP system by adding more keywords, including and excluding certain conditions and medications, and conducting analyses on false positives and false negative cases. This study should be replicated in other medical centers across the United States; its wider application across various hospitals, encapsulating diverse populations and regions, will be instrumental. This study also has multifaceted applications, spanning epidemiological tracking, optimizing hospital resource utilization, and influencing the design of specific interventional studies. This study’s findings could serve as a launchpad for integrated care for PWUD with less prejudice and inequity. ReGex is a relatively fundamental AI technology, and as more advanced NLP tools become available, we envision our methodology being expanded alongside these too. Regardless of type and complexity of NLP technology, the cohorting and comparative analysis outlined in this paper can be used as a framework to assess the NLP’s performance against conventional ways of locating PWUD.
This study is not without its limitations. The NLP system, despite its effectiveness, occasionally misidentifies certain keywords. The constant calibration of the algorithm and frequent addition of keywords is needed to optimize and sustain accuracy. There are potential flaws in our characterization of domains; limitations include false positives from using ’amphetamine’ as a keyword, which unintentionally classified patients prescribed amphetamines for attention-deficit/hyperactivity disorder as PWUD. Similarly, methadone prescribed for pain management in conditions such as sickle cell disease was misclassified as OUD treatment. Achieving a balance between NLP’s inclusivity and exclusivity presents a significant challenge for this purpose. Future steps should include evaluating the NLP system’s sensitivity and specificity and iterating on the model to enhance these metrics. This will involve refining the keyword list for PWUD, enhancing the NLP algorithm to better account for common confounding variables. The field of addiction medicine is innovative and adaptive; to make NLP a meaningful clinical or research tool in this field, the NLP systems need to receive extensive training and constant input of nuanced decision-making that clinicians partake in daily. Thus, a feedback mechanism and fine-tuning to train the NLP model based on clinician feedback would be critical, fully leveraging repetitive learning, which is one of AI’s biggest strengths. Furthermore, the single-cohort design of the study may limit generalizability; therefore, future studies with streamlined cross-institutional protocols, allowing simultaneous data collection from diverse locations, would improve external validity. This study had a particular focus on comparing diagnostic codes and NLP as single identifiers of PWUD. While NLP identified PWUD with higher PPV than the diagnostic codes, it must be noted that diagnostic criteria still exceeded NLP in the actual number of PWUD cases identified. One major purpose of NLP in PWUD identification is to identify cases that are otherwise missed in conventional screenings; thus, the fact that NLP alone identified a comparable number of PWUD to diagnostic code, with a higher predictive rate, is still remarkable. Future investigation should include a more robust performance comparison between a combination of two or more PWUD clinical identification tools.
The ethics of improving identification of PWUD requires careful consideration. Medical records indicating drug use may become a source of discrimination, compromise job security, housing, and ability to care for family. To mitigate these risks, institutions should implement strict policies ensuring that NLP findings are used solely for improving patient care. Members of this research team collaborated with a broad group of experts including people with lived experience of SUD on a study outlining some of the potential pros and cons of improving systems to identify PWUD with the creation of an additional ICD-10 code for injection drug use [37]. Future work should proactively incorporate the perspectives of individuals with lived experience of SUD. Furthermore, broader discussion regarding AI’s role in health care is needed for effective, ethical, and productive clinical implementation: “Should NLP be a “wide net” or “precision tool” when locating PWUD and connecting them to the care they need?”
Despite these limitations, we believe that this study helps frame the future of systems for measuring health care delivery to PWUD. Hospitalization represents a crucial opportunity when nonjudgmental, trauma-informed, culturally competent care can be offered to PWUD. This presents many potential applications for NLP to be built into systems that track epidemiology and inform quality improvement and implementation science. By integrating NLP, we can advance equitable PWUD care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chiosi JJ Mueller PP Chhatwal J Ciaranello AL A multimorbidity model for estimating health outcomes from the syndemic of injection drug use and associated infections in the United States BMC Health Serv Res 07172023231760 doi 10.1186/s 12913-023-09773-1Medline 37461007 PMC 10353126 · doi ↗ · pubmed ↗
- 2Mattson CL Tanz LJ Quinn K Kariisa M Patel P Davis NL Trends and geographic patterns in drug and synthetic opioid overdose deaths - United States, 2013-2019 MMWR Morb Mortal Wkly Rep Feb 122021706202207 doi 10.15585/mmwr.mm 7006 a 4Medline 33571180 PMC 7877587 · doi ↗ · pubmed ↗
- 3Sun J Mehta SH Astemborski J et al Mortality among people who inject drugs: a prospective cohort followed over three decades in Baltimore, MD, USA Addiction Mar 20221173646655 doi 10.1111/add.15659 Medline 34338374 PMC 10572098 · doi ↗ · pubmed ↗
- 4Hollander MAG Chang CCH Douaihy AB Hulsey E Donohue JM Racial inequity in medication treatment for opioid use disorder: exploring potential facilitators and barriers to use Drug Alcohol Depend Oct 12021227108927 doi 10.1016/j.drugalcdep.2021.108927 Medline 34358766 PMC 8464525 · doi ↗ · pubmed ↗
- 5Hamdan S Smyth E Murphy ME et al Racial and ethnic disparities in HIV testing in people who use drugs admitted to a tertiary care hospital AIDS Patient Care STDS Nov 20223611425430 doi 10.1089/apc.2022.0165 Medline 36301195 PMC 9700355 · doi ↗ · pubmed ↗
- 6Westgard LK Sato T Bradford WS et al National HIV and HCV screening rates for hospitalized people who use drugs are suboptimal and heterogeneous across 11 US hospitals Open Forum Infect Dis 052024115 ofae 204doi 10.1093/ofid/ofae 204Medline 38746950 PMC 11093397 · doi ↗ · pubmed ↗
- 7Ti Lianping Ti Lianlian Leaving the hospital against medical advice among people who use illicit drugs: a systematic review Am J Public Health Dec 201510512 e 539doi 10.2105/AJPH.2015.302885 Medline 26469651 PMC 4638247 · doi ↗ · pubmed ↗
- 8Hazen A Pizzicato L Hom J Johnson C Viner KM Association between discharges against medical advice and readmission in patients treated for drug injection-related skin and soft tissue infections J Subst Abuse Treat 072021126108465 doi 10.1016/j.jsat.2021.108465 Medline 34116815 · doi ↗ · pubmed ↗