Development and Feasibility of a Smartphone Application for Promoting Healthy Heart Behaviors Following Open-Heart Surgery: A Mixed-Method Pilot Study
Preeyaphorn Songsorn, Pawarat Nontasil, Kornanong Yuenyongchaiwat, Noppawan Charususin, Jitanan Laosiripisan, Sasipa Buranapuntalug, Khanistha Wattanananont

TL;DR
A smartphone app called 'Term-Jai' was developed to help patients recover better after open-heart surgery by promoting healthy behaviors.
Contribution
The study introduces and evaluates a new smartphone application designed to support post-surgery heart health through behavior promotion.
Findings
70% of participants remained engaged with the app during the 30-day study period.
The app received an average System Usability Scale score of 80.2, indicating good usability.
Participants reported improved health behaviors and found the app's information useful and easy to understand.
Abstract
Background/Objectives: Adherence to healthy behaviors after open-heart surgery is crucial for recovery and long-term health. Traditional patient education methods can be enhanced by using technology to improve engagement and self-care. This study aimed to develop and assess the feasibility of the “Term-Jai” smartphone application for promoting healthy heart behaviors in open-heart surgery patients. Methods: The “Term-Jai” psychological theory-based application was tested quantitatively and qualitatively over a 30-day period with 13 patients (age 44–78 years) following open-heart surgery between November 2023 and March 2024. Participant engagement, healthy behaviors, user experience, and usability were assessed using the System Usability Scale (SUS), satisfaction ratings, healthy behavior questionnaires, and semi-structured interviews. Results: The application was feasible, with 70% of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
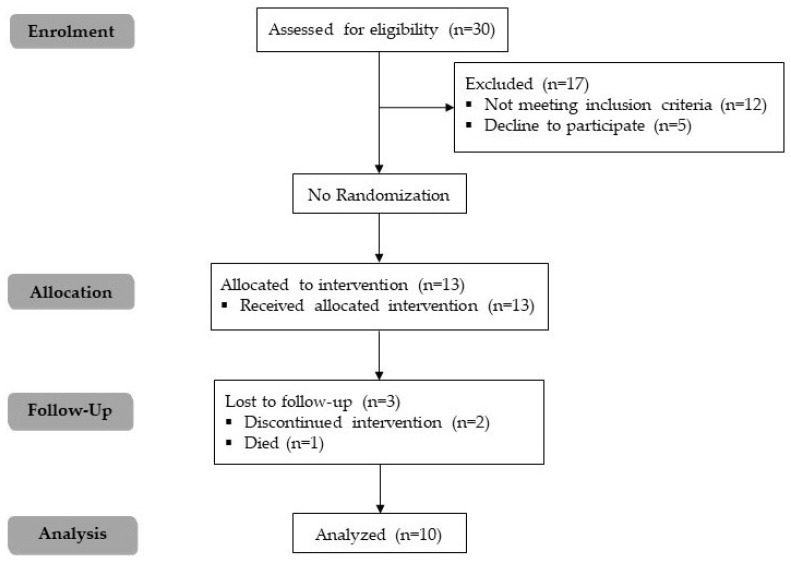 Figure 1
Figure 1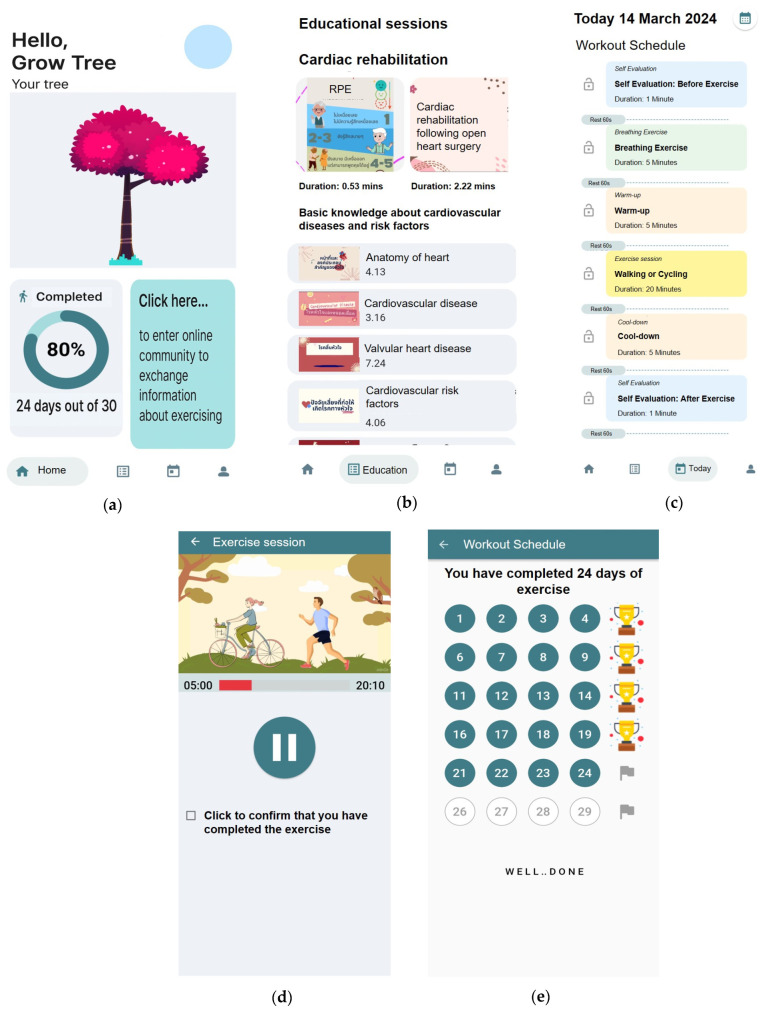 Figure 2
Figure 2- —Thailand Science Research and Innovation Fundamental Fund
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Health and Mental Health · Mobile Health and mHealth Applications · Heart Rate Variability and Autonomic Control
1. Introduction
According to data from the World Health Organization, coronary artery disease was identified as the leading cause of death worldwide [1]. In Thailand, the Ministry of Public Health’s statistics for 2021 show that, nationally, coronary artery disease is the fourth leading cause of death [2]. Treatments for coronary artery disease include medication, lifestyle adjustments, and interventions like Percutaneous Coronary Intervention (PCI) or Coronary Artery Bypass Surgery (CABG) [3]. Cardiac rehabilitation (CR) following these procedures is critical to reducing mortality and rehospitalization rates [4,5,6]. Despite its benefits, only approximately 18.3% of eligible patients in Thailand attend CR [7]. Barriers to accessing CR services in Thailand include a lack of knowledge regarding CR and its benefits, transportation issues, CR-related costs, and access to the services [8]. Ragupathi L. and colleagues suggest that utilizing mobile health technology (mHealth) for remote health monitoring and communication could help overcome these barriers and improve access to CR services [9].
Mobile health technology (mHealth), a component of electronic health (eHealth), has undergone significant advancements. Its benefits include primary and secondary prevention, personalized treatment recommendations, enhanced communication between healthcare teams and patients, enhanced access to healthcare services, patient engagement in continuous care, and real-time treatment monitoring [10]. Cruz-Ramos et al. noted the diversity of mHealth solutions for cardiovascular disease self-management, such as mobile applications for electrocardiogram monitoring, heart rate tracking, and educational tools promoting healthy behaviors like physical activity and medication adherence [11]. Furthermore, research shows mHealth’s positive impact on patient populations, including those with heart failure, arrhythmias, coronary artery disease, hypertension, and those in CR programs [11,12]. Previous research has consistently demonstrated the effectiveness of smartphone-assisted cardiac rehabilitation in improving clinical outcomes. These studies have shown that the integration of smartphone applications into cardiac rehabilitation programs significantly enhances exercise capacity, increases treatment adherence, promotes healthier lifestyle behaviors, and reduces hospital readmissions, emergency department visits, and postoperative complications [13,14,15,16]. Furthermore, such interventions have been associated with improvements in patients’ quality of life [17]. These findings provide robust evidence supporting the integration of mobile health technologies into cardiac rehabilitation programs, reinforcing their potential to improve patient engagement and adherence in both clinical and home-based settings. This study aimed to develop and evaluate the feasibility of a smartphone application to promote adherence to healthy heart behaviors following open-heart surgery.
2. Materials and Methods
2.1. Study Design
This study used a mixed-methods design, integrating quantitative and qualitative approaches, to explore the feasibility of a smartphone application to promote adherence to healthy heart behaviors in patients who underwent open-heart surgery. A research assistant provided participants with a brief educational session on application usage. Participants completed a user satisfaction and usability questionnaire and were interviewed by phone after 30 days of application usage.
2.2. Application Design
The application aims to encourage users to transition from procrastination to routine behavior and habit formation. Procrastination, defined as a failure of self-control or self-regulation, involves conscious or unconscious decisions that delay task completion [18]. Causes include lack of motivation, poor time management, and negative emotional states, and can result in adverse outcomes such as unhealthy behaviors [19,20].
The application’s design uses the Fogg Behavior Model [21], which states that motivation, ability, and triggers must coincide for a target behavior to occur. Ideally, a target behavior occurs when it requires minimal effort and high motivation. Users are prompted to complete easy daily tasks and are rewarded upon task completion to boost motivation.
2.3. Application Development Process
The application was developed between January 2023 and July 2023, using the Analysis, Design, Development, Implementation, and Evaluation (ADDIE) model [22]. The analysis phase involved a comprehensive literature review to identify clinical guidelines, behavior change strategies, and mobile health trends relevant to CR. This was followed by a comparative analysis of existing CR applications to assess common features and user limitations, which informed the application’s functional and educational requirements. The design phase focused on conceptualizing the application’s two main components: promoting daily physical activity through guided exercise and delivering structured health education on cardiovascular disease management. During the development phase, the application was built for the Android platform using the Dart programming language and Flutter framework, following the learning objectives and the structure outlined in the analysis and design phases. The first version of the application was evaluated by three experts (two physiotherapists and one cardiothoracic surgery nurse) with over five years of CR experience. Following revisions, the implementation phase involved distributing the application via smartphone and conducting evaluations post-usage.
2.4. Participants
The participants in this study were individuals who underwent open-heart surgery at Vajira Hospital in Thailand between November 2023 and March 2024. Eligible participants were 20–80 years old, had an Android smartphone, and completed the inpatient cardiac rehabilitation phase (Phase I CR program). Participants with cognitive impairment or postoperative complications such as respiratory infections, wound infections, and unstable vital signs, were excluded. This study was approved by the Institutional Review Board of the Faculty of Medicine, Vajira Hospital (COA no.177/2566). The Thai Clinical Trials Registry number is TCTR20231017008. All of the participants in the study provided informed consent. Written consent was obtained from the participants for the publication of this paper.
2.5. Feasibility, Data Collection, and Outcome Measures
The feasibility study evaluated the application’s usability, user satisfaction, and engagement. Participants were required to use the application at least five days a week for 30 days. After 30 days of usage, participants completed the questionnaires in a paper-based format. The System Usability Survey (SUS) to assess the application’s usability. The SUS consisted of ten items and was adapted from a previously validated version [23], which scored on a 5-point Likert scale. The final score ranged from 0 to 100, with higher scores indicating better usability. Participants also completed an 8-item satisfaction questionnaire to evaluate the participants’ experience with the contents and design of the application throughout the study. The user satisfaction questionnaire was adapted from a previous research study [24]. Each item was scored on a 5-point Likert-type scale ranging from 1 (not satisfied at all) to 5 (extremely satisfied). The application’s acceptability was further evaluated through semi-structured interviews (Table 1).
Improvements in health behavior were evaluated using a questionnaire adapted from a previously published study [25] which focused on cardiovascular disease risk behaviors. Responses were rated on a scale from 1 (no engagement in the behavior) to 5 (consistent and active engagement). An increase of at least one point was interpreted as an indication of positive change in health-related behavior. Participant engagement with the application was measured by the number of days they used its features for at least 20 out of 30 study days [26].
2.6. Data Analysis
2.6.1. Quantitative Data
Descriptive statistics were used to summarize participants’ demographic data, showing means, standard deviations, and proportions.
2.6.2. Qualitative Data
A content analysis of the semi-structured interview transcripts was conducted to assess their usability using thematic analysis [27]. To ensure the accuracy and reliability of the data, the transcripts were rigorously cross-checked against the original audio recordings. Key statements reflecting the experiences and perceptions of participants were identified and systematically coded. Each newly generated code was compared with previously established ones, eventually forming subthemes and overarching themes. Finally, the themes were refined, and the core aspects of the application’s feasibility in practical implementation.
3. Results
A total of 30 participants were assessed for eligibility, of which 12 did not meet the inclusion criteria, and five declined to participate for personal reasons. As a result, 13 participants were enrolled in the study. Three participants dropped out, two discontinued the intervention for personal reasons, and one died for reasons unrelated to this study (Figure 1).
3.1. Development of the Smartphone App
The “Term-Jai” (meaning “fulfilled heart” in Thai) application was designed to be user-friendly. According to the ADDIE model, the analysis phase identified key limitations in previous apps, including a lack of guided exercise content, minimal user engagement features, and limited educational support. These findings informed the definition of user needs and learning objectives for the application, emphasizing simplicity, motivation, and comprehensive CR support. Based on this analysis, the application was designed with two primary components: a daily exercise module and a set of educational sessions. These components include three main features: a daily exercise plan, exercise progress tracking, and educational content. The daily exercise plan involves self-assessment before and after each session using the rated perceived exertion (RPE) scale, along with video guides for breathing exercises, warm-up, main exercise sessions, and cool-down. A visual representation of a growing tree and a green circle appears upon daily completion of the exercise. Participants receive a trophy after completing five sessions in a week, recognizing their exercise progress. The educational sessions incorporate video and audio media covering basic knowledge about cardiovascular diseases, associated risk factors, and CR (Figure 2). The initial prototype was evaluated by experts, whose feedback led to improvements in video quality, text size, clarity of visual instructions, and consistency of the user interface layout. The revised application was then implemented on users’ smartphones for real-world use.
3.2. Baseline Characteristics of Participants
The demographic and clinical characteristics of ten participants are shown in Table 2. The average age was 60.4 ± 10.0 years and the average BMI was 25.0 ± 3.5 kg/m^2^. Most of the participants in this study were male (80%). The surgeries performed included coronary artery bypass surgery (50%), valve replacement (40%), and aortic hemiarch replacement (10%).
3.3. Quantitative Findings
3.3.1. Application Engagement
70% of participants met the engagement requirement by using the application for at least 20 out of the 30 days. One participant did not use the application regularly because of technical problems, and two participants lost interest in it.
3.3.2. Application Usability
Ten participants completed the SUS after 30 days, with a mean score of 80.2 ± 10.3 (range 70–92.5) out of 100. Table 3 shows the five-point Likert scale scores for the ten SUS questions.
3.3.3. Application User Satisfaction
Table 4 lists the mean values of user satisfaction with the “Term-Jai” application’s content and design. The average participant satisfaction score was 4.3 ± 0.6 out of 5. All participants stated that the application’s information was useful; 90% said it was clear and easy to understand and felt that the content quantity was appropriate. Moreover, all participants stated that the screen color was appropriate, 80% found that the application made learning easy and that the font size was appropriate, and 60% said that the overall composition of the application was appropriate.
3.3.4. Healthy Behaviors Improvement
All participants improved their health behaviors (Table 5), including more exercise, increased consumption of vegetables and fruits, reduced salt intake, and decreased consumption of high-fat and high-sugar foods. They also managed stress better. However, smoking cessation and alcohol consumption remained unchanged.
3.4. Qualitative Findings
Based on semi-structured interviews, the participants identified four main themes: appropriate application content, appropriate application design, barriers to use, and suggestions for improvement. Most participants were satisfied with the application content, finding it beneficial, especially for exercise programs and educational sessions. Participants also found that the application was user-friendly. However, some participants reported technical issues, and others offered useful suggestions for improvement. The themes, subthemes, and participants’ interview quotes are presented in Table 6.
4. Discussion
This study aimed to develop and investigate the feasibility of the “Term-Jai” smartphone application to promote adherence to healthy heart behaviors following open-heart surgery. Quantitative and qualitative data revealed that the “Term-Jai” application was feasible for improving healthy heart behaviors.
The findings of this study align with existing studies on the development of smartphone applications for patients recovering from cardiac surgery [12,28,29]. Previous studies demonstrated high engagement with applications in peri-operative cardiac surgery patients [28] and patients enrolled in CR [12]. These findings align with the present study, which showed that 70% of participants remained engaged with the “Term-Jai” application over a 30-day intervention. However, the engagement in this study was higher than that in a previous study on cardiovascular diseases [29]. This difference may be due to the variant psychological strategies used in this study, such as gamification strategies, tree growth visualization, green circle visualization, and trophies. Gamification strategies effectively promote behavior change by making health-related activities more engaging and motivating participants to use the application consistently [30].
Some participants had low engagement with the “Term-Jai” application. One participant cited technical issues, and two others stated that they could remember the content and perform the exercises without using the application. These findings are consistent with a previous study that demonstrated low adherence to application usage due to technical difficulties and lack of interest [31]. Additionally, after initially engaging with a digital intervention, users might achieve adequate self-regulation, making the application unnecessary [32]. Providing technical support and personalized exercise progression could increase engagement with the application.
The average SUS score was 80%, indicating a good user experience and supporting the “Term-Jai” application’s usability [33]. All participants found the application’s information useful, with most stating it was easy to understand and clear. A qualitative analysis of the interviews provided further insight into the application’s benefits. The mean participant satisfaction score was high, emphasizing its potential as an effective CR tool. Participants gave high ratings to the application’s design, emphasizing the importance of an intuitive and aesthetically pleasing interface. A well-designed application can significantly enhance user experience, making it easier for patients to navigate and access the necessary information [34]. This is particularly relevant for elderly Thai users, who often face challenges in adopting technology due to difficulties navigating complex digital tools [35]. To address this, our application is designed as a simple, user-friendly solution tailored to this demographic, ensuring accessibility and ease of use. However, some technical issues were noted, indicating the need for continuous technical support. Some participants also suggested improvements, such as adding more interactive features and enhancing exercise customization options to better tailor the application to individual recovery needs. Implementing these suggestions could further enhance the application’s utility and user satisfaction.
One of the primary benefits of this feasibility study was improved healthy behaviors. The development of this application aligns with growing evidence supporting the use of mobile health technologies to promote healthy behaviors among individuals at risk of or living with cardiovascular disease [36,37]. The present application contributes to this movement by offering accessible tools to support daily exercise, self-assessment, and comprehensive educational materials on surgery, recovery, potential complications, and lifestyle modifications. Increased patient education is associated with better self-care practices and health outcomes [38,39]. Additionally, gamification was shown to affect health outcomes positively [40]. However, smoking and alcohol consumption did not change after the intervention, as only one participant was a current smoker, and none consumed alcohol.
This study had some limitations. First, the relatively small sample size may restrict the generalizability of the findings; however, the results can serve as preliminary data for future research. The absence of a control group limits the ability to attribute improvements solely to the application. Additionally, open-heart surgery patients were not involved in the application development process; hence, their needs and preferences were not directly incorporated. The male-dominant composition of the sample also presents a limitation, as men have been shown to respond more strongly to perceived usefulness in technology adoption [41]. This demographic distribution may limit generalizability. Additionally, due to time and budget constraints, the application was only developed for the Android platform, was deployed within a single-center setting, and lacked personalization features.
Despite these limitations, the study offers meaningful contributions. While the level of technological innovation may be considered moderate, the strength of this study lies in its integration of functionality with accessibility. It addresses a critical gap by providing structured, guided exercise sessions and essential cardiovascular education through a simple, intuitive interface. These features are particularly significant for older adults or patients with limited health and digital literacy, who are often excluded from high-tech solutions.
Future research should focus on larger patient populations and conduct multi-center randomized controlled trials (RCTs) to validate these findings and explore the long-term impact of the application on clinical outcomes such as blood pressure, cholesterol levels, or physical fitness level. Steps are being taken to develop an iOS-compatible version of the app to broaden accessibility, and to recruit more diverse participants across urban and rural healthcare settings with a balanced representation in terms of gender, age, and comorbidities. In addition, incorporating user feedback will guide enhancements such as exercise customization, interactive features, and improved personalization to better address individual recovery needs. Technical refinements, including offline functionality, performance optimization, and robust user support services (e.g., in-app help centers, AI chatbots, and live support), are essential to ensuring a seamless and user-friendly experience. Future iterations may integrate additional modules, such as dietary tracking, medication adherence support, and mental health resources, offering a more holistic approach to cardiac rehabilitation. Further investigation into the app’s cost-effectiveness and its potential to reduce healthcare utilization is also warranted. Lastly, the integration of AI-driven personalized recommendations presents a promising direction for enhancing patient engagement and outcomes.
5. Conclusions
The study demonstrated that the “Term-Jai” smartphone application could be a valuable tool for supporting postoperative care in open-heart surgery patients. High patient satisfaction and positive feedback on the application’s content and design suggest that it could enhance recovery by providing easily accessible information. Addressing barriers and incorporating patient suggestions is crucial for the application’s ongoing development and effectiveness.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization The Top 10 Causes of Death Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death(accessed on 4 March 2022)
- 2Office of the Permanent Secretary Ministry of Public Health Public Health Statistics A.D. 2021 Ministry of Public Health Nonthaburi, Thailand 2021
- 3Lawton J.S. Tamis-Holland J.E. Bangalore S. Bates E.R. Beckie T.M. Bischoff J.M. Bittl J.A. Cohen M.G. Di Maio J.M. Don Creighton W. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization J. Am. Coll. Cardiol.202279 e 21e 12910.1016/j.jacc.2021.09.00634895950 · doi ↗ · pubmed ↗
- 4Ghisi G.L.d.M. Chaves G.S.d.S. Bennett A. Lavie C.J. Grace S.L. The Effects of Cardiac Rehabilitation on Mortality and Morbidity in Women: A Meta-Analysis Attempt J. Cardiopulm. Rehabil. Prev.201939394210.1097/HCR.000000000000035130252785 · doi ↗ · pubmed ↗
- 5Graham H.L. Lac A. Lee H. Benton M.J. Predicting Long-Term Mortality, Morbidity, and Survival Outcomes Following a Cardiac Event: A Cardiac Rehabilitation Study Rehabil. Process Outcome 20198117957271982761010.1177/117957271982761034497458 PMC 8282132 · doi ↗ · pubmed ↗
- 6Medina-Inojosa J.R. Grace S.L. Supervia M. Stokin G. Bonikowske A.R. Thomas R. Lopez-Jimenez F. Dose of Cardiac Rehabilitation to Reduce Mortality and Morbidity: A Population-Based Study J. Am. Heart Assoc.202110 e 02135610.1161/JAHA.120.02135634612055 PMC 8751887 · doi ↗ · pubmed ↗
- 7Raungratanaamporn S. Yunibhand J. Jitpanya C. Factors predicting physical activity after hospitalization among new coronary artery disease patients J. Health Res.201529127133
- 8Kotcharoen R. Tower M. Boyde M. Eley R. Facilitators and Barriers to Cardiac Rehabilitation Uptake Among Patients with Coronary Artery Disease in Thailand: A Qualitative Study ASEAN J. Rehabil. Med.2024348595