Breast Cancer Survivors’ Perception on Health Promotion and Healthy Lifestyle: A Systematic Review and Qualitative Meta-Synthesis
Luca Guardamagna, Orejeta Diamanti, Giovanna Artioli, Lorenzo Casole, Matteo Bernardi, Francesca Bonadies, Enrico Zennaro, Gloria Maria Modena, Tiziana Nania, Federica Dellafiore

TL;DR
This study reviews how breast cancer survivors view health promotion efforts to prevent recurrence and improve outcomes after treatment.
Contribution
It provides a qualitative meta-synthesis of survivors' perceptions on health interventions to reduce recurrence risk.
Findings
Five themes emerged: challenges, self-motivation, relationships, barriers to change, and proactive support.
Tailored interventions and social support are crucial for improving health behaviors and outcomes.
Internal and external factors influence adherence to health promotion strategies.
Abstract
Aims: To systematically review and synthesize qualitative research exploring the Breast Cancer Survivors (BCSs)’ perception of health promotion interventions and informing strategies to mitigate recurrence risk within five years post-treatment and improve clinical outcomes. Specifically, this study addresses the question: “How do women diagnosed with breast cancer perceive health promotion interventions for recurrence prevention?” Design: A systematic review and qualitative meta-synthesis were performed. Data Sources: A systematic search of scientific databases (CINAHL, MEDLINE, and Scopus) was undertaken in November 2024. The reference list was cross-referenced and hand-searched to identify additional articles. Review Methods: Studies were included if they met the following criteria: they were primary qualitative studies focusing on BCSs within five years post-treatment, involving…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
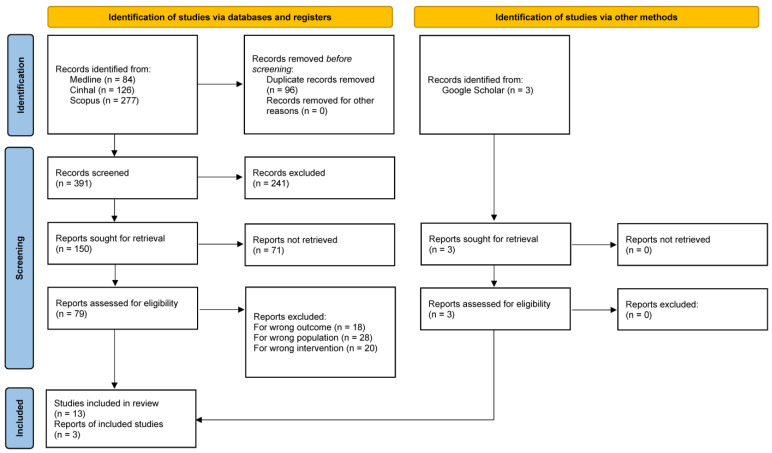 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer survivorship and care · Women's cancer prevention and management · Cancer-related cognitive impairment studies
1. Background
Breast Cancer (BC) is the most prevalent malignancy among women worldwide and remains the leading cause of cancer-related mortality [1]. In 2020, 2.3 million women were diagnosed with a BC [1], and it has been estimated that 3.2 million women will receive a BC diagnosis by 2050 [2]. BC is hugely devastating [3] and has a high and vital impact on quality of life, and both physical and psychological patient outcomes [4]. In particular, women facing BC are often exposed to anxiety and depression after diagnosis [5], and the stress of living with the fear of relapse is their biggest burden [6].
Recurrence, defined as the reappearance of malignancy following initial treatment, marks a deterioration in clinical prognosis and contributes to significant psychological distress among Breast Cancer Survivors (BCSs). According to the National Cancer Institute, a Sis an individual who has completed primary treatment and is living either with or without evidence of the disease. This broad definition includes both those in long-term remission and individuals managing ongoing challenges related to the disease. Recurrence is further defined as “cancer that has recurred (come back), usually after a period of time during which the cancer could not be detected” [7]. Recurrence rates remain clinically relevant, with a pooled recurrence proportion of 12.2% within 1–4 years post-diagnosis, increasing to 14.3% between 5 and 9 years, and reaching 23.3% after 10 or more years [8]. Given the rising global incidence of BC [1], and the increasing risk of recurrence over time—especially in certain subtypes and stages—the long-term risk represents a major public health concern.
Recent evidence suggests that health-promoting behaviors, such as regular physical activity, healthy nutrition, and weight management, play a significant role in reducing the risk of BC recurrence within the critical first five years following primary treatment and improving long-term survival [9,10,11]. This timeframe is critical, as it represents the follow-up period during which the risk of cancer recurrence is highest and health promotion interventions may have the greatest impact on clinical outcomes and quality of life. Although much of the current evidence derives from studies that include survivors beyond five years post-diagnosis, these findings highlight the critical importance of adopting healthy behaviors early in the survivorship trajectory, particularly within the first five years following primary treatment, when the risk of recurrence is generally higher. This underscores the need for targeted interventions that support behavior change during this pivotal window [9,10,11].
Despite this new evidence, BCSs often do not follow recommendations, and it is estimated that 70% of them annually do not adhere to a healthy lifestyle [12,13,14,15,16]. Specifically, only 32% adhere to physical activity during their follow-up [17], and only 14% of BCSs decide to follow the correct nutrition [18]. Major guidelines for breast cancer survivors, including the ACS and WCRF/AICR recommendations, highlight the importance of adopting healthy behaviors such as regular physical activity, weight management, and balanced diets to reduce the risk of recurrence and improve overall health during early survivorship [10,19]. However, these guidelines often lack detailed specifications on optimal intensity, duration, and composition of interventions tailored for survivors within the first five years, indicating a gap that future research and clinical practice should address.
Some authors identified different reasons that could hinder changes in BCS behavior and adhesion to a healthy lifestyle [12,16]. For example, BCSs prefer to spend time with their children, not give up their nutrition habits, not stop drinking alcohol or smoking tobacco, or renounce their engagements [20,21]. Additionally, a rich qualitative literature described the BCS perceptions of physical activity, nutrition, and weight management, allowing us to understand better the reasons why BCSs do not adhere to health promotion behaviors, the difficulties encountered, and the strategic role of nurses in sustaining and promoting a healthy lifestyle [21,22,23].
Therefore, this study aims to address this gap by systematically reviewing and synthesizing qualitative research on BCSs’ perceptions of health promotion interventions. This will inform tailored strategies to mitigate recurrence risk within five years after completion of primary treatment and improve clinical outcomes. Specifically, this study uses a systematic review and meta-synthesis approach to answer the research question: ‘How do women diagnosed with BC perceive health promotion interventions for recurrence prevention?’
2. Materials and Methods
2.1. Study Design
A systematic review and qualitative meta-synthesis were performed. Specifically, to keep the original meaning of individual studies, a new, cohesive interpretation of the results was generated through meta-synthesis, a method for integrating and presenting qualitative findings [24]. This process also contributes to advancing clinical practice, informing intervention design, and supporting theory development [25].
The methodological criteria and PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart for systematic reviews (Figure 1) guided the identification of the primary literature to include in the meta-synthesis. It secured a detailed overview of the studies, while at the same time, it allows for an accurate analysis of every single research belonging to the sample [26]. Afterwards, the Joanna Briggs Institute (JBI) meta-aggregative approach in synthesizing qualitative evidence guided the included study’s synthesis [27]. The JBI approach to qualitative synthesis is designed to pragmatically identify evidence to guide clinical practice, employing a rigorous methodology [27]. This method followed a three-step process: firstly, generating statements that represent aggregated data by combining findings from qualitative studies; secondly, grouping findings into categories based on shared meanings; and thirdly, performing a meta-aggregation of the categories to create a cohesive synthesis of findings [27].
2.2. Protocol Registration
The review study protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO) of the National Institute of Health Research to straighten the study’s producibility, accountability, and transparency (CRD42024626033) [28].
2.3. Formulation of the Research Question
The search was constructed using the SPIDER (Sample, Phenomenon of Interest, Design, Evaluation, Research type) tool to define key elements of the review question better and to inform and standardize the search strategy. The SPIDER tool applied to the research question was as follows: Sample = adult women diagnosed with BC within the last five years, who completed primary treatment; Phenomenon of Interest = perception of health promotion measures, including nutrition, physical activity, and weight management; Design = phenomenology, ethnography, grounded theory or mixed-methods studies; Evaluation = effectiveness of health promotion interventions in reducing recurrence risk; Research type = literature review and synthesis [29].
2.4. Search Strategy
Tailored search strings were developed, incorporating specific keywords and Medical Subject Headings (MeSH Terms) such as Breast Cancer Survivors, Neoplasms, Meta-synthesis, Qualitative research, Experience, and point of view, with their variants. Boolean operators (AND, OR) were utilized to refine the search, and search strings were to adapt to each database’s requirements, ensuring efficient literature retrieval. Two independent reviewers (LG; FD) systematically searched three databases that provided broad coverage in nursing and medical domains: CINAHL, MEDLINE, and Scopus. MeSH and free-text words were listed to construct the search strategy, which was explicitly adapted to the syntax of each database as appropriate (Table 1). The reference list was cross-referenced and hand-searched to identify additional articles [30]. Theses, dissertations, abstracts in proceedings, systematic reviews, and other unpublished papers were excluded, as they are not subjected to a peer review. The review included articles published from January 2015 until November 2024.
2.5. Eligibility Criteria
SPIDER framework guided article selection [29]. The inclusion criteria were (a) articles (published and in press) consisting of primary studies focused on BCSs within the follow-up period of up to five years after the completion of primary treatment; (b) participants—defined as breast cancer survivors—who had completed surgical, radiotherapy, or chemotherapy treatments; (c) primary qualitative research, utilizing phenomenology, ethnography, grounded theory, or mixed methods (d) articles containing abstracts, (e) published in the Italian, English, French and Spanish language in peer-reviewed journals, and (f) full-text availability. Language restrictions were set to minimize any potential misinterpretation of the results.
Specifically, in this systematic review, we aimed to include studies investigating health promotion behaviors among breast cancer survivors (BCSs) across a broad survivorship continuum. We considered studies enrolling BCSs at various time points post-diagnosis, ranging from early survivorship (within 5 years of diagnosis or remission) to long-term survivorship (beyond 5 years). This approach was chosen to capture the dynamic nature of survivors’ motivations, barriers, and adherence patterns, which may change over time. When the exact duration since diagnosis or remission was not explicitly reported, studies were included if they otherwise met the inclusion criteria regarding population and outcome measures relevant to health promotion behaviors. Several included studies involved long-term survivors, with remission durations extending up to approximately 10 years or more. We intentionally retained these studies to provide a comprehensive and nuanced synthesis that reflects the heterogeneity of the BCS population and the evolving challenges in maintaining health-promoting behaviors throughout survivorship.
2.6. Data Selection and Extraction
Firstly, to support the screening organization and management, all records identified by databases were imported into Rayyan-Intelligent Systematic Review-software [31] (Version 7). The Rayyan^®^ platform is designed to optimize and streamline workflows for systematic reviews [31]. The process involved both automated and manual methods within Rayyan to remove duplicates, ensuring a thorough elimination of redundant records. After that, two authors independently (LG and LC) conducted a preliminary screening of the literature search by reviewing the titles and abstracts, followed by an in-depth examination of full texts. The assessment was conducted independently and anonymously by two reviewers to determine the relevance of the studies to the predefined research questions. Any conflicts were resolved through consultation with a third author (OD). The authors debated the reasons for inclusion or exclusion and disagreements to ensure reliability and consistency. The eligible articles selected during the title and abstract screening phase were then individually reviewed in full by the two authors [32]. Disagreements between the two authors were resolved during this phase through discussion with the goal of reaching a consensus. The structured approach guaranteed the selection of studies for review to be meticulous and unbiased.
2.7. The Methodological Quality of Studies
The JBI Critical Appraisal Checklist for Qualitative Research was used to assess the methodological quality of the studies [33]. The 10 items were evaluated using the following criteria: “yes,” “no,” “unclear,” and “not applicable.” The criteria evaluate the alignment between the study’s theoretical perspective, research methodology, data collection, analysis, and interpretation, while also ensuring that the researcher’s influence, ethical considerations, and participants’ voices are appropriately acknowledged and represented [33]. The tools were widely recognized for evaluating various research designs and allowed for a structured evaluation of study quality and relevance. Specifically, the evaluation results were determined based on the number of items meeting the standard requirements. Studies were classified as weak if the number of “yes” responses was ≤6, medium if between 7 and 8, and high if between 9 and 10. Only studies with at least a medium rating were included for data extraction and synthesis. Two reviewers (LG and FD) independently appraised the studies, with any disagreements resolved by a third reviewer (OD) to achieve consensus.
2.8. Data Analysis and Synthesis
Data from each study were systematically extracted into a standardized table summarizing key characteristics, including references, study purpose, design, and methodology with sample characteristics, key findings, and conclusions. The extracted data were synthesized to identify recurring themes and commonalities across the selected studies, with a thematic analysis conducted to derive meaningful insights. Data were meticulously extracted for qualitative studies to include codes, categories, and interpretations from the original study authors. These extracted data were abstracted into codes and subsequently consolidated into overarching themes or delineated into sub-themes where analytically appropriate. A synthesis of BCSs’ perceptions and the impact of health promotion interventions on recurrence prevention was encapsulated by the resulting themes.
3. Results
3.1. Study Selection
According to the PRISMA framework [26] that ensured a systematic, transparent, and comprehensive approach to identifying and analyzing the relevant literature, Figure 1 represents the screening methodology process for the identified studies. The literature search identified 490 records: 487 articles have been retrieved from databases CINAHL, MEDLINE, and Scopus, while 3 articles were identified through websites and citation searching. Before the screening started, 96 duplicate records were removed. Then, 394 records were screened based on title and abstract. Accordingly, 241 records were excluded because their content did not meet the inclusion criteria: they were not based on research methodology or not related to the research question. Then, of the 153 included records (150 from databases and 3 from other research), 71 were excluded because they were not retrieved (abstract or conference presentation). So, 82 full-text articles were screened for eligibility (79 from databases and 3 from other research), and 6 were excluded for the following reasons: 18 reported other outcomes, 28 described other populations, and 20 described other interventions. No study was excluded based on the quality critical appraisal tool. Finally, 13 articles from databases and 3 articles identified via other methods (web and citation searching) were included in the last PRISMA phase (Figure 1). The 16 included articles were analyzed using a narrative synthesis approach [34].
Table 2 shows the key characteristics of each included studies, such as aim, design, and methodology with sample characteristics, results, and conclusions, and Table 3 focuses on the description of various study qualitative design and sample features included.
3.2. Characteristics of the Included Studies
As represented in Table 3, the studies were conducted worldwide. All of them employed a qualitative design, emphasizing multiple specific approaches to explore BCSs’ nuanced experiences. Some studies used interpretive frameworks [10,35,36,37,38,39,40,41,44,45,46,47]; two studies adopted inductive and reflexive methods to identify themes from participant narratives [43,49], while Mehrabi et al. (2016) used a phenomenological design [50]. The total number of BCS patients enrolled in the 16 studies included was 230. The reported age range of participants spans from 18 to 72 years, reflecting the inclusion of both younger and older BCSs (Table 3).
Semi-structured interviews were the primary data collection method, valued for their flexibility in addressing specific topics while encouraging participant insights [35,36,37,38,39,40,41,43,44,45,46,47,49,50]. Instead, two studies used focus groups to provide collective insights, though influenced by group dynamics [42,48].
With regard to the methodological quality of included studies, most studies demonstrated strong methodological integrity and achieved rich data saturation, further supporting the reliability of the findings. Specifically, as showed in Table 2, the JBI Critical Appraisal Checklist for Qualitative Research of included studies was high, having a number of “yes” responses between 9 and 10 [33] Table 4.
The sample’s full text led to the identification of five main themes: (I) Challenges, (II) Self-motivation and Empowerment, (III) Relationships as a Facilitator, (IV) Barriers to Change, and (V) Proactive Support Strategies.
3.2.1. Theme I: Challenges
The first theme emphasizes BCSs’ challenges in their commitment to health promotion. Generally, BCSs were determined to adopt behaviors that might mitigate recurrence risk, such as adhering to regular and intense physical activity programs, and to learn exercises suitable for their condition, start eating properly at all meals, and understand the correct foods to eat [49]. But this should not be overlooked. Some survivors faced conflicts between maintaining dietary discipline and the social aspects of eating, as one participant remarked “I don’t want to be like ‘No, I actually can’t eat because of dietary restrictions that I put on myself because I’m fearful that my cancer’s going to come back’” [36]. Structural constraints, such as time conflicts and familial responsibilities, further compounded the issue, with a young mother stating “I probably wouldn’t participate [in a physical activity program] because I don’t want to miss out on [family] time” [36], underlining the criticality of giving priorities: spend time with your children or join programs. Indeed, most BCSs do not take time away from their children to train, but at the same time, they do not want to give up their health either: “Me being a young mom, I’m not [physically active]. I don’t want to miss out. My son goes to school, and if it [a physical activity program] is any time during his time at home, I probably won’t participate because I don’t want to miss out on that time” [36]. The physical exhaustion associated with survivorship was a recurring theme, as one participant explained “Usually I’m okay, but some days, I feel like I’d faint… When exhausted, you have to sleep… Can’t go out, it’s just like ‘playing dead” [48]. Furthermore, the psychological burden of cancer survivorship was widespread, with one participant stating “Every day is a battle with the fear of recurrence. Even if I feel fine, the thought is always there” [50]. Physical and emotional struggles, however, remained significant. The challenges that BCSs faced were related to their self-image and the long-term effects of treatment. One survivor described the impact of chemotherapy on her body, saying “I felt more pain in my body after chemotherapy… it caused me worry that if the pains and disabilities continue forever” [50]. Others struggled with body image issues, as one survivor shared “I took a shower without turning the light on for 2 months. I didn’t want to see it [my body]” [42]. The BCSs’ efforts to embrace health-promoting behaviors are multifaceted, which are highlighted by these challenges.
3.2.2. Theme II: Self-Motivation and Empowerment
Despite significant challenges experienced, many women were determined to adopt behaviors that might mitigate recurrence risk. In this process, motivation is a positive or negative determinant factor. One BCS shared the importance of physical activity: “I’m finding it hard to stay active as my motivation is way low… Then days pass until I say I have to get to it again” [41]. On the contrary, a 62-year-old BCS in Fang and Lee’s (2016) study asserts “Now I want to change and think of [eating] all kinds of foods. […] Ah, we are scared of relapse, so we try to eat some alkaline items” [37]. Another survivor also reflected on the impact of dietary changes, stressing the importance of self-motivation: “In the past, I wouldn’t be able to get through a 10-hour day, but now I can. I’m tired by the end of the day, but not mentally tired, so eating the right foods is helping my mental status” [38].
Regarding physical activity, another BCS states “Because of [BC], we must exercise; otherwise, you just lay there or sit here, which cannot be good. I have to get out and exercise or occasionally clean the house” [37]. Physical exercise has an essential mental benefit, too: “You really need to focus on mental benefits of exercise for BC, and control is a big issue too. You are dealing with not being in control, but exercise is something you can do” [40]. Structured programs recognized strong motivation: “Knowing that I was part of a structured program kept me going. The encouragement I received made me want to do better for myself” [39].
Additionally, making healthier choices improved their sense of empowerment: “Knowing that I could influence my recovery with better choices motivated me to eat more healthily” [50]. Similarly, the diagnosis itself served as a pivotal moment for self-awareness, with a participant noting “It [cancer diagnosis] made me very conscious of the control I had of my health after the treatment had finished” [43].
3.2.3. Theme III: Relationships as a Facilitator
The third theme defines the importance of relationships: social support and empathetic healthcare providers were prominently highlighted as BCSs’ survivorship facilitators. Participants affirm that having trusted people to talk to is essential to improve their response to diagnosis treatments and to increase adherence to health promotion. Specifically, social support and peer connections offered emotional solace and practical advice, as one survivor noted “You met a lot of other people [at a support group] who were able to tell you things that they found useful or didn’t find useful” [43].
Innovative support mechanisms, like shared cooking classes or group exercise programs tailored to survivors, have been proposed as effective ways to promote a sense of community and support [36]. Therefore, one participant shared that those social interactions also mitigated feelings of isolation: “My neighbours are very kind and comforting. They always ask me to go outside, and they chat with me” [35].
On the other hand, self-care can be hindered by a support network that lacks companionship for activities such as physical exercise. As one participant noted, “Not having someone to go with, that prevents me from doing it [physical activity] sometimes” [41]. Empathetic healthcare providers were also essential, as their attention to BCS patients provided emotional security. One participant expressed “If the doctor cares for me, I feel okay; thus, I am not afraid when the doctor is present” [37]. Furthermore, another BCS affirmed “Once, after I had a very long day, I grabbed a nurse and just started to express all the things that made my life so hard, and at some point, I found this nurse’s tears dropping on me! I was so touched and felt grateful to her, a huge help it was” [48].
3.2.4. Theme IV: Barriers to Change
The results of the included studies frequently identified several barriers to adopting health-promoting behaviors. Firstly, the misinformation and lack of guidance are often experienced by BCS: “In this regard, we did not receive sufficient training. I do not know what food is good for me” [44]. Other patients expressed dissatisfaction with structured dietary programs, highlighting personal preferences as a challenge: “Some of the meals didn’t taste great, and it was hard to eat things that I wasn’t used to. I wished the meals were more tailored to my preferences” [39]. Additionally, physical exercise can be hindered by physical and logistical challenges, making it necessary to use tailored programs. One participant emphasized the importance of exercises suited to their physical limitations: “It would be excellent to have a program that considers that and helps with stretching and such” [48]. Another prevalent theme was the absence of structured support during and after treatment: “I didn’t get any of this information through treatment” [40]. For some, the absence of post-treatment guidance felt isolated: “It was like being pushed into the sea from shore on a boat with no oars … what now? What do I do? … I’ve had to do all this myself, and I don’t think that’s right” [43]. Fatigue and emotional exhaustion became significant barriers as well. One participant noted, “I felt exhausted… I had no energy, so I went to a well-being centre far away from my house” [48]. Emotional challenges, such as body image struggles and strained relationships, appear to worsen the situation. Women shared “When I look in the mirror, I don’t see the breast I should have had. I’ve accepted it. My husband has also accepted it. But it is still difficult” [46]. Finally, financial hardships also emerged as a barrier to accessing treatments or therapies that could aid in health promotion, as one participant lamented “My pension is not sufficient to pay for my medicine and treatment” [44].
3.2.5. Theme V: Proactive Support Strategies
Fortunately, women’s experiences identified many proactive support strategies for adopting a healthy lifestyle, especially to compensate for support gaps, emphasizing the importance of tailored interventions to promote sustainable health behaviors. BCSs can benefit from joining the health promotion program. It increases their physical performance and improves their body’s emotional and physical condition; it positively impacts life despite the diagnosis of BC. This is possible thanks to the information provided by dieticians and trainers regarding nutrition and physical activity that they must carry on having a healthy lifestyle [39]. “We need regular exercise” [35] and “I [need] sports. I try eating healthy food” [47]. Another participant in Kim’s (2020) study shared “[…] we do need to raise the arm and use it for exercising. It would be excellent to have a program that considers that and helps with stretching. […] I think we need a light-intensity program” [42]. Women’s organizational skills could help them maintain a healthy lifestyle after surgery, as they must manage work, medical visits, and other events, as well as physical activity and food preparation. In addition, they must address symptoms that could decrease the body’s response: fatigue, joint pain and swelling, dizziness, nausea, tingling, and asthenia are the most common. The changes associated with diagnosis and treatment cause increased mental strain that negatively impacts BCSs, sometimes causing difficulties in planning their diet. An alternative solution to having a healthy lifestyle emerged from the studies include asking family members for help and preparing the daily routine by scheduling all the commitments so that BCSs can have time for self-care. Alternative strategies, such as consuming anti-cancer foods, were mentioned by some patients to overcome the perception of inadequate medical support: Thus, I have started consuming more fruits high in fibre and vitamins such as apples; I […] learned that fruits with fibre and vitamins could help fight free radicals, boost the immunity of the body and kill cancer cells” [45].
4. Discussion
Adopting a healthy lifestyle is a key strategy for reducing the risk of cancer recurrence in BCSs, but encouraging behavioral change remains a significant challenge for healthcare systems and providers. Understanding BCSs’ perspectives and perceptions regarding their adherence to health-promoting behaviors is crucial. Our meta-synthesis offers a comprehensive overview, helping clinicians and researchers navigate the diverse findings of primary studies and provide adequate support. The results highlight the complex factors influencing BCSs’ adherence to healthy behaviors. The five themes identified—Challenges, Self-Motivation and Empowerment, Relationships as Facilitators, Barriers to Change, and Proactive Support Strategies—reveal the difficulties and potential solutions for improving adherence to health-promoting behaviors. Despite recognizing the benefits of physical activity and dietary changes, BCSs often face emotional distress, physical exhaustion, and structural barriers, which hinder their ability to maintain these behaviors. Nevertheless, self-motivation, supportive relationships, and structured intervention programs are essential in overcoming these obstacles.
BCSs face significant challenges in balancing health maintenance with family responsibilities, particularly motherhood. The demands of caring for children and family members often leave little time or energy for self-care, making it difficult for many BCSs to prioritize their own health needs, despite understanding the importance of healthy behaviors in preventing recurrence. This internal conflict, often influenced by cultural values that emphasize self-sacrifice, can create substantial barriers to adopting health-promoting behaviors [51]. Reframing self-care as an act that benefits both personal health and family well-being, along with fostering self-compassion and emotional resilience, may offer critical support in overcoming these barriers, allowing BCSs to maintain healthy behaviors even during times of high caregiving demands [52].
The unpredictable nature of BC recurrence presents a significant challenge not only for clinical management but also for the psychological well-being of survivors [53]. This uncertainty often generates a constant state of fear and vigilance, which can undermine survivors’ confidence in their ability to maintain health-promoting behaviors over time. Survivors may struggle with feelings of helplessness and a lack of control, which can erode motivation and lead to disengagement from healthy routines, especially when the perceived risk of recurrence feels beyond their personal influence [53]. Therefore, this inherent unpredictability highlights the critical importance of developing tailored, long-term health promotion and preventive strategies that address each survivor’s unique medical risk profile, psychosocial context, and evolving life circumstances. Survivors need not only clinical follow-up but also sustained, personalized guidance that integrates emotional support, empowerment, and skills to adapt lifestyle behaviors over time, even when facing fluctuating risk perceptions or changing personal responsibilities. In this sense, shifting from a static model of survivorship care to a dynamic, individualized approach is essential. This includes providing survivors with tools to cope with uncertainty, strengthen self-efficacy, and maintain resilience. For example, psychoeducational programs that combine health literacy with stress management, mindfulness, or cognitive–behavioral strategies may help reduce fear of recurrence and reinforce motivation for healthy behaviors [52,54]. Regular, personalized risk communication and goal-setting sessions can further empower survivors to feel actively engaged in their own long-term prevention plan. Addressing both the biological and psychosocial dimensions of recurrence risk is therefore vital to empowering BCSs to sustain health-promoting behaviors, enhance their quality of life, and potentially reduce the likelihood of recurrence.
Self-motivation and empowerment are central to the adoption of healthy behaviors among BCSs. Despite physical and psychological challenges, many survivors find motivation, often driven by the fear of recurrence. However, motivation is complex, shaped by social support, emotional resilience, and personal agency [55]. Intrinsic motivation, particularly the desire to regain control over one’s health, is crucial for maintaining an improved diet and physical activity [56]. Empowerment reinforces this drive, with BCSs showing a more significant commitment to health-promoting behaviors when they believe their choices can influence recovery. The diagnostic moment, a turning point in their journey, increases health awareness and encourages proactive self-care [54]. Recent studies underscore the importance of emotional resilience and self-compassion in maintaining motivation, significantly when family responsibilities and fear of recurrence complicate adherence [54].
Having strong social relationships is crucial to promoting survival and adhering to healthy behaviors. Support networks reduce psychological distress and enhance quality of life, with peer support—especially from those with similar experiences—building resilience and hope [57]. Support groups provide essential spaces for emotional exchange and practical advice during and after treatment, which can significantly improve physical and mental well-being. Inadequate social support, however, can undermine self-care and adherence to health-promoting behaviors, which necessitates targeted interventions to strengthen these networks [58]. Even so, the difficulty of accessing these resources is still a significant obstacle, especially for those in rural or underserved areas [59]. Future research should focus on scalable interventions, such as digital platforms, to support survivors, especially in regions with limited access to in-person services [60].
Access to healthy food and physical activity resources plays a crucial role in the well-being of BCSs, influencing their ability to maintain a healthy lifestyle and mitigate long-term treatment effects. Women with higher socioeconomic status have been found to experience a lower risk of BC recurrence, fewer subsequent events, and a more favorable prognosis following recurrence over a 10-year period compared to those with lower socioeconomic status [61,62]. This association may be attributed to various factors, including BC risk, adherence to adjuvant treatments, and the management of recurrence, all of which may be influenced by socioeconomic factors [62,63].
Access to affordable, nutritious food—such as fruits and vegetables—is often limited in low-income or rural areas, where the cost of healthy food is a well-documented barrier to adequate consumption [64]. Similarly, the cost and accessibility of physical activity facilities, including gyms or recreational centers, can be a barrier to exercise [65]. In this context, knowledge about how to engage in appropriate physical activity at home becomes essential. However, studies indicate that many survivors lack guidance on how to safely and effectively adapt physical activity routines to the home setting. There is often insufficient information available to BCSs about exercises tailored to their specific needs, particularly in the absence of professional supervision [66]. As previously discussed, cultural and socioeconomic factors substantially influence lifestyle behaviors. These barriers should be addressed through tailored educational interventions, improved access to affordable resources, and the implementation of community-based programs that promote healthy eating and physical activity. Such strategies are crucial to improving the long-term health outcomes of BC survivors [67].
BCSs also face significant barriers to adopting health-promoting behaviors due to a lack of information and training on healthy habits, such as diet and exercise. Some authors note that many survivors are uncertain about beneficial lifestyle changes after treatment, which leads to confusion and frustration [68]. Personalized interventions are essential to bridge these gaps, ensuring survivors are motivated and equipped to engage in healthy activities [69]. Proactive support strategies, including health promotion programs and dietitians’ and fitness trainers’ guidance, can improve physical and emotional well-being [49]. Organizational skills and family involvement are also crucial for maintaining a healthy lifestyle. By scheduling self-care and seeking support from loved ones, survivors can better balance health maintenance with family and work responsibilities [42]. These findings emphasize the importance of planning, coordination, and personalized approaches to achieving and sustaining a health-oriented lifestyle [42,49].
The complexity of BC, including its biological subtypes, stages, and extent, deeply affects treatment options and their duration. Even patients with the same cancer type may respond differently to treatments, leading to varying survival outcomes and psychological well-being. Surgical choices—from partial breast conservation to bilateral mastectomy—impact postoperative recovery and follow-up care. Additionally, the use of radiotherapy and the type of medical treatments, such as hormonal, chemotherapy, or targeted therapies, influence patients’ follow-up experiences. These factors affect not only recurrence rates but also patients’ anxiety levels and the frequency of follow-up visits. Such clinical variations highlight the need for personalized care approaches to support survivors’ adherence to healthy behaviors and overall well-being.
4.1. Strengths and Weaknesses of the Study
This study’s main strength is its thematic synthesis of qualitative research, which gives a comprehensive understanding of the challenges and facilitators that influence the adoption of health behavior among BCSs. The research captures various perspectives and insights by synthesizing multiple studies. The inclusion of direct patient quotes further enhances the validity and relatability of the findings, providing an authentic representation of BCSs experiences, as noted by Onwuegbuzie and Leech [70]. However, some limitations should be considered. Self-reported data may introduce recall bias, leading to overestimating or underestimating adherence to health-promoting behaviors. Moreover, the review includes a limited number of studies from each country, often with small or localized samples, which may not fully capture the diverse cultural perspectives on BC, health promotion, and healthy lifestyles. Therefore, the findings should be interpreted with caution regarding their generalizability across different populations and cultural contexts. Cultural and socioeconomic factors also play a significant role in shaping survivors’ behaviors and may affect the generalizability of the results across diverse populations.
Moreover, some cultural and socioeconomic contexts play a critical role in shaping BCSs’ health behaviors, including the normativity and feasibility of physical activity, especially among women balancing family responsibilities. For instance, in some countries or less resourced areas, exercise may not be a culturally accepted or practical option for women with caregiving duties. Many included studies lacked detailed descriptions of participants’ cultural backgrounds or geographic contexts, limiting the representativeness of the findings. Therefore, caution is warranted when generalizing results, as these factors may significantly influence survivors’ ability and motivation to engage in health-promoting behaviors. Financial constraints, limited social support, and healthcare disparities may vary significantly depending on demographic characteristics, limiting the findings’ broader applicability [59]. Future quantitative research is needed to address these gaps and assess the prevalence and significance of the identified themes across different populations [42].
4.2. Clinical and Public Health Implications
This study’s findings have significant implications for clinical practice and public health. Healthcare providers should prioritize individualized counseling that addresses specific barriers and motivations for each survivor. As supported by Kim et al. (2020), tailoring interventions to the unique needs of everyone can significantly enhance adherence to health-promoting behaviors [42]. Programs incorporating peer support, such as group exercise or community-based dietary workshops, can help build resilience and foster a sense of community, which has been shown to improve adherence and overall well-being. Educational interventions are also crucial in dispelling myths and providing accurate information, empowering survivors to make informed decisions about their health [49]. Furthermore, fatigue management strategies, including customized exercise programs with adjustable intensity, should be incorporated into survivorship care plans to help manage BCSs’ physical challenges and improve recovery [43]. These findings suggest that a more holistic approach, addressing emotional and physical needs, is essential for improving health outcomes in BCS.
In addition to individualized counseling and health-promoting interventions, our findings emphasize the critical need for a comprehensive follow-up care approach that goes beyond periodic imaging and symptom education. Integrating routine psychosocial support, ongoing lifestyle guidance, and proactive monitoring for signs of recurrence can enhance early detection and empower BCSs to maintain healthy behaviors consistently. Such a holistic follow-up framework should involve multidisciplinary teams, including oncologists, surgeons, dietitians, and mental health professionals, to address the complex and evolving needs of survivors after primary treatment completion.
5. Conclusions
This study highlights the multifaceted nature of health behavior adoption among BCSs, identifying obstacles and potential solutions. While numerous barriers exist, leveraging self-motivation, structured programs, and social support can significantly enhance adherence to health-promoting behaviors. By addressing individual needs and incorporating tailored interventions, healthcare providers and policymakers can play a pivotal role in improving survivorship outcomes and reducing the risk of recurrence among BCS. There is an urgent need to implement comprehensive preventive strategies that target both the primary onset of cancer and the risk of disease recurrence, reflecting a critical public health priority.
Future research should focus on developing and testing intervention models tailored to the unique needs of BCSs. Longitudinal studies are needed to evaluate support strategies’ long-term adherence and effectiveness. Additionally, exploring the impact of digital health tools, such as mobile applications for activity tracking and virtual support groups, could offer innovative solutions to improve lifestyle adherence among survivors. Understanding the intersectionality of factors such as socioeconomic status, cultural beliefs, and access to healthcare can further refine interventions to ensure their inclusivity and efficacy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization Breast Cancer 2024 Available online: https://www.who.int/news-room/fact-sheets/detail/breast-cancer(accessed on 5 January 2025)
- 2Afkar A. Jalilian H. Pourreza A. Mir H. Sigaroudi A.E. Heydari S. Cost analysis of breast cancer: A comparison between private and public hospitals in Iran BMC Health Serv. Res.20212121910.1186/s 12913-021-06136-633706762 PMC 7953682 · doi ↗ · pubmed ↗
- 3Bao T. Seidman A. Li Q. Seluzicki C. Blinder V. Meghani S.H. Farrar J.T. Mao J.J. Living with chronic pain: Perceptions of breast cancer survivors Breast Cancer Res. Treat.201816913314010.1007/s 10549-018-4670-929350307 PMC 6147242 · doi ↗ · pubmed ↗
- 4Elder E.E. Kennedy C.W. Gluch L. Carmalt H.L. Janu N.C. Joseph M.G. Donellan M.J. Molland J.G. Gillett D.J. Patterns of breast cancer relapse Eur. J. Surg. Oncol.20063292292710.1016/j.ejso.2006.06.00116822644 · doi ↗ · pubmed ↗
- 5Moloney N.A. Pocovi N.C. Dylke E.S. Graham P.L. De Groef A. Psychological factors are associated with pain at all time frames after breast cancer surgery: A systematic review with meta-analyses Pain Med.20212291594710.1093/pm/pnaa 36333547465 · doi ↗ · pubmed ↗
- 6Liamputtong P. Suwankhong D. Living with breast cancer: The experiences and meaning-making among women in Southern Thailand Eur. J. Cancer Care 20162537138010.1111/ecc.1232125899775 · doi ↗ · pubmed ↗
- 7National Cancer Institute Division of Cancer Control & Population Sciences 2025 Available online: https://cancercontrol.cancer.gov/ocs/definitions(accessed on 6 June 2025)
- 8Morgan E. O’Neill C. Shah R. Langselius O. Su Y. Frick C. Fink H. Bardot A. Walsh P.M. Woods R.R. Metastatic recurrence in women diagnosed with non-metastatic breast cancer: A systematic review and meta-analysis Breast Cancer Res.20242617110.1186/s 13058-024-01881-y 39605105 PMC 11603627 · doi ↗ · pubmed ↗