‘As You Set Out for Ithaca’: VIEW- A Visual Tool for Teaching Ethical Decision Making in Medical Practice
Dikla Agur Cohen, Liv Shadmi, Aya Biderman, Gila Yakov

TL;DR
VIEW is a visual tool designed to help medical professionals better navigate ethical dilemmas by integrating emotional reflection and value-based reasoning.
Contribution
VIEW introduces a novel visual framework for teaching ethical decision making that emphasizes emotional and value-based reflection.
Findings
Participants created visual maps that captured emotional responses and core values during ethical dilemmas.
The tool was found to externalize thought processes and promote value-based reasoning among users.
Users reported improved capacity to handle complex ethical dilemmas and greater engagement with their professional identity.
Abstract
Ethical dilemmas in healthcare often involve navigating emotional and value-laden challenges. Traditional teaching approaches, such as principle-based frameworks, highlight the theory but do not contain tools to integrate emotional reflection and value prioritization, leaving a gap in preparing physicians for real-world ethical decision making. We introduce a novel visual tool named VIEW (Visual Insight for Ethical Wisdom) that enhances ethical decision making by fostering reflection on values, emotions, and professional identity. The VIEW tool was developed as an interactive framework that allows users to map ethical dilemmas visually. It was implemented in three workshops with 31 participants, including junior and senior physicians and medical educators. Participants used the VIEW to analyze real-life ethical challenges. They created 31 visual maps that captured emotional responses,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
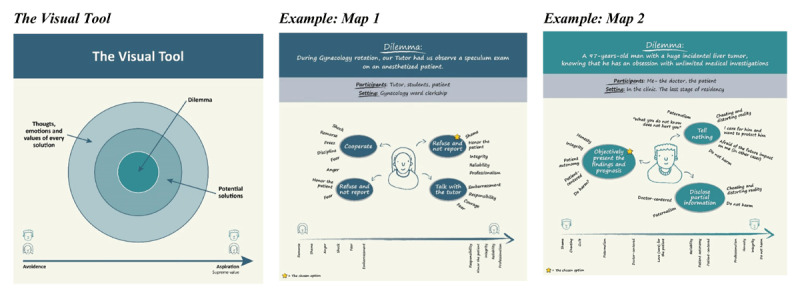 Figure 1
Figure 1|
| |||||
|---|---|---|---|---|---|
| DILEMMA | PARTICIPANTS | SETTING | POTENTIAL SOLUTIONS | THOUGHTS AND EMOTIONS | VALUES |
|
| |||||
| Presenting a 97-year-old man with a huge incidental liver tumor, knowing that he has an obsession with unlimited medical investigations ( | Me- the doctor, | Last stage of residency | Not to tell | Cheating and distorting reality. I care for him and want to protect him. ‘ | Paternalism, integrity, moral degradation Do not harm |
|
| |||||
| During gynecology rotation, our tutor had us observe a speculum exam on an anesthetized patient ( | Tutor, students, patient. | Gynecology clerkship | Collaboration | Regret, shame, shock, helplessness, anger, responsibility, fear, embarrassment. Respect the patient. | Helplessness, remorse for reliability and professional integrity. Values at the center: reliability, professionalism, integrity |
|
| |||||
| Discussing the euthanasia of a hospice patient with the patient and his family | Me- the doctor | At his home, near his bed. Three days after treatment ended | Give optimal palliative care, including sedation; | The ‘right’ legal action; | Integrity |
|
| |||||
| A dialysis patient is not cooperating and insults the staff, who feel threatened. | Patient, dialysis institute staff, | Dialysis institute, during COVID-19 | Support and back up the team and continue care. | The staff is entitled to respect and security. | Patient-centered Teamwork Respect |
|
| |||||
| Gynecological surgery, a woman in a lithotomy position. A janitor inappropriately touches the patient. I reported the incident to my supervisor, who warned me about the potential repercussions. | The patient, | Fifth-year student. Potential for residency in this ward. | Tell the patient. | Fear | Responsibility, |
|
| |||||
|
| |
|---|---|
| THEME |
|
|
| |
| Tool’s effectivity | |
|
| |
|
| |
|
| |
|
| |
|
| |
| Reflective thoughts on personal growth and professional identity | |
|
| |
|
| |
|
| |
|
| |
|
| |
|
| |
|
| |
|
| |
| Avoidance | |
|
| |
|
| |
| Emotions |
|
|
| |
|
| |
|
| |
|
| |
|
| |
|
| |
|
| |
|
| |
| Values | |
|
| |
|
| |
|
| |
|
| |
|
| |
| Integrity | |
|
| |
|
| |
| Patient’s autonomy | |
|
| |
|
| |
| Avoiding harm | |
|
| |
|
| |
|
| |
|
| |
| Doing good | |
|
| |
|
| |
|
| |
|
| |
|
| |
| Teamwork |
|
|
| |
|
| |
|
| |
|
| |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInnovations in Medical Education · Empathy and Medical Education · Clinical Reasoning and Diagnostic Skills
Background & Need for Innovation
‘As you set out for Ithaka,hope your road is a long one,full of adventure, full of discovery…’
C.P. Cavafy’s words [1] echo the journey of healthcare professionals who navigate the challenging landscape of medical ethics—wisdom, reflection, and growth. Medical ethics is central to shaping professional identity (PI) in healthcare. It integrates values, behaviors, and responsibilities [2], while reinforcing key principles such as patient-centered care, autonomy, and social justice into medical professional conduct [3]. Ethical education fosters reflection, empathy, and integrity. It helps professionals align personal and institutional values amidst clinical challenges. This process supports professionalism, fostering trust and collaboration [45]. According to Cruess et al., PI formation involves internalizing the values and norms of the medical profession, transforming individuals into healthcare professionals through reflective practices and ethical reasoning. This connection between reflective practice and PI formation is well-established in the literature [67]. Modern medical ethics have evolved from Percival’s work in 1803 through the post-World War II Nuremberg Code, culminating in today’s comprehensive ethical frameworks. These frameworks include the widely adopted four principles approach of autonomy, beneficence, nonmaleficence, and justice as well as MacIntyre’s revival of Aristotelian virtue ethics, which emphasizes virtues over rigid principles [8910].
Despite this solid theoretical foundation, teaching ethical decision making remains challenging. Recent literature emphasizes context-specific approaches such as Kaldjian’s phronesis framework, which prioritizes contextual understanding and virtues [11]. Various teaching methods—case-based learning, small group discussions, workshops, reflective writing, and patient perspectives—are employed to develop practical wisdom and critical thinking skills [12].
The four topics approach offers a structured framework for analyzing ethical dilemmas in healthcare by focusing on medical indications, patient preferences, quality of life, and contextual features [13]. While this structured approach helps practitioners and trainees consider ethical dilemmas in a systematic manner, it may oversimplify complex issues and struggles to address emotional aspects or support rapid decision making in time-sensitive situations.
Current methods emphasize principle-based ethics, focusing less on the importance of virtues and personal values, which are crucial for holistic reasoning. A one-size-fits-all approach fails, however, to address variability in learner experiences and cultural contexts [14]. Furthermore, the increasing reliance on technology in medical practice creates gaps in training tools that emphasize human-centered, reflective processes [15]. The theoretical framework for the proposed visual tool is inspired by Visual Thinking Strategies (VTS), which integrate visual perception and analytical thinking to enhance clinical skills. The tool, which adopts VTS principles—structured observation, reflective analysis, and collaborative dialogue—aims to cultivate an “ethical eye” enabling healthcare professionals to navigate moral dilemmas with both analytical rigor and emotional awareness [16].
To address the need for a structured approach to ethical decision-making, we developed the VIEW (Visual Insight for Ethical Wisdom) tool, a novel visual tool designed to enhance ethical decision making through reflective practices.
Goal of Innovation
The VIEW tool integrates virtue-based and principle-based ethics by fostering reflective practices through visual mapping. Its name highlights its function of providing a clearer “view” of ethical dilemmas. By incorporating emotions, narratives, and structured ethical frameworks, VIEW offers an interactive and introspective approach for both educational and clinical contexts.
Steps Taken for Development and Implementation
The VIEW tool was initially designed for a workshop by two early career physicians in a leadership program. Its effectiveness led to its use in two subsequent workshops.
Implementation Steps
The VIEW tool employs a three-step process to guide users through ethical dilemmas: structured observation, emotional reflection, and narrative integration.
The workshops followed a structured sequence using the visual tool (Figure 1), as follows:
Graphic Mapping: Using four concentric layers, participants created a map, i.e., a visual representation of an ethical dilemma. The outer layer documented a specific ethical dilemma from their professional practice, while the central layer contained the core moral question. The two layers in between mapped potential resolution pathways, with participants identifying each solution’s emotional responses and underlying values. This method helped participants systematically assess how different solutions align with their emotions and values.Instinctual Choices and Value Exploration: Participants identified their instinctual choices among the potential solutions, and explored the underlying emotions and values driving the different options.Values Ranking: Participants ranked values from avoidance to aspiration, fostering a multi-dimensional perspective of their relationship with each value and encouraging non-linear exploration of ethical decision making.
The Visual Tool.
Group Discussion and Reflection: Participants shared their maps and reflections in a group setting, discussing their decisions’ emotional and long-term implications.
Workshops
To evaluate the tool, data were collected from three workshops:
May 2021: Ten junior family physicians (FPs).February 2022: Fifteen family medicine educators.July 2022: Six senior medical educators involved in ethical committees.
The Supplementary Table presents the demographic data of the workshop participants. Most participants had minimal exposure prior to ethics training, primarily limited to traditional case-based discussions during residency.
Data Collection and Analysis
Data from the workshops were analyzed through an iterative process involving observations, visual maps, and semi-structured interviews. Two independent researchers manually coded and analyzed all data, refining themes through discussion. This rigorous qualitative approach ensured comprehensive interpretation of the participants’ experiences and insights.
Observations: We took detailed field notes during the workshops, with observations focusing on participants’ interactions with the tool, group dynamics, and the nature of discussions. Verbal and non-verbal behaviors were documented, including collaborative problem-solving processes. These notes were coded, focusing on behaviors and discussions, capturing the reflections and evolving interpretations [17].
Visual Maps: In total, 31 visual maps were generated by workshop participants during the sessions. Each map represents a participant’s articulation of an ethical dilemma, prioritized values, and emotional responses. The analysis process involved identifying recurring patterns and cross-referencing these patterns with the observations and interview data to ensure triangulation and comprehensive understanding of the themes.
Interviews: We conducted four semi-structured interviews with workshop participants from diverse backgrounds within two weeks of the workshops to capture immediate reflections. Transcriptions were manually coded to identify recurring themes and patterns. The number of interviews was intentionally limited so as to complement insights from the observations and visual maps rather than to achieve theoretical saturation [18].
Outcomes of the Innovation
We evaluated the VIEW tool’s effectiveness as a teaching method for enhancing ethical decision making among healthcare professionals. Workshop participants had diverse backgrounds and professional experience, and included early career and senior FPs, educators, and ethics committee members (See Supplementary Table).
The analysis of 31 maps demonstrated that the tool effectively addressed diverse ethical challenges. They ranged from complex end-of-life care decisions to everyday, yet ethically significant situations, such as sick leave certification.
Participants explored ethical dilemmas through personal real-life clinical examples. These personal scenarios sparked discussion and mapping exercises, fostering a deeper understanding of ethical reasoning processes. The analysis identified three primary themes: interpretation of dilemmas, emotional responses, and values in ethical decision making (See Table 1). For example, participants navigated conflicts between patient autonomy and professional integrity, balanced emotional distress with legal and ethical obligations, and reflected on their evolving PI.
Case Example: A medical student recounts a gynecology clerkship incident two years ago. During a gynecology rotation, students were instructed to observe a speculum exam on an anesthetized patient, leading to a significant ethical dilemma (see Figure 1).
Interpretation: The student faced conflicting values, particularly the tension between respecting the patient’s dignity and complying with the tutor’s instructions. Core values such as patient autonomy, consent, and professional integrity were at stake, as the student questioned the ethical propriety of observing the procedure without the patient’s explicit consent.
Values: The student faced varying values, with patient dignity and autonomy at the aspiration end, emphasizing respect for consent and ethical responsibility. In contrast, authority acceptance and obedience are at the avoidance end, representing discomfort in following the tutor’s instructions. Values like professional integrity and clinical learning balanced the need for experience with ethical practice.
Emotions such as regret, shame, and fear surfaced as the student navigated the situation, highlighting the inner conflict and the depth of reflection required when balancing these intersecting values.
Table 2 presents the themes and quotes.
For example, a reflection on the case presented in Map 1, Figure 1:
I felt shocked and ashamed; it didn’t seem right to perform such an exam without the patient’s consent.
This case exemplifies the complex ethical landscape that medical trainees navigate. Conflicting interpretations and emotional distress were also observed in other cases (See Table 1), emphasizing the need for a decision-making framework that integrates thoughts, emotions, and values for practical ethical reasoning in medical education.
Interpretation of Dilemmas
Participants’ reflections revealed the challenges of balancing competing values and legal obligations, often exposing tensions between patient-centered care and professional integrity. For instance, one participant struggled with the ethical complexity of providing life-ending care to a hospice patient. Her reflections highlighted the emotional weight of the decision and its broader implications for the patient’s dignity and relationships:
Did he [the patient] have time to say goodbye?
This same participant also wrestled with the fear of violating the principle of nonmaleficence, expressing concern about the irreversible consequences of his actions:
Do not cause death to a conscious person.
Another participant, who had to deal with a non-cooperative dialysis patient, found it challenging to prioritize team well-being and security over patient dignity, especially in what was a high-stress environment:
The staff is entitled to respect and security. Who has priority?
In a different scenario, where inappropriate behavior by a colleague was observed, a participant expressed fear and doubt:
What does that say about me? I bypassed my superiors… I will not be able to specialize in the ward
Following their interpretation, participants’ real-time reactions to the dilemmas ranged from avoidance to confrontation, where avoidance often reflects the desire to escape emotional challenges:
Let it go… Don’t think about it.
Others, however, perceived avoidance in a positive light, as constructive collaboration:
I will approach my supervisor and ask her to confront the conflict.
Emotional Responses
The emotional landscape revealed through the VIEW tool was rich and complex, with participants expressing a broad spectrum of emotions, including helplessness, anger, fear, regret, shame, and empathy, all closely linked to the ethical dilemmas they faced.
For instance:
Reflecting on the workshop, I realized my decisions were often fear-driven, overlooking potential benefits. I was angry with the patient’s family; why did they put me in this situation?
The VIEW tool assisted participants in processing and identifying their emotional responses, allowing them to confront these feelings both intellectually and emotionally.
Values in Ethical Decision Making
Participants articulated various values that guided their ethical decision making. Senior professionals struggled to rank emotional and value-based components, while less experienced participants found the process more intuitive.
As one senior participant noted:
When unsure, I consult with a colleague and avoid involving feelings.
In contrast, a younger participant reflected:
Values evolve; flexibility is necessary. Life isn’t black and white.
Values expressed during the workshops often aligned with the four principles of medical ethics, in addition to integrity and teamwork. For example:
Collision of values: ‘The patient’s benefit often takes precedence over absolute values like integrity.’Patient autonomy: ‘The patient’s dignity and right to his life.’Avoiding harm: ‘I will not expedite the death of a person.’Doing good: ‘What is in the patient’s best interest.’Integrity: ‘Acting against my beliefs and values may lead to moral deterioration.’Teamwork: ‘I am afraid of my colleague’s hostility…’
The diversity in values enriched the learning experience and highlighted the importance of tools that accommodate varied ethical perspectives.
These insights were pivotal for fostering ethical reasoning, self-awareness, and reflective thoughts concerning PI, as expressed by the following quotes:
I realized there’s no absolute truth; everything is a matter of perspective.…the workshop’s pivotal role in fostering ethical reflection and self-awareness, which are crucial for making sound moral decisions.I felt I had processed the case more effectively and could draw significant insights from the challenging experience for the future.
Participants actively engaged with the tool, emphasizing personal values and offering a nuanced understanding of the complex interplay between individual and contextual factors in ethical decision making.
Critical Reflection on the Process
Unlike increasingly AI-driven decision-support tools, our visual tool, the VIEW, offers a personalized and intuitive platform, providing a novel framework for ethical analysis by linking emotions, narratives, and structured decision-making. Its focus on integrating these dimensions encourages a holistic approach to navigating moral dilemmas, ensuring its relevance in both educational and clinical settings.
Our findings highlight differences in ethical reasoning based on professional experience. Senior physicians rely more on protocols and experience, while younger physicians often react emotionally. This emphasizes the need for tailored ethics education that integrates reflection to cultivate practical wisdom.
The VIEW complements established ethical frameworks such as the four principles model [8] and the four topics model [13], by incorporating integrity and teamwork, emphasizing their importance in collaborative, patient-centered care. It emphasizes the emotional and value-based responses of ethical analysis, allowing participants to reconcile instinctual virtue-based responses with principle-based reasoning. This fosters a more integrative and nuanced approach to ethical dilemmas.
The VIEW tool promotes a reflective practice by integrating ethical frameworks. It helps healthcare professionals strengthen their moral compass, self-awareness, and professional identity, engaging them more effectively than traditional methods like case discussions and lectures [1920].
The tool effectively explores emotional and value-based dimensions of ethical dilemmas through personal examples, but it lacks real-time clinical scenarios. While this foundational approach aids in ethical reasoning, future research is needed to evaluate its applicability in dynamic real-world contexts as well as its long-term impact on medical practice compared with traditional ethics teaching methods. Nonetheless, participants reported improved clarity and resolution in their ethical decision making, suggesting the VIEW has the potential to enhance reflective practices and strengthen ethical reasoning in medical education.
This study has limitations, including a small sample size and the potential influence of cultural context, which may affect the generalizability of our findings. The qualitative approach introduces subjectivity, and the tool’s effectiveness across different specialties and experience levels remains unexplored. Further research in diverse settings is necessary to validate and refine the tool.
Summary
The VIEW tool is an effective teaching method for fostering comprehensive reflective perspectives and deepening self-awareness. Its simple intuitive design helps align ethical analysis with personal values, supporting the development of a nuanced ethical framework and professional identity. Further research is recommended to validate VIEW applicability across diverse professional disciplines.
Additional File
The additional file for this article can be found as follows:
10.5334/pme.1543.s1Supplement Table.Participants’ demographics.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Foundation P. Ithaka by C. P. Cavafy [Internet]. Poetry Foundation. Poetry Foundation; 2024 [cited 2024 Jun 15]. Available from: https://www.poetryfoundation.org/poems/51296/ithaka-56d 22eef 917ec
- 2Cruess RL, Cruess SR, Boudreau JD, Snell L, Steinert Y. Reframing medical education to support professional identity formation. Acad Med. 2014;89(11):1446–51. DOI: 10.1097/ACM.000000000000042725054423 · doi ↗ · pubmed ↗
- 3Shahabi M, Mohammadi N, Koohpayehzadeh J, Soltani Arabshahi SK. The attainment of physician’s professional identity through meaningful practice: A qualitative study. Med J Islam Repub Iran [Internet]. 2020 Mar 5 [cited 2024 Dec 24];34:16. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 7293806/.32551305 10.34171/mjiri.34.16PMC 7293806 · doi ↗ · pubmed ↗
- 4Chandran L, Iuli RJ, Strano-Paul L, Post SG. Developing “a Way of Being”: Deliberate Approaches to Professional Identity Formation in Medical Education. Acad Psychiatry [Internet]. 2019 Oct 1 [cited 2024 Dec 24];43(5):521–7. DOI: 10.1007/s 40596-019-01048-430993596 · doi ↗ · pubmed ↗
- 5Touati N, Rodriguez C, Paquette MA, Maillet L, Denis JL. Professional Role Identity: At the Heart of Medical Collaboration Across Organisational Boundaries. Int J Integr Care [Internet]. 2019 Apr 2 [cited 2024 Dec 24];19(2). Available from: https://ijic.org/articles/10.5334/ijic.4184.10.5334/ijic.4184 PMC 645024430971867 · doi ↗ · pubmed ↗
- 6Sarraf-Yazdi S, Goh S, Krishna L. Conceptualizing Professional Identity Formation in Medicine. Acad Med J Assoc Am Med Coll. 2024 Mar 1;99(3):343. DOI: 10.1097/ACM.000000000000555938015999 · doi ↗ · pubmed ↗
- 7Cruess RL, Cruess SR, Boudreau JD, Snell L, Steinert Y. Reframing medical education to support professional identity formation. Acad Med. 2014;89(11):1446–51. DOI: 10.1097/ACM.000000000000042725054423 · doi ↗ · pubmed ↗
- 8Gillon R. Medical ethics: four principles plus attention to scope. BMJ [Internet]. 1994 Jul 16 [cited 2021 Nov 10];309(6948):184. Available from: https://www.bmj.com/content/309/6948/184.8044100 10.1136/bmj.309.6948.184PMC 2540719 · doi ↗ · pubmed ↗