Clinical Outcomes of Escherichia coli Acute Bacterial Prostatitis: A Comparative Study of Oral Sequential Therapy with β-Lactam Versus Quinolone Antibiotics
Laura Gisbert, Beatriz Dietl, Mariona Xercavins, Aina Mateu, María López, Ana Martínez-Urrea, Lucía Boix-Palop, Esther Calbo

TL;DR
This study compares cefuroxime and ciprofloxacin for treating Escherichia coli-induced acute bacterial prostatitis, finding ciprofloxacin more effective in preventing recurrence.
Contribution
The study provides new evidence on antibiotic efficacy for Escherichia coli-induced acute bacterial prostatitis, highlighting ciprofloxacin's superiority over cefuroxime.
Findings
Ciprofloxacin showed higher clinical cure rates compared to cefuroxime in treating Escherichia coli-induced prostatitis.
Ciprofloxacin reduced the risk of recurrence, while prior UTI increased clinical failure risk.
Clinical failure was significantly associated with cefuroxime treatment and prior urinary tract infections.
Abstract
Background/Objectives: Optimal management of acute bacterial prostatitis (ABP) remains uncertain, but the use of antibiotics with good prostatic tissue penetration is critical to prevent recurrence and chronic progression. This study aimed to describe clinical characteristics and outcomes of ABP due to Escherichia coli (ABP-E.coli), compare effectiveness of sequential high-dose cefuroxime (ABP-CXM) versus ciprofloxacin (ABP-CIP), and identify risk factors for clinical failure. Methods: We conducted a retrospective study including men >18 years diagnosed with ABP-E. coli between January 2010 and November 2023 at a 400-bed hospital. Patients received oral cefuroxime (500 mg/8 h) or oral ciprofloxacin (500 mg/12 h). Outcomes over 90 days included clinical cure, recurrence and reinfection. Definitions: Clinical cure—resolution of symptoms without recurrences; recurrence—new ABP episode with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
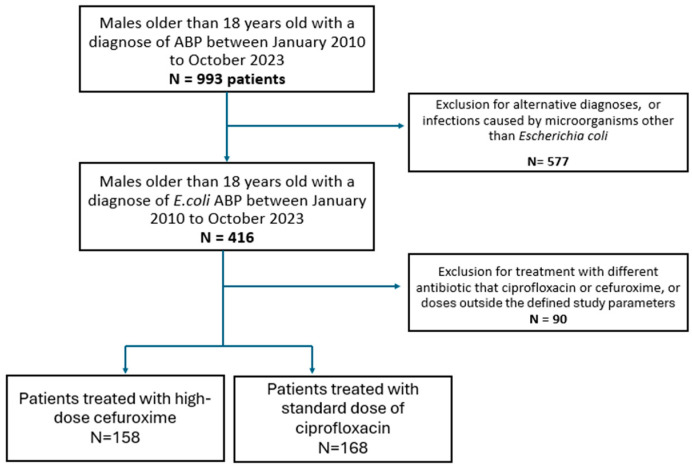 Figure 1
Figure 1- —‘Instituto de Salud Carlos III, Fondo de investigación sanitaria’ (FIS)
- —European Society of Clinical Microbiology and Infectious Diseases (ESCMID)
- —‘Fundació per la Docència i Recerca de MútuaTerrassa’
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrinary Tract Infections Management · Urinary Bladder and Prostate Research · Prostate Cancer Diagnosis and Treatment
1. Introduction
Acute bacterial prostatitis (ABP) is a common cause of emergency room visits, with an incidence of 2 to 5% in adult males [1], and contributes significantly to antibiotic use [2]. Although rarely life-threatening—except in cases of sepsis [3]—inadequate management increases the risk of chronic prostatitis and recurrent infections [1], negatively impacting quality of life. Recognized as a distinct category of prostatitis by the NIH in 1999 [4], the diagnosis of ABP remains inconsistent, and treatment approaches are heterogenous [5].
Several factors influence the risk of recurrence, abscess formation, or progression to chronic prostatitis [1,6], with adequate antibiotic penetration into prostatic tissue being a critical determinant [7,8]. Fluroquinolones remain the first-line treatment according to current clinical guidelines [9,10] and expert reviews [4,11,12]; however, their use is increasingly limited by rising resistance among Enterobacterales.
According to ECDC surveillance reports, fluoroquinolone resistance in invasive E. coli isolates in Spain remained consistently high between 2010 and 2023, ranging from 23% to 32%. Although cefuroxime is not specifically reported, resistance to third-generation cephalosporins in E. coli—often used as a proxy—ranged from 12.1% to 16.8% during the same period [13]. In clinical practice, ABP often allows early transition to oral therapy, with beta-lactam agents such as cefuroxime frequently prescribed at discharge due to the high prevalence of fluoroquinolone resistance.
We conducted a retrospective study to evaluate whether cefuroxime—the most frequently prescribed oral empirical antibiotic for ABP in our setting—is comparable in effectiveness to guidelines-recommended treatments. The study focused on ABP caused by E. coli, the most common urinary pathogen.
Our objective was to compare the clinical characteristics, diagnosis, and outcomes of ABP-E. coli, treated with high-dose cefuroxime (ABP-CXM) versus ciprofloxacin (ABP-CIP) in men over 18 years of age, and to identify prognostic factors associated with clinical failure.
2. Results
We included 326 episodes of E. coli ABP: 158 were treated with cefuroxime and 168 with ciprofloxacin. The eligible individuals’ identification process is shown in Figure 1.
Patients in the ABP-CXM group were younger (63.5 (4–73) vs. 67.5 (58–76); p = 0.005) and had fewer comorbidities (Charlson index: 0 [0–1] vs. 1 [0–2]; p= 0.04; and age adjusted Charlson: 2 (1–4) vs. 3 (1–4); p = 0.009). In terms of urological examination findings, patients in the ABP-CIP group had undergone urological surgical manipulations more frequently in the previous month (2.5% vs. 9.6%; p = 0.008) and had a higher prevalence of benign prostatic hyperplasia (26.1% vs. 39.5%; p = 0.01). However, both prostatic and urologic tract neoplasia rates were not significantly different between the groups. Clinical characteristics and complementary explorations are summarized in Table 1.
Overall, the rate of E. coli resistant to ciprofloxacin in the total cohort (including every ABP-E. coli) was 23.1% (n = 96/416), while resistance to cefuroxime was 16.3% (n = 68/416), being consistent with rates reported in Europe. Data on microbiological results is shown in Table 2.
Clinical cure was achieved in 132 episodes (85.7%) in the ABP-CXM group, in front of 158 (96.9%) in the ABP-CIP group (p < 0.001). Recurrence was higher in the ABP-CXM group (6.96% (n = 11) versus 0 in the ABP-CIP group (p < 0.001)) without differences in reinfection (5 (3.16) vs. 5 (3); p = 0.91). No difference was found in prostatic abscess development (1 (0.63) vs. 1 (0.6); p = 0.93), nor was mortality (1 (0.63) vs. 1 (0.6); p = 16) identified between groups. Data about treatment is summarized in Table 3.
We perform a multivariate analysis of clinical failure to find risk factors, results are in Table 4. Statistical analysis was performed using logistic regression test.
3. Discussion
This retrospective observational study suggests that ciprofloxacin may offer superior clinical outcomes compared to high-dose cefuroxime (CXM) in ABP-E. coli. Our analysis demonstrates that patients treated with CIP achieved higher clinical cure rates and lower recurrence rates than those receiving CXM. Notably, CIP emerged as a protective factor against clinical failure, highlighting its efficacy as targeted therapy for ABP. These results are particularly compelling given that the CIP group exhibited higher baseline disease severity and more recurrence risk factors, suggesting robust performance in challenging cases. These findings support CIP as the preferred treatment for ABP-E. coli, especially in high-risk patients.
Our results are consistent with studies evaluating ABP treatment outcomes. Marquez-Algaba et al. [14] reported relapse rates of 1.8% with CIP versus 3.6% with intravenous beta-lactams (BL), 9.3% with cotrimoxazole (TMP-SMX), and 9.8% with oral BL in their 410-patients ABP retrospective cohort—a pattern that aligns with our observed 7% relapse rate with CXM. In a multivariable analysis, oral BL (OR 5.3, 95% CI 1.2–23.3) and TMP-SMX (OR 4.9, 95% CI 1.1–23.2) were detected as significant relapsed risk factors. Another large retrospective study (n = 33,336 UTI cases) found higher relapse rates with BL (7.3%) and TMP-SMX (5.7%) comparing with FQ (3.9%), with BL emerging as an independent risk factor for relapse (OR 1.81, 95% CI 1.52–2.17) [15]. Madaras-Kelly’s multicenter analysis (n = 73,334) further supported these trends, showing higher clinical failure rates with BL (17.8% in men) versus FQ (12.7%) [16]. Although study designs vary, the collective evidence suggests that oral BL have lower efficacy than fluoroquinolones for male complicated urinary tract infections and acute bacterial prostatitis
Several retrospective studies have assessed oral step-down therapy for Gram-negative bloodstream infections (BSI), though most focus on uncomplicated UTIs or exclude ABP. A 2018 systematic review and meta-analysis of Enterobacterales BSI transitioned to oral therapy (n = 2289) found higher recurrence rates with oral BL despite similar mortality [17]. Suboptimal BL dosing was common and may have contributed to this outcome. Although BSI was uncommon in our study, these data support our findings.
Fluoroquinolones are the preferred treatment for ABP in international guidelines, supported by their high intraprostatic penetration (due to their lipophilic nature small molecular size) and concentration-dependent bactericidal activity [7,8]. Although no randomized trials have been conducted, their efficacy is well documented in retrospective studies and clinical experience. However, the IDSA advises against empirical FQ use when Enterobacterales resistance exceeds 10%, a threshold commonly surpassed in Europe [18].
Our study reflects real-life clinical practice. Notably, up to two-thirds of patients in the ABP-CXM group had an infection caused by CIP-susceptible strain but were still treated with BL. These patients were likely discharged earlier than those in the ABP-CIP group, as suggested by their shorter length of stay, and microbial susceptibility results may not have been available in time to guide oral therapy decisions. Some authors have proposed systematic urine culture reviews after discharge in patients treated empirically for ABP [3,14]. Given the rising rates of fluoroquinolone resistance, targeted strategies—such as rapid FQ resistance testing or electronic alerts to flag eligible patients—are needed to optimize treatment. In parallel, generating robust evidence through prospective studies to support alternative oral treatment options for ABP remains a key priority.
ABP still lacks standardized diagnostic criteria, which limits diagnostic certainty and comparability across studies. In 2023, Soudais et al. reviewed international guidelines and highlighted inconsistencies in ABP definitions [19]. A recent Delphi consensus proposed diagnostic criteria based on symptoms, systemic signs, pyuria, and microbiological findings [20]. Still, a unified international definition is needed. Further complicating this, clinical presentation varies with age and care setting. A 2019 study by Etienne et al. (n = 586) found that older patients (median age 84) had fewer typical symptoms (63% fever, 50% urinary symptoms), and treatment approaches differed across departments despite similar outcomes [5]. In our cohort, 96% of patients had fever at presentation, supporting appropriate case selection.
Serum prostate-specific antigen (sPSA) is a potentially useful marker for ABP diagnosis but remains underexplored. Prospective studies have shown that 81–83% of men with febrile UTI present with elevated sPSA levels that normalize after treatment [21,22]. In a recent study by our group, 89% of episodes in men with febrile UTI had sPSA > 5 ng/mL (median 16.7 ng/mL) [23]. These findings suggest that sPSA may reflect prostate involvement in male UTIs and could help guide treatment decisions.
Several risk factors for poor ABP outcomes have been described. Two large retrospective studies (n = 130 and n = 614) reported higher rates of abscesses and recurrence in patients with prior urological manipulation [24,25]. Another study (n = 437) found progression to chronic prostatitis or pelvic pain syndrome in 11.8% of cases, associated with alcohol use, diabetes, voiding symptoms, prior manipulations, prostate enlargement, catheterization, and shorter antibiotic courses, regardless of antibiotic type [26]. In our cohort, prior manipulation was not associated with higher rates of clinical failure or abscesses. However, these patients were overrepresented in the ABP-CIP group, suggesting that ciprofloxacin may have reduced the risk of complications. In multivariate analysis, ciprofloxacin use was a protective factor against recurrence, while the history of UTI in the previous year was associated with clinical failure. This may reflect underlying chronic prostatitis, which often presents as recurrent lower UTI and may require prolonged treatment [2,11].
Our study has several limitations. First, it was conducted at a single center which may limit the generalizability of the findings. Second, the long study period could have introduced variability in clinical practice. Third, its retrospective design inherently limits data consistency and completeness. Finally, most patients were diagnosed in the emergency department, where variability in physician experience and decision-making may have influenced diagnostic and treatment approaches.
Nonetheless, the study also has notable strengths. It includes a well-characterized cohort with comprehensive clinical data. Patients with catheter-related UTIs were excluded, reducing the likelihood of misclassification. Moreover, by focusing solely on patients treated with either cefuroxime or ciprofloxacin, the analysis allows comparison between these two therapeutic options.
4. Material and Methods
We conducted a retrospective, observational study at a 400-bed teaching hospital in Barcelona, Spain (Hospital Universitari Mutua Terrassa), including all adult patients (>18 years) diagnosed with ABP-E. coli between January 2010 to October 2023. Eligible patients were treated with high-dose cefuroxime (500 mg every 8 h) or standard-dose ciprofloxacin (500 mg every 12 h) and were diagnosed at the Emergency Department or during hospitalization. Patients were followed up to 90 days after the initial episode.
We reviewed all ABP cases in the hospital database and included those presenting with symptoms consistent with ABP and a positive urine culture showing significant growth of E. coli (>100,000 CFU). Data were collected from medical and nursing records, including clinical presentation, physical examinations findings, laboratory and microbiological results, acquisition site, imaging studies, treatment regimens, adverse effects, and clinical outcomes, as well as age and comorbidities present in the year prior to infection.
Informed consent was waived due to the retrospective nature of the study. According to institutional and national regulations, formal ethics committee approval was not required.
Exclusion criteria, variables definitions, and statistical methods are detailed in Appendix A.
5. Conclusions
In conclusion, our findings support ciprofloxacin as the preferred treatment for E. coli-related ABP, particularly in patients at higher recurrence risk. The history of previous UTIs emerged as a significant predictor of clinical failure, underscoring the need for closer follow-up and potentially alternative therapeutic strategies. Notably, many patients infected with ciprofloxacin-susceptible strains were treated with beta-lactams. This highlights the challenge of managing community-acquired infections requiring prolonged therapy, where empirical decisions are often made without susceptibility data. A more personalized approach—considering individual risk factor and rapid diagnostics—is needed. In the context of increasing resistance to quinolones, it is essential to produce prospective studies and explore effective oral alternatives such as fosfomycin.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Davis N.G. Silberman M. Acute bacterial prostatitis Stat Pearls Stat Pearls Treasure Island, FL, USA 202429083799 · pubmed ↗
- 2Krieger J.N. Lee S.W.H. Jeon J. Cheah P.Y. Liong M.L. Riley D.E. Epidemiology of prostatitis Int. J. Antimicrob. Agents 200831859010.1016/j.ijantimicag.2007.08.02818164907 PMC 2292121 · doi ↗ · pubmed ↗
- 3Nagy V. Kubej D. Acute bacterial prostatitis in humans: Current microbiological spectrum, sensitivity to antibiotics and clinical findings Urol. Int.20128944545010.1159/00034265323095643 · doi ↗ · pubmed ↗
- 4Krieger J.N. NIH consensus definition and classification of prostatitis JAMA 199928223623710.1001/jama.282.3.23610422990 · doi ↗ · pubmed ↗
- 5Etienne M. Chavanet P. Sibert L. Michel F. Levesque H. Lorcerie B. Doucet J. Pfitzenmeyer P. Caron F. Acute bacterial prostatitis: Heterogeneity in diagnostic criteria and management. Retrospective multicentric analysis of 371 patients diagnosed with acute prostatitis BMC Infect. Dis.200881210.1186/1471-2334-8-1218234108 PMC 2254416 · doi ↗ · pubmed ↗
- 6Lee D.S. Choe H.S. Kim H.Y. Kim S.W. Bae S.R. Yoon B.I. Lee S.J. Acute bacterial prostatitis and abscess formation BMC Urol.2016163810.1186/s 12894-016-0153-727388006 PMC 4936164 · doi ↗ · pubmed ↗
- 7Lipsky B.A. Byren I. Hoey C.T. Treatment of bacterial prostatitis Clin. Infect. Dis.2010501641165210.1086/65286120459324 · doi ↗ · pubmed ↗
- 8Charalabopoulos K. Karachalios G. Baltogiannis D. Charalabopoulos A. Giannakopoulos X. Sofikitis N. Penetration of antimicrobial agents into the prostate Chemotherapy 20034926927910.1159/00007452614671426 · doi ↗ · pubmed ↗