Multisite Infections Caused by Carbapenem-Resistant Klebsiella Pneumoniae: Unveiling the Clinical Characteristics and Risk Factors
Jing Li, Shunjun Wu, Huanhuan Zhang, Xingxing Guo, Wanting Meng, Heng Zhao, Liqiang Song

TL;DR
This study examines infections caused by drug-resistant Klebsiella bacteria in multiple body sites and identifies risk factors for severe outcomes.
Contribution
The study identifies specific risk factors for multisite CRKP infections and mortality, offering insights for early intervention.
Findings
74.3% of CRKP bloodstream infection patients had multisite infections.
ICU admission and thrombocytopenia were significant risk factors for mortality.
Previous surgery and ICU admission were linked to higher risk of multisite infections.
Abstract
Objectives: There is a scarcity of studies on multisite infections (MSIs) caused by carbapenem-resistant Klebsiella pneumoniae (CRKP). The primary objectives of this research were to determine the clinical characteristics of CRKP MSI, and the risk factors of infection and mortality. Methods: Patients with a CRKP bloodstream infection (BSI) were enrolled retrospectively between January 2017 and December 2021 in Xijing Hospital, China. The risk factors for CRKP MSI and mortality were evaluated. The demographic data, clinical and microbiological characteristics, therapy and outcomes were analyzed. Results: Among 101 patients, 74.3% (75/101) had a diagnosis of CRKP MSI, while 25.7% (26/101) of CRKP non-MSI. The overall case fatality rate was 42.6% (43/101). Multivariate analysis indicated that previous surgery (OR 3.971, 95% CI 1.504–10.480, p = 0.005) and ICU admission (OR 3.322, 95% CI…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
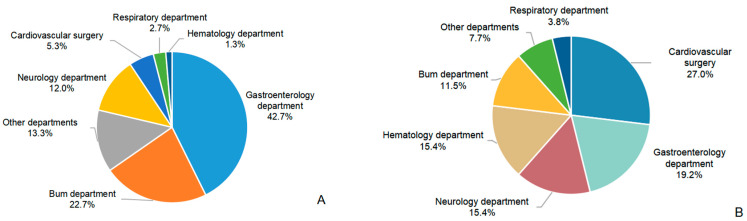 Figure 1
Figure 1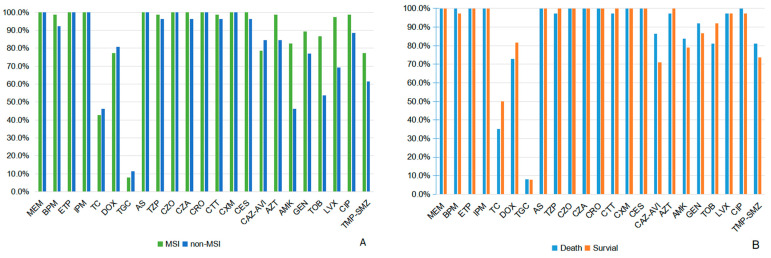 Figure 2
Figure 2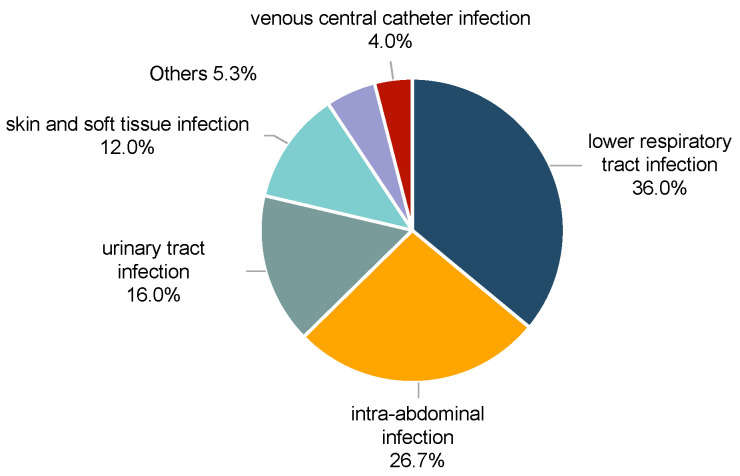 Figure 3
Figure 3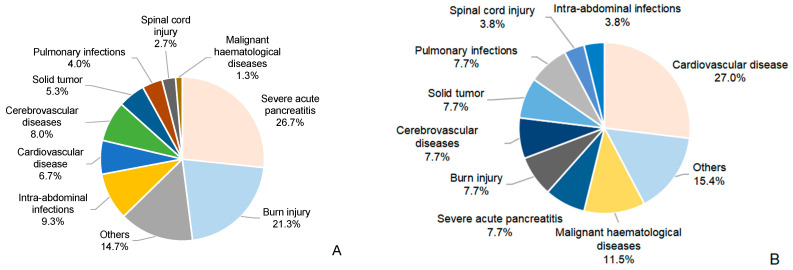 Figure 4
Figure 4- —Discipline Promotion Plan of Xijing Hospital
- —Clinical Research Program of Air Force Military Medical University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntibiotic Resistance in Bacteria · Antibiotic Use and Resistance · Bacterial Identification and Susceptibility Testing
1. Introduction
Over the past decade, carbapenem-resistant Klebsiella pneumoniae (CRKP) has become a major public health concern on a global scale [1]. Given the limited available treatments and high mortality, the World Health Organization categorized CRKP as a critical priority pathogen in 2017 [2]. In China, resistance rates for Klebsiella pneumoniae for carbapenem increased steadily between 2005 and 2020 (from 3.0 to 25.0% in imipenem and from 2.9 to 24.2% in meropenem) [3].
Numerous infections can be caused by CRKP, such as pneumonia, urinary tract infections, skin and soft tissue infections, and bloodstream infection (BSI) [4]. BSI is the most severe form of CRKP infections, with mortality ranging from 38.9% to 71.9% [5,6]. Multisite infections (MSIs) are common in BSI patients. An earlier study claimed that CRKP could be detected in additional samples from 65.9% of CRKP BSI patients [6]. MSIs often complicate the condition due to severe infections and inadequate antimicrobial therapies [7]. Therefore, an improved identification of patients at the highest risk is crucial to formulate effective intervention strategies to improve prognosis [8]. Many studies have focused on the risk factors for CRKP infections, but there are little data on CRKP MSIs.
Our study focused on CRKP BSI, especially in MSI patients. We described the clinical characteristics and antimicrobial susceptibility test results, as well as infection and mortality risk factors associated with CRKP MSIs.
2. Results
2.1. Clinical Characteristics and Antimicrobial Susceptibility
A total of 101 patients with CRKP BSI were included, consisting of 77 male (76.2%) and 24 female (23.8%) patients, with a mean age of 52.73 ± 16.17 years. Seventy-five patients (74.3%) were classified into the MSI group, while the remaining twenty-six (25.7%) comprised the non-MSI group (Table 1). Nearly half of the CRKP MSI cases were from the gastroenterology department (42.7%), followed by the burns department (22.7%). The non-MSI group was mainly from the cardiovascular surgery and gastroenterology department (26.9% and 19.2%, respectively) (Figure 1). Drug resistance of CRKP was observed across a variety of antibiotics in both groups (Figure 2). The MSI group had significantly higher resistance rates to aztreonam (98.7% vs. 84.6%, p = 0.015), amikacin (81.3% vs. 46.2%, p = 0.001), tobramycin (86.7% vs. 53.8%, p < 0.001) and levofloxacin (97.3% vs. 69.2%, p < 0.001) (Supplementary Table S1). Tigecycline maintained the lowest resistance rates among all antibiotics tested (11.5% in MSI vs. 8.0% in non-MSI) (Supplementary Table S1). The lower respiratory tract was the most common source of infection in the MSI group (36.0%) (Figure 3). Severe acute pancreatitis was the most common cause of admission in the MSI group (26.7%) (Figure 4). The mortality rate of the MSI group was 49.3% (37/75), while that of the non-MSI group was 23.1% (6/26), which was statistically significant (p = 0.020).
2.2. Risk Factors for CRKP MSI
Besides blood samples, CRKP could be found in one site in 50.7% (38/75) patients and at least two sites in 49.3% (37/75) patients in the MSI group. Most isolates were collected from the sputum (47/75, 62.6%), followed by peritoneal effusion (28/75, 37.3%) and skin wounds (20/75, 26.7%) (Table 2). Compared with the non-MSI group, the MSI group had a higher proportion of ICU admission (73.3% vs. 46.2%, p = 0.011). The MSI group was more prone to receiving invasive mechanical ventilation (65.3% vs. 38.5%, p = 0.017). For both groups, fever was the most prevalent early clinical sign of BSI. However, chill, disturbance of consciousness, septic shock and inflammatory biomarkers did not differ between the two groups. Furthermore, 44.0% (33/75) patients received appropriate empiric therapy in the MSI group and 26.9% (7/26) in the non-MSI group (p = 0.125); 78.7% (59/75) patients received appropriate definitive therapy in the MSI group and 61.5% (16/26) in the non-MSI group (p = 0.085). Most patients in both groups received appropriate combination in definitive therapy, with 62.7% (47/75) in the MSI group and 42.3% (11/26) in the non-MSI group (p = 0.070).
Univariate analysis results indicated that the variables associated with CRKP MSI were as follows (Table 1): ICU admission (p = 0.011), invasive mechanical ventilation (p = 0.017), nasogastric or nasobiliary tube (p = 0.001), urinary catheter (p = 0.027), central venous catheterization (p = 0.010), previous surgery (p = 0.003) and a PBS > 4 (p = 0.029).
Multivariate analysis indicated that previous surgery (OR 3.971, 95% CI 1.504–10.480, p = 0.005) and ICU admission (OR 3.322, 95% CI 1.252–8.816, p = 0.016) were independent risk factors for CRKP MSIs (Table 3). The logistic regression model was credible, as indicated by a Hosmer–Lemeshow test result of p = 0.862.
2.3. Risk Factors for CRKP MSI Mortality
According to the prognosis, patients with CRKP MSIs were divided into a survival group (n = 38) and a death group (n = 37). Compared with the survival group, patients in the death group had a higher proportion of admission to the ICU (86.5% vs. 60.5%, p = 0.011), exposure to carbapenems (48.6% vs. 23.7%, p = 0.024) and received more invasive mechanical ventilation (83.8% vs. 47.4%, p = 0.001) (Table 4).
Multivariate analysis indicated that ICU admission (OR 4.765, 95% CI 1.192–19.054, p = 0.027), a PBS > 4 (OR 3.820, 95% CI 1.218–11.983, p = 0.022) and thrombocytopenia (OR 8.650, 95% 2.573–29.007, p < 0.001) were independent risk factors for mortality (Table 5). The p-value of the Hosmer–Lemeshow test was 0.802, indicating that the logistic regression model was valid.
3. Discussion
CRKP has imposed enormous threats to public health nowadays. As an important bacterial pathogen, CRKP can cause various types of nosocomial infections. Nevertheless, available treatment options for CRKP MSIs remain limited. This study primarily focused on CRKP MSIs. A high mortality up to 49.3% has been observed in patients with CRKP MSIs. Previous surgery and ICU admission were independent risk factors for CRKP MSI. ICU admission, a PBS > 4 and thrombocytopenia were associated with the mortality of CRKP MSI.
In our study, CRKP MSI was most commonly found in the gastroenterology department, and severe acute pancreatitis was the primary cause of hospitalization. Similar results were found by Yuan et al., who discovered that digestive diseases were independently associated with CRKP BSI [9]. Digestive system diseases are often accompanied by intestinal barrier function disruption and gut flora disorder [10]. Additionally, patients with severe acute pancreatitis had a more critical condition and a higher incidence of Gram-negative organism infection [11]. BSI accounts for 30–60% of the complications of severe acute pancreatitis, and most pathogens isolated from BSI patients are Gram-negative bacteria [12,13]. We, therefore, believe that patients with digestive diseases need close attention, especially those with severe acute pancreatitis.
Besides the gastroenterology department, CRKP MSI also occurred frequently in the burn department. The majority of these patients had severe burns with extensive skin barrier damage. They suffered from multiple surgeries, exposure to various antibiotics and invasive operations, all of which put them at a higher risk of contracting and spreading CRKP. Previous studies have discovered that the detection rates of CRKP in burn-injured patients were significantly higher, and these patients were more vulnerable to CRKP BSI [14,15]. Based on this information, strict contact isolation precautions are urgently needed.
It has been well established that ICU hospitalization is a risk factor for the spread of infections with multidrug-resistant bacteria. Compared with general wards, the detection rates of CRKP in the ICU were significantly higher [16,17]. In the present study, the MSI group were more likely be admitted to the ICU and had a longer length of ICU stay. The difference in the cause of admission may be primarily responsible for the result. In the MSI group, most patients suffered from severe acute pancreatitis and large-area burns. Studies have confirmed that these diseases could lead to increased susceptibility to CRKP infection [18,19]. Furthermore, patients in the ICU are critically ill and often receive various invasive treatment, such as sputum suction and endotracheal intubation. These operations can damage the mucosa, which ultimately raises the risk of MSI. The association between CRKP BSI and previous surgeries has been confirmed [6,20]. Our results also revealed that previous surgeries were an independent risk factor for CRKP MSI. Surgery was a crucial link in the treatment and substantially affected the prognosis. However, invasive procedures may damage physical barriers and result in a longer hospitalization. According to Mittal et al., hospitalization can enhance the probability of multidrug-resistant strain colonization [21]. And CRKP colonization was closely associated with nosocomial infections [22]. Impaired body barriers and infections with resistant bacteria complicate the condition, leading to a poor prognosis.
High resistance rates of CRKP to various broad-spectrum Gram-negative agents have been widely reported [4,23]. Therefore, timely adjustments of treatment based on the results of antimicrobial susceptibility test is the cornerstones of therapy. According to our findings, both the MSI group and non-MSI group were most susceptible to tigecycline. This provides a theoretical basis for us to use for treatment. However, the use of tigecycline for CRKP infections remains controversial [24]. Due to its unique pharmacokinetics, the concentration of tigecycline in tissues is much higher than in the serum. Taking standard doses of tigecycline may not reach the blood concentration that effectively kills most Gram-negative bacteria [25]. Combination therapy survival benefit for CRKP infections, though established [26,27,28], was not observed in our study. This discrepancy may stem from limited sample size, reducing the statistical power, with high baseline PBS scores masking treatment effects and restricted antibiotic options narrowing therapeutic differences. These findings warrant larger-scale validation.
In the present study, the mortality rate in the MSI group (49.3%) was significantly higher than in the non-MSI group (23.1%). Furthermore, the mortality of CRKP MSI was significantly associated with ICU admission, a PBS > 4 and thrombocytopenia, but not with gender and age. According to the study of Xu et al., CRKP patients admitted to the ICU had a higher mortality than the pooled mortality, at 48.9% and 42.14%, respectively [29]. Liu et al. and Chang et al. similarly confirmed that ICU admission increased the mortality risk of CRKP patients [30,31]. Consequently, it was not unexpected for us to find that ICU admission is a risk factor for mortality. The PBS can assess the severity of severe infections, such as BSI [32]. A higher PBS is associated with a higher mortality rate in CRKP BSI [33]. According to our findings, patients with a PBS > 4 also had a significantly higher mortality. Sezgi C et al. reported that a reduction in platelet count is an independent risk factor for patients in the ICU [34]. Moreover, the value of the platelet count in assessing condition severity and forecasting prognosis in critically ill patients was further proven by Zhang et al. [35]. Consistent with prior studies, we found that a lower platelet count was independently associated with mortality in patients with CRKP MSI. The presence of severe infection, disseminated intravascular coagulation and multiple-organ failure may be responsible for the result. No significant correlations between gender and the mortality of CRKP MSIs were found in our study, which is in line with other studies [5,6,25]. Due to poor immunity and underlying diseases, the elderly are vulnerable to developing BSI. And there was a markedly increased risk of mortality in patients aged > 65 years, indicating the complicated conditions of BSI among older adults [36]. However, in the present study, age was not found to be significantly correlated to a higher mortality for CRKP MSI. This may be related to the fact that most patients in our study were critically ill and often deteriorated rapidly to death.
Certain limitations exist in our study. First, it was a retrospective study and was conducted at a single center. Second, we did not perform the molecular characterization on CRKP isolates to determine carbapenem resistance mechanisms. Third, the definition of MSI in this study was CRKP BSI patients with other sites infection, such as urinary tract infection, pneumonia and abdominal infection. Subgroup analysis based on the number of co-infection sites is required. Lastly, while treatment strategies were analyzed, the lack of detailed pharmacological data—including specific dosages, pharmacokinetic interactions and treatment timelines—precluded deeper mechanistic analyses.
4. Materials and Methods
4.1. Design and Study Population
From January 2017 to December 2021, this retrospective study was carried out at a tertiary teaching hospital in Xi’an, China. The inclusion criterion was as follows: inpatients who met the CDC/NHSN diagnostic criteria for a CRKP BSI [37]. The exclusion criteria were as follows: (a) blood culture results indicating a polymicrobial infection and (b) missing or incomplete medical record information. After excluding specific patients, a total of 101 patients (77 males and 24 females), with an age range of 42 to 64 years (median: 52 years), were enrolled. In our analysis, only the first episode of CRKP BSI was analyzed. According to the presence of other site infections, all patients were further subdivided into the MSI group and the non-MSI group.
4.2. Data Collection and Definitions
The data collection included demographics, comorbidities, the cause of admission, the probable source of BSI, previous hospitalization (within one month), previous surgery (within one month), recent invasive procedures, ICU admission, length of hospital and ICU stay, antibiotic exposure and outcomes.
The detection of CRKP at the anatomical site was the prerequisite for diagnosing CRKP infection. Meanwhile, clinical signs and symptoms compatible with the infection were required. Each patient’s infection/colonization status was evaluated by two experts. CRKP BSI was defined as a positive blood culture with the presence of signs and symptoms of an infection (fever, chills or hypotension). Based on the microbiological findings and clinical symptoms, the primary site of the BSI was found. If the BSI pathogen matched the pathogen for the specific site, with a collection date in the secondary BSI attribution period, the BSI was considered secondary to the event. When the primary site could not be determined, the primary BSI was recorded. Primary sites were categorized as follows: lower respiratory tract infection, intra-abdominal infection, urinary tract infection, skin and soft tissue infection, venous central catheter infection and others.
CRKP was defined as Klebsiella pneumoniae that was not susceptible to any carbapenems (MIC ≥ 4 μg/mL for meropenem or imipenem; MIC ≥ 2 μg/mL for ertapenem) [38]. Receiving antibiotic treatment more than 48 h before a BSI was considered antibiotic exposure. The initial positive blood culture date was utilized to establish the onset of BSI. Within 24 h of a BSI being diagnosed, clinical data were collected and the Pitt bacteremia score (PBS) was calculated, with the worst value being recorded. PBS was based on five variables, including temperature, blood pressure, the need for mechanical ventilation, mental status and the presence of cardiac arrest. Single-active antibiotic treatment was defined as monotherapy, whereas multiple-active antibiotic administration was defined as combination therapy. Appropriate therapy was defined as receiving an antimicrobial with in vitro activity based on drug susceptibility results. Antimicrobial therapy administered before antibiotic susceptibility results were obtained was defined as empirical antibiotic treatment. Antimicrobial treatment based on conclusive antibiotic susceptibility results was defined as definitive antibiotic therapy.
4.3. Antimicrobial Susceptibility Testing
Bacterial identification was performed using the Vitek 2 system (bioMerieux, Marcy-l’Etoile, Lyon, France). The Kirby–Bauer disk diffusion method was performed to ascertain antimicrobial susceptibility to some agents: cefoperazone/sulbactam, tetracycline, cefuroxime, ceftazidime/avibactam, meropenem, biapenem, doxycycline and tigecycline. Other antibiotics susceptibility tests for the strains were examined by Gram-negative susceptibility (GNS) cards on the Vitek system (bioMérieux, Marcy-l’Etoile, France). All tests were performed according to the Clinical and Laboratory Standards Institute (CLSI) guidelines (CLSI M100). And findings were interpreted in terms of the guidelines of CLSI M100. Controls for antimicrobial susceptibility testing were Pseudomonas aeruginosa ATCC 27853 and Escherichia coli ATCC 25922.
4.4. Statistical Analysis
Continuous variables are expressed as the means and standard deviations (SD) if normally distributed, otherwise as the median and interquartile range (IQR). Depending on their distribution, continuous variables were compared using either the Mann–Whitney U test or Student’s t-test. Frequencies and proportions were used to describe categorical variables. Chi-square test or Fisher’s exact test were used to compare categorical variables. Variables with p < 0.05 in the univariable analysis were entered into the multivariate logistic model. SPSS version 22.0 (IBM, Armonk, NY, USA) was used for statistical analysis.
5. Conclusions
In summary, CRKP MSI complicated the condition and treatment, and thus eventually led to a significantly higher mortality. Previous surgery and ICU admission were independent risk factors for CRKP MSI. ICU admission, a PBS > 4 and thrombocytopenia were independent predictor of mortality, whereas other clinical factors, such as gender and age, were not correlated with mortality. Understanding these risks may contribute to identifying high-risk populations and formulating more intervention strategies to decrease the risk of developing CRKP MSI and mortality.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nordmann P. Naas T. Poirel L. Global spread of Carbapenemase-producing Enterobacteriaceae Emerg. Infect. Dis.2011171791179810.3201/eid 1710.11065522000347 PMC 3310682 · doi ↗ · pubmed ↗
- 2Shrivastava S.R.L. Shrivastava P.S. Ramasamy J. World health organization releases global priority list of antibiotic-resistant bacteria to guide research, discovery, and development of new antibiotics J. Med. Soc.2018327610.4103/jms.jms_25_17 · doi ↗
- 3Hu F.P. Guo Y. Zhu D.S. Wang F. Jiang X.F. Xu C.Y. Zhang X.J. Zhang Z.X. Ji P. Xie Y. CHINET surveillance of bacterial resistance: Results of 2020 Chin. J. Infect. Chemother.202121377387
- 4Ahmadi Z. Noormohammadi Z. Behzadi P. Ranjbar R. Molecular Detection of gyr A Mutation in Clinical Strains of Klebsiella pneumoniae Iran. J. Public Health 2022512334233910.18502/ijph.v 51i 10.1099236415795 PMC 9647615 · doi ↗ · pubmed ↗
- 5Zhang G. Zhang M. Sun F. Zhou J. Wang Y. Zhu D. Chen Z. Chen Q. Chang Q. Liu H. Epidemiology, mortality and risk factors for patients with K. pneumoniae bloodstream infections: Clinical impact of carbapenem resistance in a tertiary university teaching hospital of Beijing J. Infect. Public Health 2020131710171410.1016/j.jiph.2020.09.01233082112 · doi ↗ · pubmed ↗
- 6Li Y. Li J. Hu T. Hu J. Song N. Zhang Y. Chen Y. Five-year change of prevalence and risk factors for infection and mortality of carbapenem-resistant Klebsiella pneumoniae bloodstream infection in a tertiary hospital in North China Antimicrob. Resist. Infect. Control 202097910.1186/s 13756-020-00728-332487221 PMC 7268443 · doi ↗ · pubmed ↗
- 7Wu D. Chen C. Liu T. Wan Q. Risk Factors for Acquisition of Carbapenem-Resistant Klebsiella pneumoniae and Mortality Among Abdominal Solid Organ Transplant Recipients with K. pneumoniae Infections Med. Sci. Monit.202026 e 92299610.12659/MSM.92299632807765 PMC 7458125 · doi ↗ · pubmed ↗
- 8Paterson D.L. Ko W.C. Von Gottberg A. Mohapatra S. Casellas J.M. Goossens H. Mulazimoglu L. Trenholme G. Klugman K.P. Bonomo R.A. International prospective study of Klebsiella pneumoniae bacteremia: Implications of extended-spectrum beta-lactamase production in nosocomial Infections Ann. Intern. Med.2004140263210.7326/0003-4819-140-1-200401060-0000814706969 · doi ↗ · pubmed ↗