Giant right coronary artery aneurysm with associated dissection: diagnosis and surgical management
Henri Bartolozzi, Darragh Rice, Mikaela Forde, Fabio Bartolozzi

TL;DR
This paper describes a rare case of a giant right coronary artery aneurysm in an elderly woman and the surgical steps taken to manage it.
Contribution
The paper presents a unique case of a giant coronary artery aneurysm with dissection and its successful surgical management.
Findings
The patient had an 85 mm giant right coronary artery aneurysm causing pericardial irritation and right heart compression.
Surgical resection and bypass using a saphenous vein graft were performed, revealing a dissected aneurysm wall at risk of rupture.
The case emphasizes the need for timely diagnosis and surgical intervention in managing giant coronary artery aneurysms.
Abstract
Coronary artery aneurysms are defined as a focal dilatation exceeding 1.5 times the diameter of the adjacent normal segment. They are found in up to 5% of patients undergoing coronary angiography. Giant coronary artery aneurysms (GCAAs), typically defined as >20 mm in diameter, with an incidence of ⁓0.02%. We present the case of an 82-year-old female who underwent coronary artery bypass grafting due to a giant right coronary artery aneurysm measuring 85 mm, identified on preoperative contrast-enhanced computed tomography (CT). The patient exhibited symptoms consistent with pericardial irritation secondary to aneurysms size and was found to have significant right heart compression. Surgical intervention included opening and resection of the aneurysmal sac and bypassing the affected segment using a saphenous vein graft. Intraoperatively, it was discovered that the aneurysm wall was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
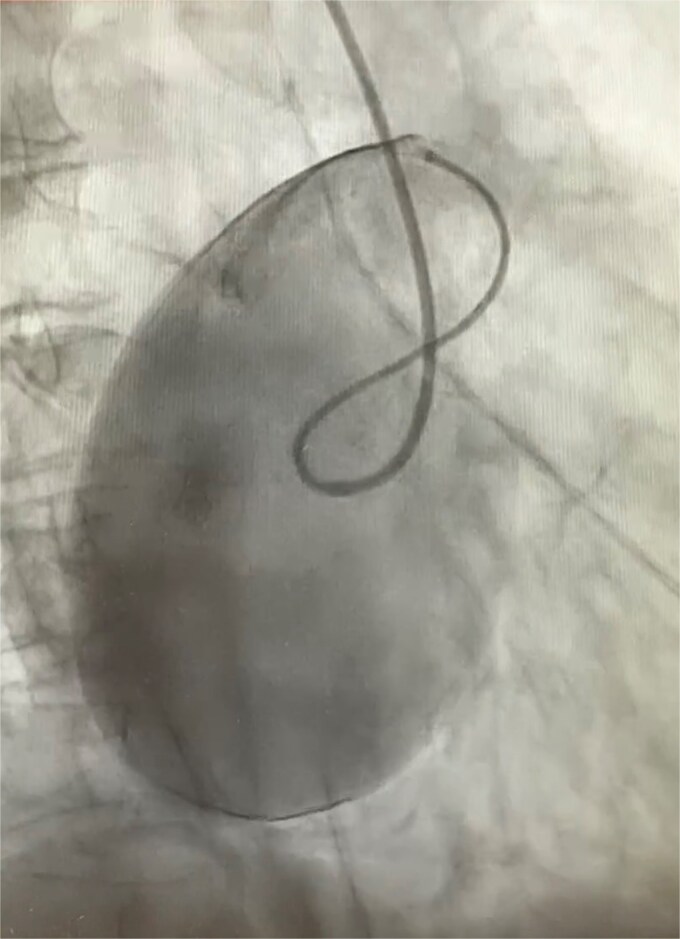 Figure 1
Figure 1 Figure 2
Figure 2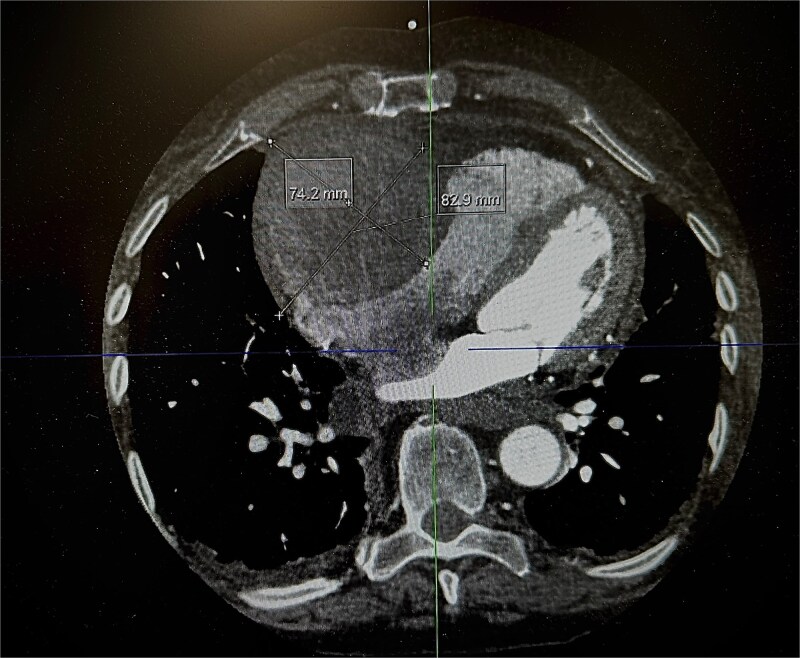 Figure 3
Figure 3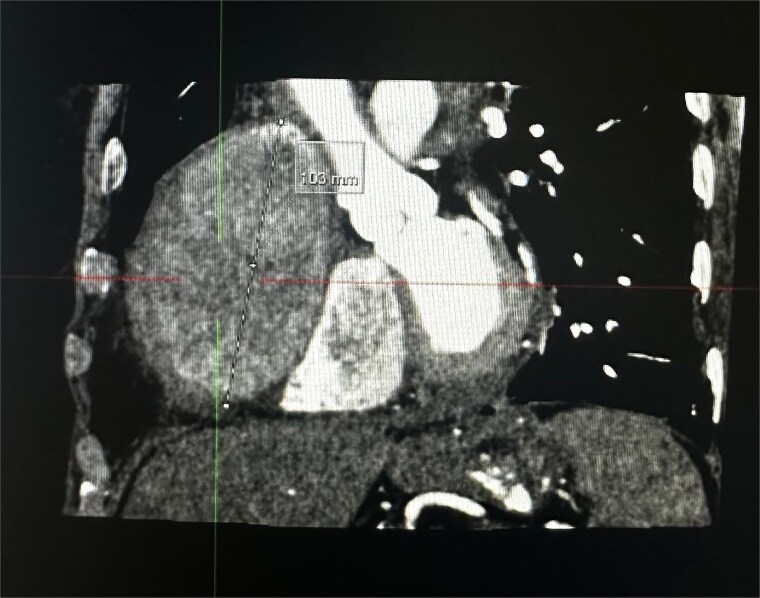 Figure 4
Figure 4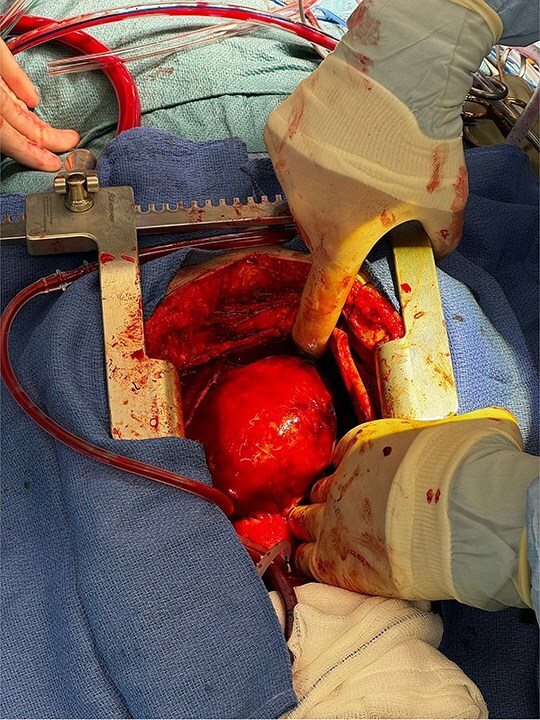 Figure 5
Figure 5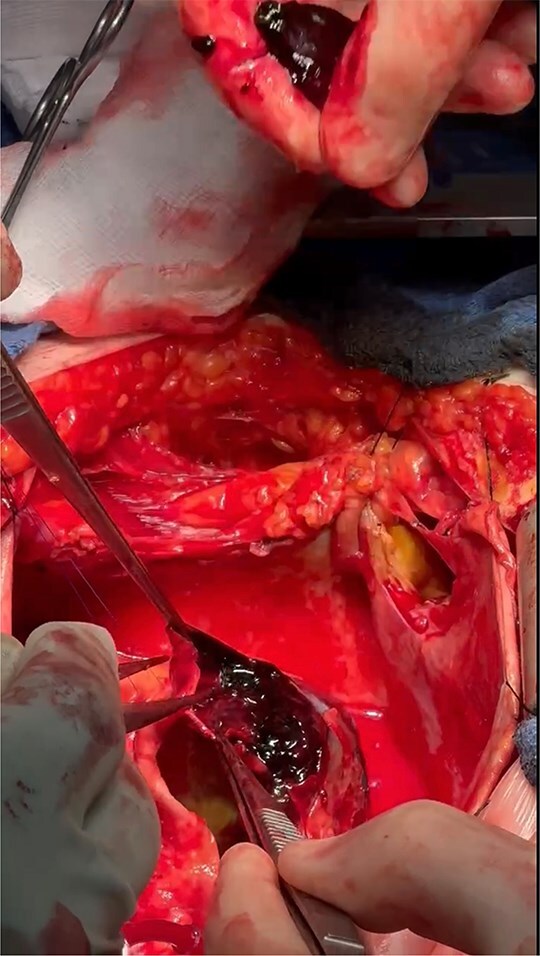 Figure 6
Figure 6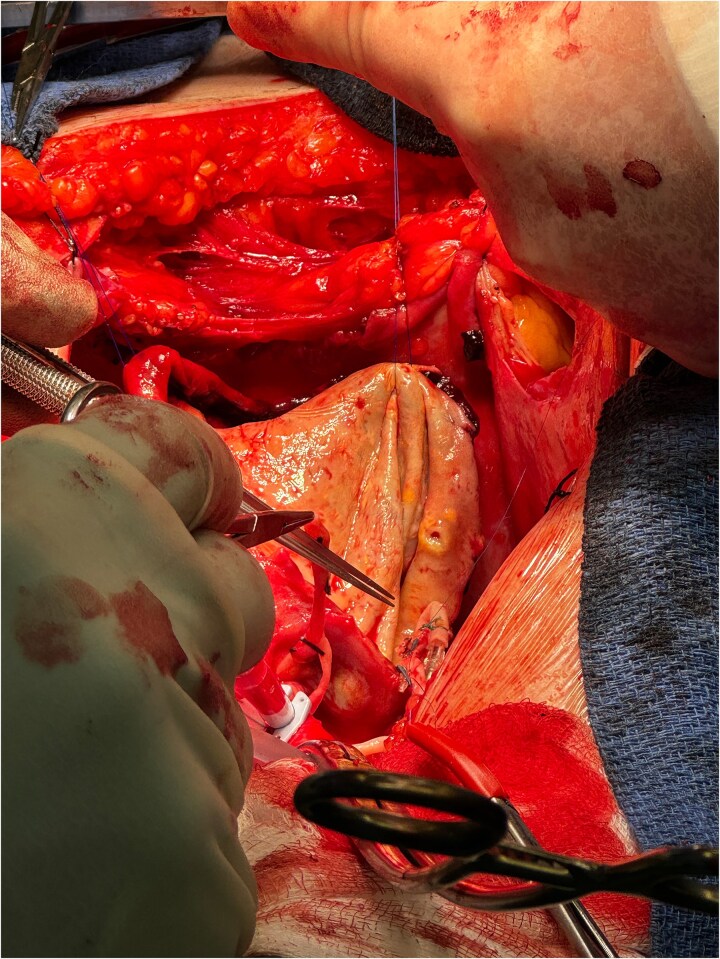 Figure 7
Figure 7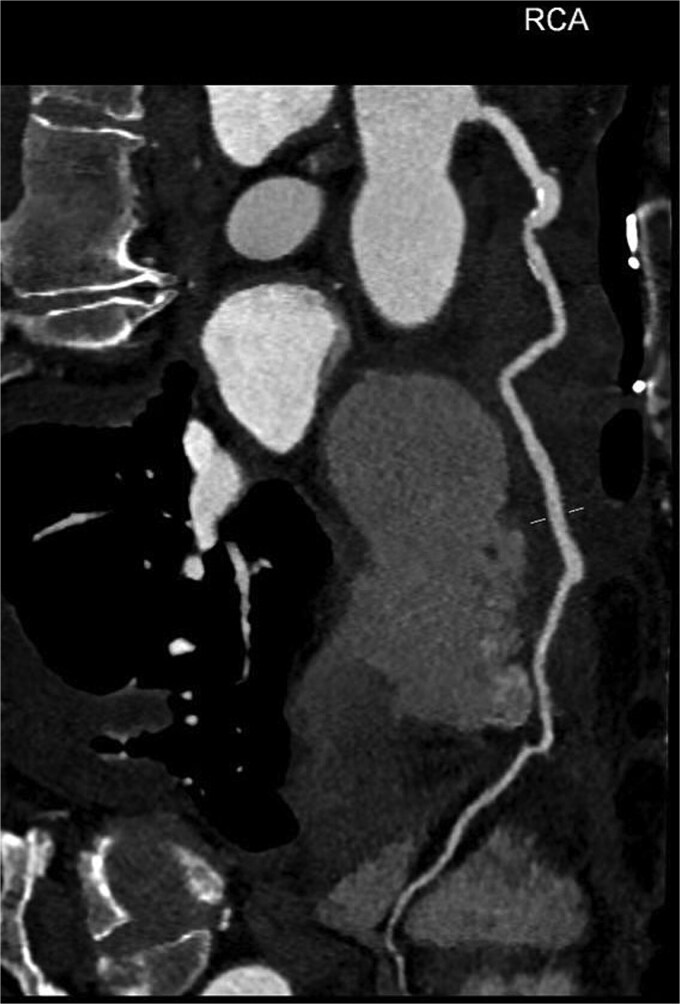 Figure 8
Figure 8Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsKawasaki Disease and Coronary Complications · Coronary Artery Anomalies · Cardiac Structural Anomalies and Repair
Introduction
A focal expansion of the coronary artery that is ˃1.5 times the diameter of the adjacent normal section is known as a coronary artery aneurysm (CAA) [1]. CAAs are a rare clinical entity, occurring most commonly as a sequelae of atherosclerosis, but can be associated with certain disorders such as Kawasaki’s disease. Similar to other aneurysms, they can be classified as saccular or fusiform and although most patients are asymptomatic, they can result in thrombosis, distal embolization, external compression or rupture [2].
Rarely, CAAs can grow to such a size that they are referred to as giant CAAs; their incidence has been reported to be 0.02% [1]. There is no widely recognized, single definition of a giant CAA, In the medical literature, sizes ˃20 mm, 40 mm, 50 mm, and quadruple the reference-vessel diameter have all been suggested as definitive [1]. Location wise, the right coronary artery is the most frequently affected in 40.4% of cases, followed by the left anterior descending artery with 32.3%, with the left main stem and circumflex being rarely involved (3.5%) [3].
Case presentation
An 82-year-old female presented to the emergency department complaining of progressive severe central chest that was pleuritic in nature, radiating to her right arm. Following a bedside echo, the patient underwent coronary angiography, where a giant right CAA was diagnosed (Fig. 1). Subsequent, contrast computed tomography (CT) scan further characterized the aneurysm, and highlighted significant compression was uncovered compressing both the right atrium and ventricle (Fig. 2). The right coronary aneurysm was measured cross-sectional dimensions of 8.3 × 7.4 cm (Fig. 3) and 10 cm in length (Fig. 4). Following Heart Team discussion, the patient was scheduled for an aneurysmectomy and coronary artery bypass to repair the extensive disease.
Right coronary angiogram highlighting the aneurysm.
3D reconstruction from CT thorax showing the right coronary aneurysm compressing right heart.
Axial plane of a contrast thorax CT scan showing the giant right coronary aneurysm.
Coronal plane of a contrast thorax CT scan showing the giant coronary aneurysm.
The operation was performed via median sternotomy, with the aneurysm immediately visible post sternotomy (Fig. 5). The pericardium was carefully opened without complication, and due to the right atrium being inaccessible, cardio-pulmonary bypass was established using central ascending aortic cannulation and femoral venous cannulation, with antegrade cardioplegia (Fig. 5). The giant CAA was then opened directly where it was uncovered that the aneurysm wall had also dissected, and was paper thin (Fig. 6). The thrombus was evacuated, perforating branches were identified and oversewn, of which there were two. Following this, an endoscopically harvested saphenous vein graft was used to directly, end-to-end anastomose the proximal and distal necks of the aneurysm, bypassing the sac entirely (Fig. 7). The patient was successfully weaned from Cardiopulmonary Bypass and the procedure concluded without complication.
Exposed right coronary aneurysm post sternotomy.
Dissected aneurysm wall with thrombus formation.
Direct anastomosis of saphenous conduit to the distal neck of the aneurysm using an end-to-end technique.
Following the surgery, the patient remained in intensive care for 2 days, and progressed as expected over the coming week. She was discharged on day 8 postoperatively, with the only postoperative complication being a short run of an atrial tachycardia that was medically managed and was in sinus rhythm at the time of discharge. Prior to discharge a CT Coronary Angiogram with contrast was performed which highlights the repair (Fig. 8). She was reviewed in outpatients six weeks post procedure and has made a full recovery.
Reconstructed path of right coronary artery including vein graft via aneurysmal sac from post-operative CT coronary angiogram.
Discussion
The prevalence of CAAs on angiography ranges from 0.15% to 4.9%, making them extremely uncommon, with a higher prevalence in men [4]. However, giant coronary aneurysms are even more rare with an incidence of 0.02%. In adults, atherosclerosis is the cause of half of CAAs making it the most prevalent cause of these conditions [5]. Kawasaki disease, vasculitidies (polyarteritis nodosa and Takayasu's arteritis), lupus erythematosus, connective tissue disorders, congenital defects, infections (like Lyme disease, syphilis, and narcotic emboli), trauma, dissection, cocaine abuse, and iatrogenic and idiopathic origins, genetic causes such as connective tissue diseases like Marfan's and Ehlers-Danlos syndromes are further known causes [3, 6, 7].
In patients with CAAs, surgical management becomes necessary when aneurysms are symptomatic or large, as these can lead to serious complications like rupture or myocardial ischemia. Surgical approaches generally involve aneurysm resection or ligation, frequently accompanied by coronary artery bypass grafting to restore adequate blood flow when the aneurysm obstructs a major artery. In more challenging cases, involving critical coronary branches, advanced grafting techniques are necessary to optimize perfusion and prevent ischemic events [8]. Although surgery carries a high level of risk, it remains essential in preventing potentially severe outcomes associated with untreated CAAs [8].
Conclusion
This case illustrates the importance of early diagnosis and tailored surgical management for giant CAAs, which can lead to severe complications like cardiac compression and rupture. Prompt imaging and surgical intervention, including aneurysm resection and bypass grafting, enabled a positive outcome for this patient.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pham V, de Hemptinne Q, Grinda J-M, et al. Giant coronary aneurysms, from diagnosis to treatment: a literature review. Arch Cardiovasc Dis 2019;113:59–69.31866173 10.1016/j.acvd.2019.10.008 · doi ↗ · pubmed ↗
- 2Matta AG, Yaacoub N, Nader V, et al. Coronary artery aneurysm: a review. World J Cardiol 2021;13:446–55. 10.4330/wjc.v 13.i 9.44634621489 PMC 8462041 · doi ↗ · pubmed ↗
- 3Brilakis E . Coronary angiography. In: Manual of Percutaneous Coronary Interventions. 2021, (p. 97‑109). Elsevier, 2021, 97–109. 10.1016/b 978-0-12-819367-9.00006-8
- 4Sheikh AS, Hailan A, Kinnaird T, et al. Coronary artery aneurysm: evaluation, prognosis, and proposed treatment strategies. Heart Views 2019;20:101–8. 10.4103/HEARTVIEWS.HEARTVIEWS_1_1931620255 PMC 6791093 · doi ↗ · pubmed ↗
- 5Hack F, Steinbach R, Wöhrer C, et al. Dissection of a giant coronary aneurysm, radiology. Radiol Cardiothorac Imaging 2023;5:e 220254. 10.1148/ryct.22025436860836 PMC 9969207 · doi ↗ · pubmed ↗
- 6Crawley PD, Mahlow WJ, Huntsinger DR, et al. Giant coronary artery aneurysms: review and update. Tex Heart Inst J 2014;41:603–8. 10.14503/THIJ-13-389625593524 PMC 4251331 · doi ↗ · pubmed ↗
- 7Marla R, Ebel R, Crosby M, et al. Multiple giant coronary artery aneurysms. Tex Heart Inst J 2009;36:244–6.19568397 PMC 2696511 · pubmed ↗
- 8Singh SK, Goyal T, Sethi R, et al. Surgical treatment for coronary artery aneurysm: a single-Centre experience. Interact Cardiovasc Thorac Surg 2013;17:632–6. 10.1093/icvts/ivt 28223803224 PMC 3781802 · doi ↗ · pubmed ↗