Delayed recognition of peripartum cardiomyopathy presenting with severe heart failure: a case report
Nordini Asri, Suraya Abdul-Razak, Mohd Fazrul Mokhtar, Khairul Shafiq Ibrahim, Roqiah Fatmawati Abdul Kadir

TL;DR
A case report shows a woman developed heart failure months after childbirth, initially misdiagnosed, but recovered after proper treatment for peripartum cardiomyopathy.
Contribution
Highlights the diagnostic challenge of delayed-onset peripartum cardiomyopathy and emphasizes the need for early treatment.
Findings
The patient's ejection fraction improved from 16% to 56% after guideline-directed medical therapy.
Delayed-onset peripartum cardiomyopathy can be misdiagnosed despite multiple medical visits.
Early initiation of heart failure treatment leads to full functional recovery.
Abstract
Peripartum cardiomyopathy (PPCM) is a rare but potentially fatal cause of heart failure that occurs towards the end of pregnancy or within the first 5 months postpartum, in the absence of other identifiable cause of cardiac dysfunction. It is characterized by left ventricular systolic impairment, with an ejection fraction (LVEF) typically ≤ 45%. While most cases are diagnosed shortly after delivery, delayed presentations can occur, leading to significant diagnostic challenges and complicate treatment. We report a case of a 40-year-old multiparous (Para 3) woman, who developed progressive dyspnoea beginning 2 months after delivery. Despite two earlier medical care visits, her symptoms were initially misdiagnosed. She represented with overt symptoms of heart failure 1 month later. Investigations encompassing transthoracic echocardiography, cardiac magnetic resonance imaging, coronary…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
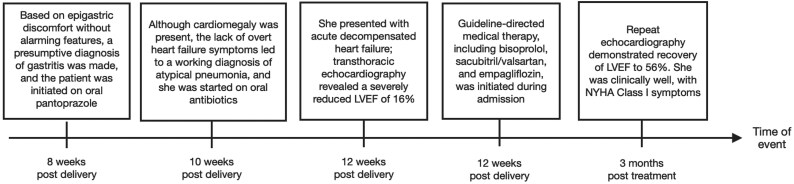 Figure 1
Figure 1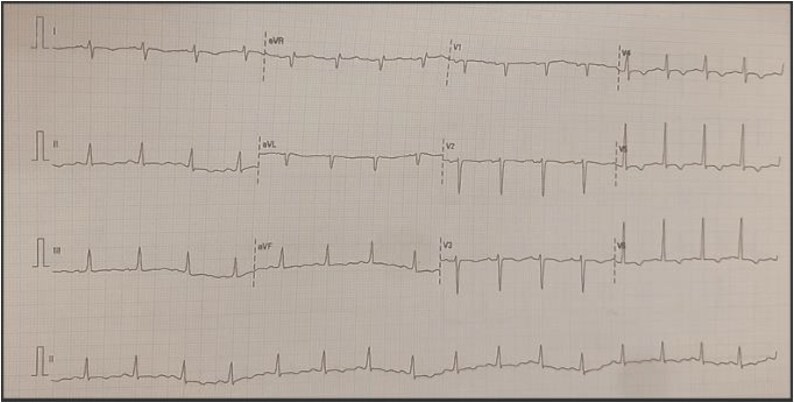 Figure 1
Figure 1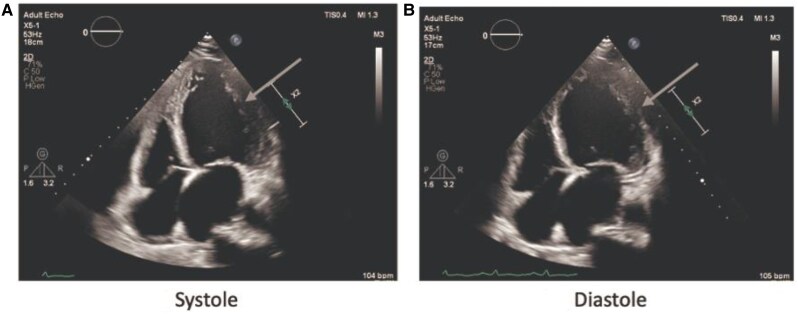 Figure 2
Figure 2 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular Issues in Pregnancy · Cardiac Structural Anomalies and Repair · Takotsubo Cardiomyopathy and Associated Phenomena
Introduction
Peripartum cardiomyopathy (PPCM) is a rare, potentially life-threatening form of heart failure occurring in the last month of pregnancy or within 5 months postpartum, marked by new-onset systolic dysfunction (left ventricular ejection fraction LVEF ≤ 45%) without an identifiable cause.^1^ The incidence ranges from 1 in 15 000 to 1 in 100 live births, influenced by genetic, socioeconomic, and healthcare factors.^2^
Symptoms including dyspnoea, fatigue, and oedema often mimic normal peripartum physiology, contributing to diagnostic delays. Early recognition and treatment improve outcomes through neurohormonal modulation and ventricular remodelling.^3^
Management generally follows guideline-directed medical therapy (GDMT) for heart failure with reduced ejection fraction (HFrEF), including beta-blockers, angiotensin-converting enzyme inhibitors or angiotensin receptor-neprilysin inhibitors, and sodium–glucose cotransporter-2 (SGLT2) inhibitors. Their use in PPCM is extrapolated from HFrEF trials and remains off-label. This case illustrates a delayed diagnosis and subsequent recovery following GDMT, highlighting the need for clinical vigilance.
Summary figure
**
Case presentation
A 40-year-old woman, para 3, presented to a primary care clinic with exertional dyspnoea starting 2 months postpartum. Initial symptoms of mild breathlessness and epigastric discomfort were managed as gastritis. Subsequently, she developed a productive cough without fever and was treated empirically for atypical pneumonia.
At 3 months postpartum, she represented with worsening dyspnoea, reduced effort tolerance, orthopnoea, paroxysmal nocturnal dyspnoea, abdominal discomfort, fatigue, and mild pedal oedema. She had no history of hypertension, diabetes, cardiac disease, or substance use. There was no family history of cardiomyopathy or sudden cardiac death. Her antenatal course was uneventful, with consistently normal blood pressure readings (114–126/68–80 mmHg), and no signs of pre-eclampsia. She was breastfeeding and not on regular medication.
She was mildly tachypnoeic (RR 22), SpO₂ 95% room air, blood pressure 144/95 mmHg, heart rate 107 bpm, without jugular venous distention. Capillary glucose was 9.7 mmol/L. Auscultation revealed dual heart sounds without any murmurs. Bibasilar crepitations and mild bilateral oedema were present. Hepatomegaly was evident with a tender liver palpable 4 cm below the right costal margin. Peripheral perfusion was intact.
Electrocardiography (ECG) showed widespread T-wave inversions (see Figure 1). Chest x-ray revealed cardiomegaly and pulmonary congestion. Blood investigations showed normal haemoglobin, renal and liver profile, troponin T, thyroid function, and HbA1c (5.6%). NT proBNP was elevated at 4320 pg/mL. The echocardiogram showed a dilated left ventricle with an LVEF of 16%, global hypokinesia, pseudo-normal diastolic filling, enlarged left atrium, mild right ventricle dilatation, and moderate mitral and tricuspid regurgitation (see Supplementary Video 1–5). No pericardial effusion or regional wall motion abnormalities were noted (see Figure 2).
Electrocardiogram with widespread T-wave inversion. Reproduced with permission from Hospital Al-Sultan Abdullah, HASA UiTM, 2025.
(A) and (B) showed evidence of left ventricle dilatation and global hypokinesia.
Coronary angiogram showed normal vessels. Cardiac MRI confirmed biventricular dysfunction (LVEF 20% and RVEF 22%). There was a subtle intramyocardial late gadolinium enhancement pattern consistent with dilated non-ischaemic cardiomyopathy. Mild diffuse oedema on T2 STIR images, along with a slight increase in native T1 and T2 mapping (see Figure 3).
MRI of the heart showing (A) the longitudinal 4-chamber views demonstrate a dilated left ventricle with an end-diastolic volume of 126 mL/m². There is global hypokinesia observed on cine steady-state free precession images, with reduced left and right ventricular systolic functions of 20% and 22%, respectively. A pericardial effusion with a maximal thickness of 1.3 cm is also noted. (B) The late gadolinium short-axis image showed subtle intramyocardial enhancement, particularly in the septal and anterior walls. (C) and (D) Mid-ventricular septal measurements of T1 and T2 mapping demonstrate slight increases in T1 and T2 mapping values, respectively.
She was admitted and started on intravenous furosemide and oxygen. GDMT was initiated with sacubitril/valsartan 24/26 mg twice daily, empagliflozin 10 mg once daily, bisoprolol 1.25 mg once daily, and spironolactone 25 mg once daily. These medications were gradually up titrated based on clinical response. The patient tolerated the treatment well without adverse effects. All medications were selected based on lactation safety. She responded well and she was discharged after 3 days.
At 3-month follow-up, she was asymptomatic (NYHA Class I) with normalized left ventricular function (LVEF of 56%). NT-proBNP was not repeated. She remained clinically stable on maintenance therapy.
Discussion
This case highlights the diagnostic complexity of PPCM, where symptoms overlap with normal postpartum physiology. Initial misdiagnoses underscore the need for heightened suspicion in postpartum women with unexplained dyspnoea. Differential diagnoses include pre-existing cardiomyopathy, pulmonary embolism, and infection.^4^
The pathophysiology may involve inflammation, oxidative stress, angiogenic imbalance, and genetic susceptibility. Risk factors include advanced maternal age, multiple gestations, multiparity, and hypertensive disorders.^2,4,5^ In this case, advanced maternal age was the only apparent factor.
Echocardiography is the diagnostic cornerstone, complemented by NT-proBNP, ECG, chest imaging, and laboratory evaluation.^6–8^ Cardiac MRI aids in excluding other cardiomyopathies, although typical findings in PPCM are non-specific, such as global dysfunction, myocardial oedema, and subtle late gadolinium enhancement.^2,6^
Management follows HFrEF guideline,^9,10^ including diuretics, bisoprolol, spironolactone, SGLT2 inhibitor, and sacubitril/valsartan. Though effective in HFrEF, ARNI and SGLT2 inhibitors are off-label in PPCM and require cautious use.^2,11,12^ Counselling was provided to ensure continued breastfeeding and all prescribed medications were reviewed and supported by lactation safety data.^13^ The patient demonstrated marked improvement in LVEF from 16% to 56% and symptoms within 3 months.
Long-term follow-up is essential due to the risk of relapse, arrhythmias, or persistent cardiomyopathy.^2,14,15^ Recovery varies, with some patients normalizing cardiac function, while others experience lasting impairment or relapses.^2,14,15^ Counselling about future pregnancies is critical, as any subsequent pregnancy carries an elevated risk of recurrence.^2^ Our patient received a progestin-only implant (Implanon) to mitigate thromboembolic risks associated with oestrogen-containing methods.^2^ Breastfeeding was continued safely.
In summary, PPCM present diagnostic and management challenges. This case highlights the importance of postpartum vigilance and demonstrates favourable outcomes with timely GDMT. While HFrEF therapies show promise, further studies are needed to define their role in PPCM. Ongoing surveillance, cardiovascular risk reduction, and reproductive counselling are essential.
Supplementary Material
ytaf306_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bauersachs J, König T, van der Meer P, Petrie MC, Hilfiker-Kleiner D, Mbakwem A, et al Pathophysiology, diagnosis and management of peripartum cardiomyopathy: a position statement from the Heart Failure Association of the European Society of Cardiology Study Group on peripartum cardiomyopathy. Eur J Heart Fail 2019;21:827–843.31243866 10.1002/ejhf.1493 · doi ↗ · pubmed ↗
- 2Davis MB, Arany Z, Mc Namara DM, Goland S, Elkayam U. Peripartum cardiomyopathy. J Am Coll Cardiol 2020;75:207–221.31948651 10.1016/j.jacc.2019.11.014 · doi ↗ · pubmed ↗
- 3Arany Z, Elkayam U. Peripartum cardiomyopathy. Circulation 2016;133:1397–1409.27045128 10.1161/CIRCULATIONAHA.115.020491 · doi ↗ · pubmed ↗
- 4Elkayam U, Akhter MW, Singh H, Khan S, Bitar F, Hameed A, et al Pregnancy-associated cardiomyopathy. Circulation 2005;111:2050–2055.15851613 10.1161/01.CIR.0000162478.36652.7E · doi ↗ · pubmed ↗
- 5Isogai T, Kamiya CA. Worldwide incidence of peripartum cardiomyopathy and overall maternal mortality. Int Heart J 2019;60:503–511.31019181 10.1536/ihj.18-729 · doi ↗ · pubmed ↗
- 6Tsang MW, Lang RM. Peripartum cardiomyopathy: Etiology, clinical manifestation and diagnosis. Up To Date 2023. Updated 18 November 2024.
- 7Gita Setyanda YO, Yaswir R. The role of NT-pro BNP in the diagnosis of peripartum cardiomyopathy with multiple left ventricular thrombus: a case report. Biosci Med J Biomed Transl Res 2024;8:5084–5093.
- 8Sarma AA, Aggarwal NR, Briller JE, Davis M, Economy KE, Hameed AB, et al The utilization and interpretation of cardiac biomarkers during pregnancy. JACC Adv 2022;1:100064.38938393 10.1016/j.jacadv.2022.100064 PMC 11198183 · doi ↗ · pubmed ↗