Correlation between histopathological features and recurrence score according to menopausal status in HR+/HER2– breast cancer patients: a retrospective study
Federica Martorana, Sabrina Nucera, Gianmarco Motta, Maria Vita Sanò, Carlo Carnaghi, Marialuisa Puglisi, Claudia Gelsomino, Giuseppe Corsaro, Chiara Conti, Lucia Motta, Giuliana Pavone, Stefano Marletta, Giada Maria Vecchio, Gaetano Magro, Giuseppe Catanuto, Gaetano Castiglione

TL;DR
This study explores how histopathological features relate to a genomic recurrence score in breast cancer patients, finding differences based on menopausal status.
Contribution
The study reveals how menopausal status affects the relationship between histopathological features and genomic recurrence scores in breast cancer patients.
Findings
In pre-menopausal patients, PgR% predicted a higher recurrence score (RS > 16).
Post-menopausal patients showed significant correlations between RS and Ki67% and PgR%.
Histopathological features correlated differently with RS based on menopausal status.
Abstract
Clinico-pathological features have traditionally guided prognosis and adjuvant therapy for breast cancer (BC) patients. In the past decade, genomic tests such as Oncotype DX entered clinical practice to refine risk stratification and predict chemotherapy benefit for hormone-receptor positive (HR+)/human epidermal growth factor-receptor 2 negative (HER2–) BC patients after surgery. This is a retrospective analysis to investigate the correlation between histopathological parameters and recurrence score (RS), accounting for menopausal status. Data on HR+/HER2– early BC patients who underwent Oncotype DX were collected using an institutional database. Clinico-pathological characteristics were retrieved. Linear regression was used with RS as a continuous outcome, while logistic regression was performed for pre- and post-menopausal patients, dichotomizing RS at thresholds of 16 and 25,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
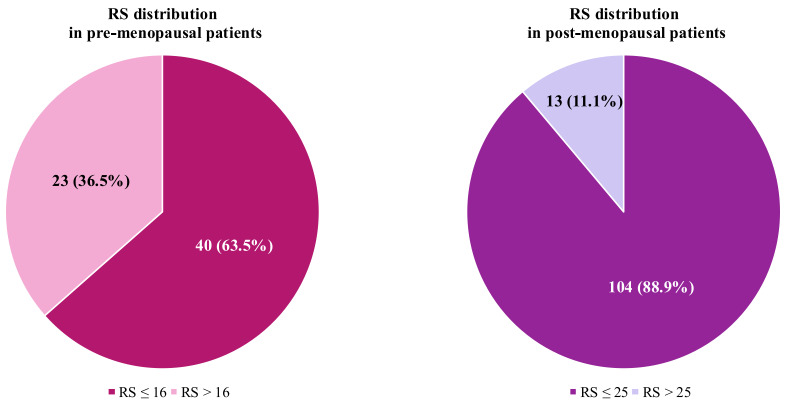 Figure 1
Figure 1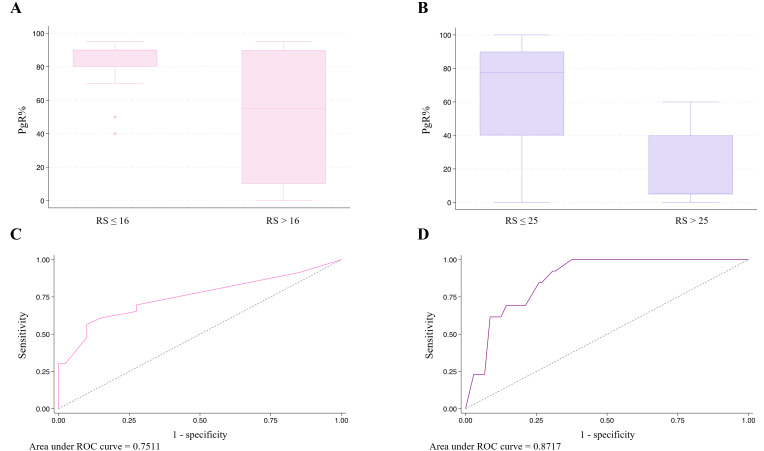 Figure 2
Figure 2|
|
|
|
|
|
|---|---|---|---|---|
| Age, years (median IQR) | 57.5 (49–67.5) | 47 (44–50) | 64 (58–69) |
|
| Tumor histology, | 0.60 | |||
| NST | 132 (73.3) | 49 (77.8) | 83 (70.9) | |
| Lobular | 32 (17.8) | 9 (14.3) | 23 (19.7) | |
| Other | 16 (8.9) | 5 (7.9) | 11 (9.4) | |
| Tumor size, mm (median IQR) | 18 (12.5–23) | 18 (12–25) | 18 (13–22) | 0.57 |
| pT, | 0.50 | |||
| pT1 | 111 (61.7) | 41 (65.1) | 70 (59.8) | |
| pT2 | 67 (37.2) | 22 (34.9) | 45 (38.5) | |
| pT3 | 2 (1.1) | - | 2 (1.7) | |
| Number of positive nodes, | 0.65 | |||
| 0 | 111 (61.7) | 42 (66.7) | 69 (59.0) | |
| 1 | 55 (30.5) | 18 (28.6) | 37 (31.6) | |
| 2 | 10 (5.6) | 3 (4.7) | 7 (6.0) | |
| 3 | 2 (1.1) | - | 2 (1.7) | |
| NA | 2 (1.1) | - | 2 (1.7) | |
| pN, | 0.39 | |||
| pN0 | 111 (61.7) | 42 (66.7) | 69 (59.0) | |
| pN1 | 67 (37.2) | 21 (33.3) | 46 (39.3) | |
| NA | 2 (1.1) | - | 2 (1.7) | |
| LVI, | 0.47 | |||
| Evident | 52 (28.9) | 20 (31.8) | 32 (27.3) | |
| Not evident | 125 (69.4) | 41 (65.0) | 84 (71.8) | |
| NA | 3 (1.7) | 2 (3.2) | 1 (0.9) | |
| PNI, | 0.87 | |||
| Present | 53 (29.4) | 17 (27.0) | 36 (30.7) | |
| Abstent | 120 (66.7) | 40 (63.5) | 80 (68.4) | |
| NA | 7 (3.9) | 6 (9.5) | 1 (0.9) | |
| Tumor grading, | 0.21 | |||
| 1 | 12 (6.7) | 3 (4.8) | 9 (7.7) | |
| 2 | 119 (66.1) | 47 (74.6) | 72 (61.5) | |
| 3 | 49 (27.2) | 13 (20.6) | 36 (30.8) | |
| ER positivity, % (median IQR) | 95 (90–95) | 95 (90–95) | 95 (90–95) |
|
| PgR positivity, % (median IQR) | 80 (40–90) | 90 (55–90) | 70 (30–90) |
|
| HER2, | 0.42 | |||
| 0 | 70 (38.9) | 22 (34.9) | 48 (41.0) | |
| 1–2 | 110 (61.1) | 41 (65.1) | 69 (59.0) | |
| Ki67, % (median IQR) | 25 (15–30) | 20 (15–28) | 25 (15–30) | 0.29 |
| RS (median IQR) | 16 (12–22) | 15 (11–18) | 17 (12–22) | 0.41 |
|
|
|
|
|
|---|---|---|---|
| Histology | |||
| NST | - | - | - |
| Lobular | –1.10 | –4.41 to 2.20 | 0.51 |
| Other | –1.36 | –5.79 to 3.08 | 0.55 |
| LVI | 0.10 | –2.68 to 2.89 | 0.94 |
| PNI | –0.69 | –3.42 to 2.05 | 0.62 |
| Grading | |||
| 1 | - | - | - |
| 2 | 3.10 | –1.86 to 8.06 | 0.22 |
| 3 | 6.70 | 1.43 to 11.97 |
|
| ER% | –0.29 | –0.54 to –0.04 |
|
| PgR% | –0.14 | –0.18 to –0.11 |
|
| HER2 | |||
| 0 | - | - | - |
| 1–2 | 1.08 | –1.47 to 3.63 | 0.41 |
| Ki67% | 0.28 | 0.15 to 0.40 |
|
|
|
| ||||||
|---|---|---|---|---|---|---|---|
|
|
|
|
|
|
|
|
|
| Histology | Histology | ||||||
| NST | - | - | - | NST | - | - | - |
| Lobular | 0.26 | –5.56 to 6.08 | 0.93 | Lobular | –1.78 | –5.87 to 2.31 | 0.39 |
| Other | –4.61 | –12.14 to 2.93 | 0.23 | Other | 0.03 | –5.53 to 5.59 | 0.99 |
| LVI | 1.52 | –2.94 to 5.97 | 0.50 | LVI | –0.62 | –4.23 to 2.99 | 0.73 |
| PNI | –1.09 | –5.52 to 3.33 | 0.62 | PNI | –0.52 | –4.01 to 2.97 | 0.77 |
| Grading | Grading | ||||||
| 1 | - | - | - | 1 | - | - | - |
| 2 | 1.11 | –78.25 to 10.46 | 0.81 | 2 | 4.06 | –1.95 to 10.10 | 0.184 |
| 3 | 6.08 | –3.98 to 16.14 | 0.23 | 3 | 6.89 | 0.55 to 13.22 |
|
| ER% | –0.41 | –0.71 to 0.10 |
| ER% | –0.24 | –0.69 to 0.21 | 0.30 |
| PgR% | –0.18 | –0.24 to –0.12 |
| PgR% | –0.14 | –0.18 to –0.09 |
|
| HER2 | HER2 | ||||||
| 0 | - | - | - | 0 | - | - | - |
| 1–2 | –1.66 | –5.93 to 2.54 | 0.43 | 1–2 | 2.59 | –0.63 to 5.82 | 0.11 |
| Ki67% | 0.26 | 0.05 to 0.47 |
| Ki67% | 0.28 | 0.13 to 0.44 |
|
|
|
| ||||||
|---|---|---|---|---|---|---|---|
|
|
|
|
|
|
|
|
|
| Histology | Histology | ||||||
| NST | - | - | - | NST | - | - | - |
| Lobular | 1.51 | 0.37 to 6.36 | 0.58 | Lobular | 1.00 | - | - |
| Other | 1.25 | 0.19 to 8.25 | 0.81 | Other | 0.59 | 0.07 to 5.05 | 0.63 |
| LVI | 0.67 | 0.21 to 2.10 | 0.49 | LVI | 0.77 | 0.20 to 2.98 | 0.70 |
| PNI | 0.69 | 0.20 to 2.36 | 0.56 | PNI | 0.64 | 0.16 to 2.47 | 0.51 |
| Grading | Grading | ||||||
| 1–2 | - | - | - | 1–2 | - | - | - |
| 3 | 1.66 | 0.48 to 5.74 | 0.42 | 3 | 1.47 | 0.45 to 4.86 | 0.53 |
| ER% | 0.93 | 0.85 to 1.02 | 0.11 | ER% | 1.02 | 0.86 to 1.21 | 0.81 |
| PgR% | 0.95 | 0.93 to 0.98 |
| PgR% | 0.95 | 0.93 to 0.98 |
|
| HER2 | HER2 | ||||||
| 0 | - | - | - | 0 | - | - | - |
| 1–2 | 0.75 | 0.26 to 2.18 | 0.60 | 1–2 | 2.54 | 0.66 to 9.78 | 0.18 |
| Ki67% | 1.06 | 0.10 to 1.12 | 0.061 | Ki67% | 1.08 | 1.01 to 1.16 |
|
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEndometrial and Cervical Cancer Treatments · Cancer Risks and Factors
Introduction
In recent years, multigene tests such as Oncotype DX, MammaPrint, Breast Cancer Index, Prosigna (PAM50), and EndoPredict have transformed the management of hormone-receptor positive (HR+)/human epidermal growth factor-receptor 2 negative (HER2–) early breast cancer (BC). These tools are used to refine risk stratification and assess the potential benefit of chemotherapy for individual patients [1].
Oncotype DX is a genomic test that analyzes the expression of 21 genes using quantitative real-time polymerase chain reaction (qRT-PCR) from paraffin-embedded tumor tissue samples. The test result is expressed as a recurrence score (RS), which ranges from 0 to 100 [2]. The prognostic and predictive value of Oncotype DX has been extensively validated in both retrospective and prospective studies. The TAILORx trial showed that patients with HR+/HER2– node negative BC and a RS between 0 and 25 do not benefit from adjuvant chemotherapy [3, 4]. An exploratory analysis of the study demonstrated that subjects aged 50 or younger with a RS between 16 and 25 may derive an additional benefit from chemotherapy compared to endocrine therapy alone [5]. The role of Oncotype DX in HR+/HER2– BC patients with 1–3 positive locoregional lymph nodes (i.e. pN1) has been explored in the prospective RxPONDER trial. According to this study, adjuvant chemotherapy does not add a significant benefit to endocrine therapy alone in post-menopausal women with RS < 26, regardless of the tumor clinico-pathological parameters. However, in pre-menopausal pN1 patients with RS < 26, adjuvant chemotherapy seems to reduce the rate of distant recurrence, supporting its use in this population [6].
Despite the established role of Oncotype DX in the management of HR+/HER2– early BC patients, several factors, such as its cost and turn-around time, fostered interest in developing algorithms for RS prediction based on clinical parameters and tumor biomarkers. Many of these parameters, such as the immunohistochemistry (IHC) expression of estrogen receptor (ER) and progesterone receptor (PgR), HER2 status, tumor stage, lymph node involvement, and Ki67%, are already widely recognized for their prognostic and predictive roles [7]. However, data supporting RS prediction based on these factors are still limited and inconsistent, and none of these variables have been analyzed according to patient menopausal status. Still, previous evidence suggests that menopausal status can influence gene expression patterns in normal and cancer breast tissue, and that this could eventually impact genomic test results, including RS [8].
This study aims to explore the relationship between histopathological features and RS in patients with early HR+/HER2– BC, with a particular focus on the influence of menopausal status.
Materials and methods
Study population
We retrospectively analyzed a cohort of patients with a histologically confirmed diagnosis of early-stage HR+/HER2– BC who received an Oncotype DX test after curative surgery. All patients were followed at Humanitas Istituto Clinico Catanese (HICC) in Catania, Italy, from September 2021 (when the Oncotype DX test was made freely available from the Italian National Health System) to March 2024. Fully anonymized data were extracted from DataBreast, a prospectively maintained European Society of BC Specialists (EUSOMA)-approved institutional database for quality assurance [9, 10]. Patient’s informed consent was obtained before performing data entry.
Pathological examination, including IHC stainings, was performed on tumor tissues in the Pathology Unit of HICC. Tumor sections from formalin-fixed, paraffin-embedded specimens were sent to Genomic Health laboratories (Exact Sciences) to perform the Oncotype DX test.
Relevant information was extracted from the database, including age, menopausal status, baseline tumor pathological features, i.e. tumor size (T), axillary nodal status (N), histotype, HR status (ER, PgR), Ki67 values, HER2 status, lymphovascular invasion (LVI), perineural invasion (PNI), and Oncotype DX RS value. Only patients with complete clinico-pathological data were included in the analysis.
Objectives
The primary aim of the study was to assess the association between traditional histopathological features and RS in patients with early-stage HR+/HER2– BC. Specifically, we examined how these variables influence RS values and contribute to risk stratification, with a focus on menopausal status.
Statistical analysis
Continuous variables were reported as medians with interquartile range (IQR), while binary and categorical variables were expressed as percentages. For descriptive statistics, t-test and chi-square have been used for continuous and categorical variables, respectively.
Linear regression analysis was performed to assess the association between RS as a continuous variable and histopathological characteristics to identify potential predictive factors.
Logistic regression analysis was performed separately for pre- and post-menopausal patients, dichotomizing RS according to thresholds of 16 and 25, respectively, to evaluate the association between clinico-pathological characteristics and the likelihood of obtaining an RS above or below the clinically relevant thresholds.
All statistical analyses were performed using STATA software v18.0 (StataCorp., 2023, College Station, TX: StataCorp LLC).
Results
Demographics
We identified 187 patients with early-stage HR+/HER2– BC who underwent Oncotype DX testing at HICC between September 2021 and March 2024. Of these, 180 were included in the analysis.
Detailed clinico-pathological characteristics are reported in Table 1. Median age in the overall population was 57.5 years (IQR 49–67.5). Sixty-three patients (35%) were pre-menopausal, and 117 (65%) were post-menopausal. The majority of tumors (n = 132, 73.3%) had a non-special type (NST) histology, were moderately differentiated (i.e. G2) (n = 119, 66.1%), with a median tumor size of 18 mm (IQR 12.5–23), a pT1 stage (n = 111, 61.7%) and without nodal involvement (pN0, n = 111, 61.7%). Median ER expression was 95% (IQR 90–95), and median PgR expression was 80% (IQR 40–90). Approximately 40% of the population (n = 70, 38.9%) had a HER2 0 disease, the remaining 61.1% (n = 110) had a HER2 low (i.e. 1+ or HER2 2+ with a negative FISH test) tumor. The median Ki67 proliferation index was 25% (IQR 15–30). LVI was reported in 28.9% of patients (n = 52), while PNI was detected in 29.4% of cases (n = 53). Median RS in the overall population was 16 (IQR 12–22).
No significant differences were observed between the pre- and post-menopausal patients, except for age, which was younger in pre-menopausal women. ER expression had a superimposable mean and IQR in the two groups, indicating an uneven distribution at extreme values (range min–max: 60–98% in pre-menopausal individuals; 80–100% in post-menopausal women). PgR levels were higher in the pre-menopausal group.
Median RS was slightly lower in pre-menopausal patients (median RS = 15, IQR 11–18) compared to post-menopausal subjects (median RS = 17, IQR 12–22), but this difference was not statistically significant. Among pre-menopausal women, 36.5% (n = 23) had an RS > 16, exceeding the threshold for high-risk definition. In the post-menopausal cohort, only 11.1% (n = 13) had a RS > 25, identifying them as high-risk (Figure 1).
Recurrence score (RS) distribution according to menopausal status, using the standard threshold for high-risk definition
Pathological features and RS
We performed linear regression analysis on the entire cohort to correlate RS, considered as a continuous variable, with several pathological variables (Table 2).
In the overall cohort, G3 [confidence interval (CI) 95%: 1.43–11.97; P = 0.01] and Ki67% (CI 95%: 0.15–0.40; P < 0.0001) had a significantly positive correlation with RS, while ER (CI 95%: –0.54 to –0.04; P = 0.03) and PgR expression (CI 95%: –0.18 to –0.11; P < 0.0001) displayed a significantly inverse association with RS.
When stratifying the population by menopausal status, some differences emerged (Table 3). In pre-menopausal women, RS remained significantly correlated with Ki67 (P = 0.02), ER (CI 95%: –0.71 to –0.10; P = 0.01), and PgR expression (CI 95%: –0.24 to –0.12; P < 0.0001). In the post-menopausal group, statistical significance persisted for G3 (CI 95%: 0.55–13.22; P = 0.03), Ki67 (CI 95%: 0.13–0.44; P = 0.001), and PgR expression (CI 95%: –0.18 to –0.09; P < 0.0001).
Next, we analyzed RS as a categorical variable, applying the standard high-risk thresholds (> 16 for pre-menopausal and > 25 for post-menopausal patients) (Table 4). PgR expression showed a significantly inverse correlation in both groups [odds ratio (OR) 0.95; 95% CI: 0.93–0.98; P = 0.001 in pre-menopausal patients; OR 0.95; 95% CI: 0.93–0.98; P < 0.0001 in post-menopausal women]. However, in post-menopausal women, Ki67% also displayed a significant correlation with RS > 25 (OR 1.08; 95% CI: 1.01–1.16; P = 0.031).
Since PgR expression was the only variable consistently showing a significantly inverse correlation across all analyses (both linear and logistic regression), we assessed its predictive performance using the area under the receiver operating characteristic (ROC) curve. In pre-menopausal patients, the area under the curve (AUC) was 0.75, whereas in post-menopausal patients, it was 0.87, indicating different predictive performances between the two groups (Figure 2).
Progesterone receptor (PgR) distribution according to recurrence score (RS) category in pre-menopausal (A) and post-menopausal (B) patients, and the area under receiver operating characteristic (ROC) curve for RS prediction based on PgR levels in pre-menopausal (C) and post-menopausal (D) patients
Discussion
Genomic tests, such as Oncotype DX, are widely used in clinical practice to assess the risk of recurrence in patients with early-stage HR+/HER2– BC [11, 12]. These tests assist therapeutic choices in the adjuvant setting by identifying individuals who can safely forgo chemotherapy, thus avoiding unnecessary and potentially toxic treatments [13]. Results from pivotal trials, such as TAILORx and RxPONDER, suggest that menopausal status should be taken into account when interpreting Oncotype DX results, since it has an impact on chemotherapy efficacy in HR+/HER2– BC [8].
Over the years, different studies explored pathological features that, alone or in combination, could surrogate RS in clinical practice [14–18]. However, none of these studies incorporated a subgroup analysis according to patient menopausal status.
We retrospectively evaluated a cohort of HR+/HER2– early BC patients treated at a single institution who underwent Oncotype DX for risk definition and adjuvant treatment decision-making, looking for pathological features correlated to RS in the overall population and in the pre- and post-menopausal subgroups.
In our cohort, clinical and pathological characteristics were superimposable in the two populations, with the only exception of ER and PgR expression levels, which were higher in pre-menopausal women. RS was also evenly distributed between pre- and post-menopausal patients, with a median value of 16 in the overall cohort, 15 in the pre- and 17 in the post-menopausal population. These results are in line with those by Carr et al. [19], who conducted a retrospective analysis on 575 HR+/HER2– early BC patients, finding higher ER levels in pre-menopausal compared to post-menopausal patients, but comparable RS values in the two groups.
We then applied different RS thresholds to identify high-risk individuals, according to menopausal status (i.e. RS > 16 and > 25 for pre- and post-menopausal women, respectively), showing that a larger proportion of patients in the pre-menopausal group presented a high risk of recurrence (36.5%) compared to post-menopausal women (11.1%). This result suggests that, although the optimal interpretation of RS in pre-menopausal women remains highly debated, younger patients diagnosed with HR+/HER2– BC are more likely to benefit from adjuvant chemotherapy [20].
According to the results of the RxPONDER trial, node positive pre-menopausal patients derive an invasive disease-free survival and distant recurrence-free survival benefit regardless of RS [6]. Hence, American Society of Clinical Oncology (ASCO) guidelines suggest avoiding offering Oncotype DX to pre-menopausal women with 1–3 positive nodes to guide decisions on adjuvant therapy [21]. Still, in clinical practice, the test is widely used even in this subgroup of patients as suggested by real world evidence [22], and as shown by our study, in which 33.3% of pre-menopausal women had pN1 disease, mostly due to the presence of a single positive node. The ongoing OFSET trial (NCT05879926) will clarify whether endocrine therapy plus ovarian function suppression (OFS) will yield comparable results to chemotherapy followed by endocrine therapy plus OFS in pre-menopausal patients with pN1 HR+/HER2– early BC and an RS of 0–25.
In our study, among the considered pathological parameters, tumor grading, Ki67, ER, and PgR displayed a significant correlation with RS, with some differences according to menopausal status.
Having G3 BC was associated with higher continuous RS values in the overall population and in the post-menopausal subgroup, but not in pre-menopausal patients. Additionally, no correlation emerged between grading and RS when considering the latter as a dichotomous outcome. Tumor grade is a known independent marker of BC aggressiveness, and it also emerged as a significant predictor of RS in several retrospective series [14, 15, 23]. Grading is also incorporated, along with patient age and tumor size, in the RSClin score, a tool developed to refine, rather than surrogate, Oncotype DX results [24].
In our analysis, the Ki67 proliferation index showed a direct association with continuous RS values, regardless of menopausal status. This correlation persisted only in post-menopausal women when RS was considered as a binary outcome. Like grading, Ki67—assessed by IHC—has also been associated with BC prognosis [25]. However, evidence of a direct correlation with RS is less straightforward. In a study by Patel et al. [26], no association emerged between Ki67 and RS in a retrospective cohort of 525 women. Additional evidence suggests only a moderate positive correlation between Ki67 and RS [27, 28]. Of note, the MKI67 gene, encoding for Ki67, is one of the proliferation-associated genes evaluated by Oncotype DX. However, a report by Selmani et al. [29] demonstrated a modest correlation between IHC assessment of Ki67 and Ki67 expression at the RNA level quantified with Oncotype DX. Other evidence suggests that Ki67 could be useful in surrogating RS, especially when combined with further pathological parameters [14, 30].
ER and PgR levels were negatively associated with RS in our study, with the latter displaying the strongest and most consistent results. The Oncotype DX assay quantifies both ER and PgR RNA, and several papers have investigated the concordance between protein and transcript expressions, finding an overall good agreement but a superior sensitivity for IHC [17, 31, 32].
In our cohort, using linear regression analysis, lower ER levels seem to predict higher RS values, especially in pre-menopausal patients. This correlation was lost in the post-menopausal subgroup after RS dichotomization. This result is in line with an exploratory analysis of the large phase III PlanB trial, where IHC ER expression had a weak negative correlation with RS [28]. Of note, in pre-menopausal women, ER expression at both mRNA and protein levels may fluctuate during different phases of the menstrual cycle, making their correlation with RS difficult to interpret [33–35]. However, clear evidence suggesting that the menstrual cycle phase can significantly influence RS is still lacking.
Among all the considered pathological features, PgR expression was the only parameter demonstrating a persistently significant negative correlation with RS, regardless of menopausal status, with better performance in the post-menopausal cohort according to a ROC analysis. PgR expression has a well-known prognostic role in BC, with lower levels predicting inferior outcomes. Several thresholds to discriminate between PgR-low and -high tumors have been proposed over time, with inconsistent results thus far [36, 37]. Stratifying our population according to PgR levels < 10 or > 10, we obtained a significant inverse correlation with RS (data not shown), even though the small number of patients in each subgroup did not allow us to draw definitive conclusions. In general, our results are in line with pre-existing literature demonstrating that PgR is a valid surrogate for RS, either alone or combined with other variables [15, 16, 30, 38].
Our study presents some limitations. Firstly, our cohort is not large enough to fully generalize the results to all patients with HR+/HER2– early BC. This is especially true for the pre-menopausal cohort, which comprised only 63 patients. Additionally, being a retrospective analysis, the available information is based on pre-existing clinical data, which could introduce selection bias. In this context, the definition of menopausal status, as self-reported by patients, could be heavily biased. This limitation has been extensively discussed for large randomized trials, such as TAILORx and RxPONDER [8]. Over time, more precise and robust methods to define menopausal status have been investigated, including measurement of the anti-Mullerian hormone, but their application in clinical practice is still limited [39]. IHC evaluation could also be biased in the context of a retrospective analysis, due to the subjectivity of the assessment. However, all the evaluations in our study have been performed at a single institution, minimizing the risk of inter-observer variability. Another significant shortcoming of our work is the lack of long-term follow-up, which prevents us from definitively assessing the predictive ability of Oncotype DX for recurrence.
Taking into account these inherent limitations, our findings suggest that risk stratification based on clinical-pathological factors, such as tumor grade, Ki67, ER, and PgR, could be useful in personalizing treatment according to patient menopausal status. The ability of these clinical parameters to predict the RS could support the choice of the test, guiding physicians to select patients who will benefit most from a molecular evaluation. Further prospective studies with longer follow-up and a larger cohort are needed to further validate these results and improve the accuracy of risk stratification for women with HR+/HER2– early BC. In this context, a significant effort should be made to generate results that may help to refine treatment and follow-up indications according to the menopausal status of these patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bottosso M Miglietta F Vernaci GM Giarratano T Dieci MV Guarneri V et al. Gene Expression Assays to Tailor Adjuvant Endocrine Therapy for HR+/HER 2– Breast Cancer Clin Cancer Res 20243028849410.1158/1078-0432.CCR-23-402038656833 PMC 11247313 · doi ↗ · pubmed ↗
- 2Sparano JA Gray RJ Makower DF Pritchard KI Albain KS Hayes DF et al. Prospective Validation of a 21-Gene Expression Assay in Breast Cancer N Engl J Med 201537320051410.1056/NEJ Moa 151076426412349 PMC 4701034 · doi ↗ · pubmed ↗
- 3Fisher B Dignam J Bryant J Wolmark N Five versus more than five years of tamoxifen for lymph node-negative breast cancer: updated findings from the National Surgical Adjuvant Breast and Bowel Project B-14 randomized trial J Natl Cancer Inst 2001936849010.1093/jnci/93.9.68411333290 · doi ↗ · pubmed ↗
- 4Paik S Shak S Tang G Kim C Baker J Cronin M et al. A multigene assay to predict recurrence of tamoxifen-treated, node-negative breast cancer N Engl J Med 200435128172610.1056/NEJ Moa 04158815591335 · doi ↗ · pubmed ↗
- 5Sparano JA Gray RJ Makower DF Pritchard KI Albain KS Hayes DF et al. Adjuvant Chemotherapy Guided by a 21-Gene Expression Assay in Breast Cancer N Engl J Med 20183791112110.1056/NEJ Moa 180471029860917 PMC 6172658 · doi ↗ · pubmed ↗
- 6Kalinsky K Barlow WE Gralow JR Meric-Bernstam F Albain KS Hayes DF et al. 21-Gene Assay to Inform Chemotherapy Benefit in Node-Positive Breast Cancer N Engl J Med 202138523364710.1056/NEJ Moa 210887334914339 PMC 9096864 · doi ↗ · pubmed ↗
- 7Allison KH Kandalaft PL Sitlani CM Dintzis SM Gown AM Routine pathologic parameters can predict Oncotype DX recurrence scores in subsets of ER positive patients: who does not always need testing?Breast Cancer Res Treat 20121314132410.1007/s 10549-011-1416-321369717 · doi ↗ · pubmed ↗
- 8Zhang S Fitzsimmons KC Hurvitz SA Oncotype DX Recurrence Score in premenopausal women Ther Adv Med Oncol 2022141758835922108107710.1177/1758835922108107735295864 PMC 8918761 · doi ↗ · pubmed ↗