Racial Differences in Care Quality Among Men With Newly Diagnosed Prostate Cancer
Dawson C. Hill, Samuel R. Kaufman, Christopher Dall, Paula Guro, Sarah Leick, Preeti Chachlani, Xiu Liu, Addison Shay, Mary Oerline, Rishi R. Sekar, Lindsey A. Herrel, Brent K. Hollenbeck, Vahakn B. Shahinian, Arnav Srivastava

TL;DR
The study explores differences in the quality of prostate cancer care received by men of different races in the Medicare system.
Contribution
The novelty lies in analyzing racial disparities in confirmatory testing and treatment among newly diagnosed prostate cancer patients.
Findings
Racial disparities in care quality were identified among Medicare beneficiaries with newly diagnosed prostate cancer.
The study highlights variations in confirmatory testing and potential overtreatment based on race.
Abstract
This cross-sectional study examines racial disparities in care quality, including confirmatory testing and potential overtreatment, among Medicare beneficiaries with newly diagnosed prostate cancer.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure
Figure| Characteristic | Men initiating active surveillance | Unhealthy men at risk of overtreatment | ||||||
|---|---|---|---|---|---|---|---|---|
| No. (%) | No. (%) | |||||||
| Black | White | Other | Black | White | Other | |||
| No. | 568 | 6804 | 679 | NA | 571 | 4173 | 346 | NA |
| Age, mean (SD), y | 69.5 (2.4) | 69.8 (2.5) | 69.1 (2.3) | <.001 | 79.9 (5.0) | 82.0 (4.9) | 76.9 (7.2) | <.001 |
| CCI score | ||||||||
| 0 | 303 (53.3) | 4757 (69.9) | 463 (68.2) | <.001 | 27 (4.7) | 317 (7.6) | 127 (36.7) | <.001 |
| 1 | 147 (25.9) | 1252 (18.4) | 122 (18.0) | 67 (11.7) | 538 (12.9) | 55 (15.9) | ||
| 2 | 118 (20.8) | 795 (11.7) | 94 (13.8) | 92 (16.1) | 826 (19.8) | 43 (12.4) | ||
| ≥3 | NA | NA | NA | 385 (67.4) | 2492 (59.7) | 121 (35.0) | ||
| SES, tertile | ||||||||
| 1 | 279 (49.1) | 1737 (25.5) | 126 (18.6) | <.001 | 342 (59.9) | 1578 (37.8) | 67 (19.4) | <.001 |
| 2 | 176 (31.0) | 2450 (36.0) | 215 (31.7) | 153 (26.8) | 1514 (36.3) | 242 (69.9) | ||
| 3 | 113 (19.9) | 2617 (38.5) | 338 (49.8) | 76 (13.3) | 1081 (25.9) | 37 (10.7) | ||
| Rurality | ||||||||
| City | 324 (57.0) | 3122 (45.9) | 381 (58.2) | <.001 | 345 (60.4) | 1763 (42.2) | 76 (57.1) | <.001 |
| Metro county | 166 (29.2) | 2278 (33.5) | 183 (27.9) | 144 (25.2) | 1470 (35.2) | 39 (29.3) | ||
| Near metro area or rural | 78 (13.7) | 1404 (20.6) | 91 (13.4) | 82 (14.4) | 940 (22.5) | 18 (5.2) | ||
| Diagnosis year | ||||||||
| 2014 | 71 (12.5) | 782 (11.5) | 46 (6.8) | <.001 | 82 (14.4) | 541 (13.0) | 37 (10.7) | .24 |
| 2015 | 82 (14.4) | 977 (14.4) | 73 (10.8) | 70 (12.3) | 591 (14.2) | 38 (11.0) | ||
| 2016 | 79 (13.9) | 1093 (16.1) | 99 (14.6) | 97 (17.0) | 692 (16.6) | 63 (18.2) | ||
| 2017 | 103 (18.1) | 1260 (18.5) | 137 (20.2) | 100 (17.5) | 711 (17.0) | 52 (15.0) | ||
| 2018 | 104 (18.3) | 1336 (19.6) | 163 (24.0) | 109 (19.1) | 782 (18.7) | 85 (24.6) | ||
| 2019 | 129 (22.7) | 1356 (19.9) | 161 (23.7) | 113 (19.8) | 856 (20.5) | 71 (20.5) | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsProstate Cancer Diagnosis and Treatment · Global Cancer Incidence and Screening · Economic and Financial Impacts of Cancer
Introduction
Black men with prostate cancer have historically had lower health care utilization, which is believed to contribute to their higher observed mortality rates.^1,2^ However, the relationship between health care utilization and quality of prostate cancer care is nuanced. Confirmatory testing among younger, healthy men electing for active surveillance to detect occult high-grade disease is guideline-concordant care and an example of alignment between utilization and quality.^3^ Conversely, in older, unhealthy men, utilization manifesting as immediate treatment (ie, potential overtreatment) often represents poor quality.^3^ In this scenario, treatment typically offers little oncologic benefit while posing substantial toxic effects. We examined racial differences in confirmatory testing and potential overtreatment—2 measures of quality with opposing relationships to health care utilization—in men with newly diagnosed prostate cancer.
Methods
The University of Michigan Institutional Review Board deemed this study exempt because patient data were deidentified. We followed the STROBE reporting guidelines.
Using a 20% sample of traditional Medicare beneficiaries, we identified 54 979 men with newly diagnosed prostate cancer between 2014 and 2019 (analyzed in 2024). We created 2 separate study cohorts: men initiating active surveillance and unhealthy men at risk of overtreatment (eMethods in Supplement 1). The first outcome, confirmatory testing (ie, repeat prostate biopsy, magnetic resonance imaging before or after diagnosis, or genomics test within 12 months of diagnosis), was assessed among men initiating active surveillance.^4^ The second outcome, potential overtreatment, was assessed among unhealthy men (ie, those with >50% predicted noncancer mortality risk within 5 years of diagnosis). These men are highly unlikely to benefit from treatment (ie, surgery or radiation therapy) due to their competing health risks.^5^
Race, categorized using the Research Triangle Institute race code in the Medicare enrollment file (ie, Black, White, and other [not further specified]), was our main exposure. This designation demonstrates excellent agreement with self-reported Black race but might not fully capture its nature as a social construct.^2,6^ For patients categorized as other, further granularity about race was not available in the data. Adjusted odd ratios (aORs) were calculated using multilevel logistic regressions to evaluate the association between race and both outcomes (confirmatory testing and potential overtreatment), adjusting for age, socioeconomic status, Charlson Comorbidity Index score, rurality, and diagnosis year. From these models, we derived adjusted percentages for each outcome by race. Analyses were performed using Stata, version 18 (StataCorp LLC), with a 2-sided P < .05 considered significant.
Results
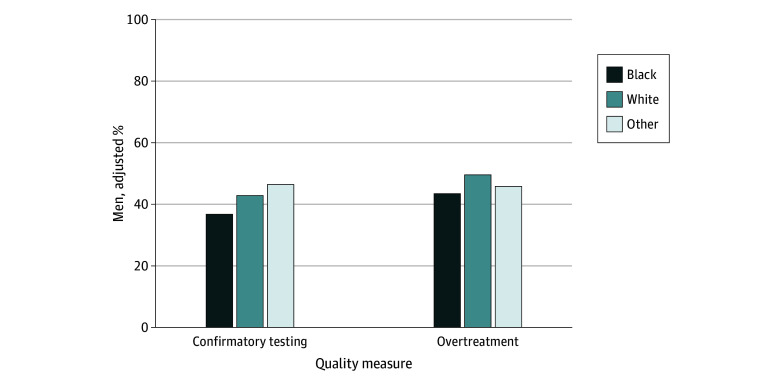
Of 8051 men electing for active surveillance and 5090 unhealthy men at risk of overtreatment, 568 (7.1%) and 571 (11.2%) were Black, respectively (Table). Among men initiating active surveillance, Black race was associated with lower odds of undergoing confirmatory testing within 12 months of diagnosis compared with White race (aOR, 0.75; 95% CI, 0.62-0.92; P = .01). This finding translated to a 6.1% (95% CI, 1.9%-10.3%) decrease in confirmatory testing completion (Figure). Among unhealthy men at risk of overtreatment, Black race was associated with lower odds of overtreatment (aOR, 0.86; 95% CI, 0.77-0.97; P = .01) compared with White race. Overtreatment was less common in Black men compared with White men (adjusted difference, 6.1%; 95% CI, 1.8%-10.4%).
Adjusted Percentages of Quality Measure Adherence by RaceAdjusted percentage for confirmatory testing for Black men statistically different than White men (P < .05). Adjusted percentage for overtreatment for Black and other men statistically different than White men (P < .05). Percentages were adjusted for socioeconomic status (tertiles), Charlson Comorbidity Index score, patient age, rurality, and diagnosis year. For patients categorized as other, further granularity about race was not available in the data.
Discussion
Among men with traditional Medicare, we examined racial differences in 2 important measures of prostate cancer care quality that have contrasting relationships with utilization. Black men had lower odds of confirmatory testing among those on active surveillance, where utilization and quality are tightly aligned, indicating worse care. Conversely, Black men had lower odds of overtreatment, where utilization and quality are misaligned, suggesting better care in this dimension. Study limitations include the lack of cancer risk characteristics in Medicare claims, hindering our ability to classify appropriateness of management, and the smaller sample of Black men. Further, our use of a race variable might not fully address structural inequities faced by minority communities. Our study highlights the importance of understanding the nuanced relationship between utilization and prostate cancer care quality when trying to improve care for underserved communities.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dieleman JL, Chen C, Crosby SW, . US health care spending by race and ethnicity, 2002-2016. JAMA. 2021;326(7):649-659. doi:10.1001/jama.2021.9937 34402829 PMC 8371574 · doi ↗ · pubmed ↗
- 2Dee EC, Todd R, Ng K, . Racial disparities in prostate cancer in the UK and the USA: similarities, differences and steps forwards. Nat Rev Urol. 2025;22(4):223-234. doi:10.1038/s 41585-024-00948-x 39424981 · doi ↗ · pubmed ↗
- 3Schaeffer EM, Srinivas S, Adra N, . Prostate cancer, version 4.2023, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2023;21(10):1067-1096. doi:10.6004/jnccn.2023.0050 37856213 · doi ↗ · pubmed ↗
- 4Modi PK, Kaufman SR, Qi J, . National trends in active surveillance for prostate cancer: validation of Medicare claims-based algorithms. Urology. 2018;120:96-102. doi:10.1016/j.urology.2018.06.037 29990573 PMC 6462187 · doi ↗ · pubmed ↗
- 5Maganty A, Kaufman SR, Oerline MK, . National trends in management of newly diagnosed prostate cancer. Clin Genitourin Cancer. 2024;22(2):10-17. doi:10.1016/j.clgc.2023.07.001 37468340 · doi ↗ · pubmed ↗
- 6Vince RA Jr, Eyrich NW, Mahal BA, Stensland K, Schaeffer EM, Spratt DE. Reporting of racial health disparities research: are we making progress? J Clin Oncol. 2022;40(1):8-11. doi:10.1200/JCO.21.01780 34694897 PMC 8683227 · doi ↗ · pubmed ↗