“What Matters” to Community-Dwelling Older Adults With Dementia and Their Family Caregivers: A Qualitative Pilot Study
Huey-Ming Tzeng, Yong-Fang Kuo, Monique R. Pappadis, Elizabeth A. Hennessy, Maribel M. Marquez-Bhojani, Samuel V. David, Demetress Harrell, Mukaila A. Raji

TL;DR
This study explores what matters most to older adults with dementia and their caregivers during annual wellness visits and how these priorities align with a healthcare framework.
Contribution
This is the first study to map health goals and worries of dementia patients and caregivers to the IHI-4Ms framework in the context of annual wellness visits.
Findings
Three overarching goal themes were identified: physical/mental health maintenance, cognitive maintenance, and independence.
Six worry themes included cognitive decline, behavioral changes, and loss of independence due to health decline.
Goals and worries were mapped to the IHI-4Ms framework, suggesting potential for addressing them during annual wellness visits.
Abstract
Drawing on the Institute of Healthcare Improvement (IHI)’s 4Ms framework of an Age-Friendly Health System in primary care to incorporate “What Matters,” mentation, mobility, and medication, this qualitative/interview pilot study listened to “What Matters” most to community-dwelling Medicare beneficiaries with dementia and family caregivers in the context of Annual Wellness Visit (AWV). We then mapped identified “What Matters” themes (health goals and worries) to IHI-4Ms. Twenty-four caregivers and two patients participated in a one-time phone/Zoom interview. We observed three overarching goal themes (physical/mental health maintenance, cognitive maintenance, and independence) and six overarching worry themes (cognitive decline, behavioral changes, health decline leading to loss of independence, mobility issues, dehydration, and caregivers’ financial responsibility). The identified goals…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1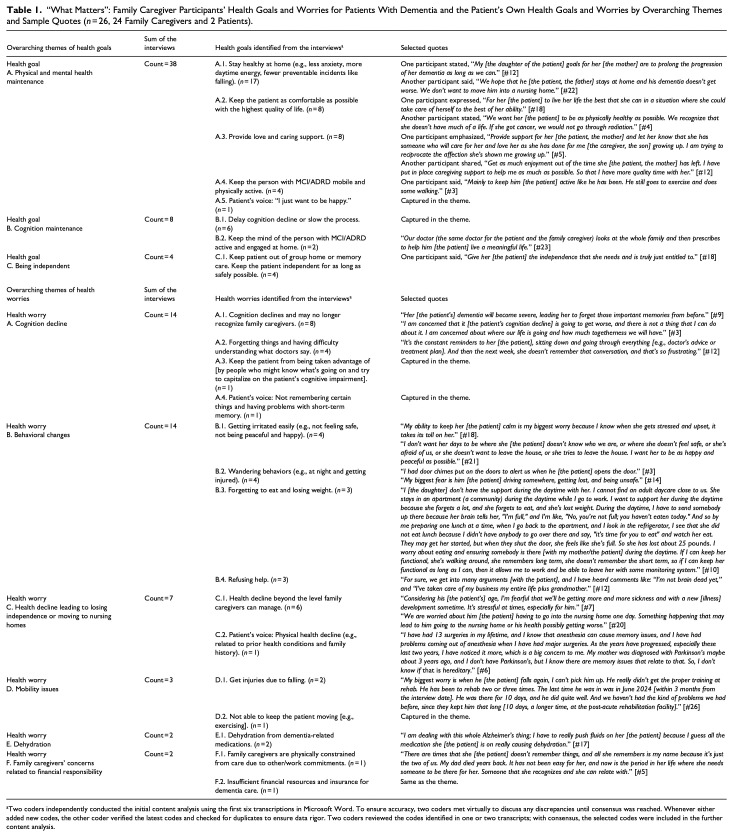 Figure 2
Figure 2- —National Institute on Aginghttps://doi.org/10.13039/100000049
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGeriatric Care and Nursing Homes · Dementia and Cognitive Impairment Research · Health disparities and outcomes
Introduction
The Centers for Medicare and Medicaid Services (CMS) has offered free Annual Wellness Visits (AWVs) to U.S. Medicare beneficiaries aged 65 years and older since 2011 (Morgan et al., 2021). AWVs’ impact on care quality for those with mild cognitive impairment (MCI) or Alzheimer’s Disease and Related Dementias (ADRD) remains a critical policy and practice gap. Those patients/caregivers often rely on primary care services to address “What matters” most regarding care needs (e.g., priorities/needs important to patients with MCI/ADRD and disease experience (DiBenedetti et al., 2020; Hauber et al., 2023)). The Institute for Healthcare Improvement’s (IHI, 2022) advocates for incorporating its 4Ms framework of an Age-Friendly Health System into primary care practices: “What Matters,” mentation, mobility, and medication. The present study focuses on the connection between AWVs for patients with MCI/ADRD and IHI’s 4Ms framework in primary care practices.
AWVs include cognition and risk assessment, medication reconciliation, advance care planning consultation, and review and development of personalized prevention plans (Centers for Medicare and Medicaid Services Medicare Learning Network, 2025). AWVs were associated with reducing the risks of falls/fractures (Tzeng et al. (2022) and the timely detection of cognitive impairment (Tzeng et al. (2024). Optimal dementia care should reflect “What Matters” most to community-dwelling patients with MCI/ADRD and their family caregivers (Downer, Al Snih et al., 2021; Downer, Chou et al., 2021; Gozalo et al., 2011; Knox et al., 2021; Kuo et al., 2009; Liss et al., 2021; Mitchell, 2015; Nguyen et al., 2020; Shepard et al., 2021, 2023). Thus, AWVs could represent the ideal healthcare encounters for incorporating “What Matters” into wellness and preventive service conversations.
Bogardus et al. (1998) developed a taxonomy for classifying goals for patients with dementia. This taxonomy includes four axes: goal domain, specificity, timeframe, and challenge. They identified three overarching goal domains: functioning, psychosocial, and medical care matters. These researchers found that patients and family caregivers often require assistance in setting specific and achievable goals; the different goals for the same patient reflect the roles and skills that people bring to support the patient’s care and include disagreements among family caregivers of the same patient. Naik and Walling (2022) urged clinicians to document the goals of care conversations with patients (veterans without cognitive impairment) throughout the care journey to include health values (e.g., managing health concerning the balance between quality and quantity of life), objective and measurable health outcome goals, and care preferences to achieve outcome goals. Another study conducted by Simpson et al. (2021) explored factors contributing to the realization of health promotion recommendations that Medicare beneficiaries (without cognitive impairment) received during the most recent AWV. Seven health-promotion-realizing factors were identified: (1) preserving mental health, (2) stress (preventing beneficiaries from practicing health promotion recommendations), (3) ongoing social support, (4) environment-supporting physical activities, (5) recent abnormal lab/assessment values, (6) reminders of practicing health promotion behaviors, and (7) community resources to ease health care access barriers. However, they found that AWV documentation did not reflect the aforementioned factors for most participants. These researchers emphasized the need to personalize AWV recommendations and strategies to provide ongoing support to older adults between AWV visits.
Since no studies have used the 4Ms framework to bridge AWV components and “What Matters” to Medicare beneficiaries with MCI/ADRD and their family caregivers, three of our co-authors first mapped the required AWV components to IHI’s four 4Ms components and the six key actions related to the 4Ms framework that IHI urges ambulatory care settings to perform at least annually for each patient (IHI, 2022; Supplemental eTable S1). We found that AWV components failed to prioritize documenting “What Matters” to community-dwelling patients/caregivers as a gap in practice. “What Matters” (i.e., health-related goals or worries) interweaves with the other three 4Ms components and may require health maintenance/care interventions associated with mentation, mobility, and medication.
Purpose of the Study
This descriptive qualitative interview pilot study aimed to identify the themes of “What Matters” most to their health (i.e., goals and worries) as reported by Medicare beneficiaries with MCI/ADRD and their family caregivers in the context of Medicare’s AWVs. We then mapped the identified “What Matters” themes (health goals and worries) from respondents to IHI’s mentation, mobility, and medication components related to the 4Ms framework of an Age-Friendly Health System (IHI, 2022).
Methods
Design and Data Source
We conducted this qualitative study using phone or Zoom video conferencing interviews to gather opinions from current family caregivers and patients with MCI/ADRD. We used convenience sampling to recruit participants into a one-time, one-on-one, semi-structured interview.
The University of Texas Medical Branch (UTMB) Institutional Review Board determined that this study met the federal regulations of a Quality Assessment/Quality Improvement project. All participants verbally agreed to participate in recorded interviews. We followed the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines (Tong et al., 2007).
Sample
The pilot study used convenience sampling of Medicare beneficiaries with MCI/ADRD and their family caregivers residing in Texas. We aimed to interview 25 participants; we completed 26 interviews. Family caregivers had to be ≥21 years old at the interview; currently caring for a person ≥65 years on Medicare with an MCI/ADRD diagnosis; and have attended at least one AWV within the past 12 months. Patient participants had to be independent enough to care for themselves, told by a healthcare provider they had MCI/ADRD, be ≥65 years, on Medicare, not living in a long-term nursing home, and have attended at least one AWV within the past 12 months. Participants must speak English or Spanish and be interviewed via telephone or videoconferencing/Zoom.
Recruitment efforts included posts on social media, emails, local community events, an adult day care program, one local geriatric clinic, and word of mouth; we did not do any cold calls. Two English-speaking nurse interviewers and one English-Spanish bilingual interviewer were trained by the first author and coached throughout the data collection period (November 2023‒September 2024) to ensure consistency across interviewers. Participants verbally agreed to participate during screening and again before the interview. Interviews lasted 20‒120 min (average = 30 min); we recorded the interviews. Post-interview, participants received a $25 gift card.
Measures
We conducted interviews using a semi-structured topic guide based on the study purpose and IHI’s 4Ms framework (open and multi-choice questions, refined through community stakeholders’ insights). The guide included seven interview questions and 12 demographic characteristics (Supplemental eFigure S1 and eTable S2). The main interview questions analyzed in this paper were Q1 and Q2 (health-related goals and worries for the patient with MCI/ADRD).
Analyses
The first author trained three interviewers and coached them throughout the data collection period to ensure consistency across interviewers. All interviews were transcribed manually by a third-party vendor in verbatim form. Two coders independently conducted initial descriptive inductive content analysis (using an inductive thematic coding process) of the first six transcriptions in Microsoft Word. Two coders discussed and agreed on the initial coding through consensus and applied the initial coding to the remaining transcripts. Both coders verified new codes and checked for duplicates (the agreement level was 97.2% between two coders for all open questions in the semi-structured interview guide; 98.4% for the responses to the interview questions analyzed in this present study). We used Microsoft Word in the coding process and IBM SPSS (IBM Corp, 2021) for organizing the identified themes. Then, two coders performed descriptive inductive content analysis on the identified codes to identify major themes using Microsoft Word. Two coders met via Zoom to compare their analyses and resolve any disagreements on the final themes. An interpretation meeting of the senior research team (three of the co-authors) refined and agreed upon the final themes. Then, the first author mapped the identified “What Matters” themes with IHI’s four 4Ms components and IHI’s six key actions. Another interpretation meeting of the senior research team (three of the co-authors) refined the mapping of the identified “What Matters” themes with IHI’s four 4Ms components and IHI’s six key actions. Descriptive analyses on the coded transcripts and themes were generated using IBM SPSS (IBM Corp, 2021).
Results
Supplemental eTable S2, eTable S3, and eFigure S2 profile the 24 caregivers (18 female, 6 Hispanic, 12 White, 10 Black) and the two patients (both female, one Hispanic, one White).
Themes for Health-Related Goals and Worries
We identified eight goals (Table 1 with selected quotes). The top three goal themes in frequencies were: (1) Stay healthy at home (n = 17, 65%); (2) Keep the patient as comfortable as possible with the highest quality of life (n = 8, 31%); and (3) Provide love and caring support (n = 8, 31%). We then grouped these eight goals into three overarching themes: physical and mental health maintenance, cognitive maintenance, and independence.
Table 1.: “What Matters”: Family Caregiver Participants’ Health Goals and Worries for Patients With Dementia and the Patient’s Own Health Goals and Worries by Overarching Themes and Sample Quotes (n = 26, 24 Family Caregivers and 2 Patients).
We identified 15 worries (Table 1 with selected quotes). The top 5 worry themes in frequencies were: (1) Cognition decline and may no longer recognize family caregivers (n = 8, 31%); (2) Health decline beyond the level family caregivers can manage (n = 6, 23%); (3) Forgetting things and having difficulty understanding what doctors say (n = 4, 15%); (4) Getting irritated easily (n = 4, 15%); and (5) Wandering behaviors (n = 4, 15%). We grouped these 15 worries into six overarching themes: cognition decline, behavioral changes, health decline leading to losing independence or moving to nursing homes, mobility issues, dehydration, and family caregivers’ worry related to financial responsibility.
IHI Mapping With Identified Health-Related Goals and Worries
We mapped the eight identified goals (Q1; Supplemental eTable S4) to at least one of the IHI’s mentation, mobility, and medication components. The 15 identified worries (Q2; Supplemental eTable S4) were mapped to at least one of the IHI’s mentation, mobility, and medication components. Two worries were related to a family caregiver’s financial responsibility, and these two worries were mapped to IHI’s mentation component in Supplemental eTAble S4. Financial responsibility can impact access to or realization of health promotion recommendations related to patients’ mental health (mentation), mobility, and medication. Here, the mentation component in 4Ms is expanded also to include psychosocial issues, such as financial concerns.
Discussion
This qualitative interview pilot study describes the themes of “What Matters” most to the health of Medicare beneficiaries with MCI/ADRD and their family caregivers. The identified “What Matters” themes (health goals and worries) from respondents were mapped to at least one of the IHI’s mentation, mobility, and medication components, suggesting the potential to be addressed through AWVs. Thus, many of the identified health goal/worry themes are not specific, realistic, or actionable; this observation could be due to a one-time interview using two open-ended interview questions to solicit insights via phone or Zoom (i.e., What are your goals for (name of the patient with dementia) health? What are your worries for (name of the patient with dementia) health?) as a study limitation. IHI (2022) recommended using previously validated questions or tools (e.g., functional status assessment) that are appropriate to patient factors (e.g., language and cultural background) to help patients and family caregivers express their health outcomes goals and care preferences. Naik and Walling (2022) emphasized that the goals of care conversations with patients (including advance care planning) are a progressive back-and-forth of health values, care preferences, and prognostic awareness, which may ultimately result in specific, realistic, and actionable outcome goals. The process of considering “What Matters” to patients from both their and their caregivers’ viewpoints is essential for primary care providers to align dementia care according to “What Matters” to each older adult with MCI/ADRD (Bogardus et al., 1998; IHI, 2022).
With only two patient participants with MCI/ADRD in this study, we were unable to draw meaningful conclusions from patients’ viewpoints. Similar to the findings of the study by Bogardus et al. (1998), the health goals expressed by the two persons with MCI/ADRD were non-specific. When family caregivers identified the goals and worries of persons with MCI/ADRD, the things labeled as “What Matters” most to the persons with MCI/ADRD appeared to be the things that mattered most to the family caregivers. Soliciting “What Matters” most to family caregivers of persons with MCI/ADRD is important and valuable, especially to support caregiving for community-dwelling persons with MCI/ADRD. “What Matters” most to the family caregiver is frequently misaligned with “What Matters” most to the patient with MCI/ADRD. Similarly, “What Matters” most to the clinicians or case managers is misaligned with “What Matters” most to the patient with MCI/ADRD (Bogardus et al., 1998).
In this study, with only two participants with MCI/ADRD, the overarching “What Matters” to patients with MCI/ADRD in the context of AWVs reflected the needs related to supporting caregivers at home and the emotional burden on caregivers. We learned that health goals centered on keeping patients comfortable at home and delaying the need to move to a nursing home. Health-related worries reflected the challenges of home-based caregiving and the grief about seeing loved ones with MCI/ADRD lose important memories, affection for family caregivers, emotional stability, and ability to care for themselves.
We observed that the health goals and worries identified in the present study (2 older adults with MCI/ADRD and 24 active family caregivers of older adults with MCI/ADRD) approximately mapped to the three broad goal domains (functional, psychosocial, and medical concerns) in the study (older adults with MCI/ADRD, family caregivers and healthcare providers) conducted by Bogardus et al. (1998), the health values in the study (older adults without MCI/ADRD) conducted by Naik and Walling (2022), and the health promotion-realizing factors (i.e., facilitators or barriers) identified in the study (older adults without MCI/ADRD) performed by Simpson et al. (2021). It appears that “What Matters” to patients, including health goals, worries, and health values, as well as facilitators and barriers to realizing wellness recommendations from AWVs, are similar terms that all lead to identifying practical directions for older adults with or without MCI/ADRD to live as fully as possible.
Limitations
This pilot combined lessons learned from family caregivers and patients as appropriate. Information abstracted from the two patient interviews was limited, which is consistent with the study conducted by Bogardus et al. (1998). This study was small, with a sample of 26 Texas-based participants from a single geographic area. Thus, generalizability is limited, and conveying the findings to other contexts, study participants, or other clinical and non-clinical settings should be done with caution.
Future Research Directions
The valuable information gained from this study suggests a practice gap in assisting older adults with MCI/ADRD and their caregivers in setting specific health goals and addressing concerns over their dementia care journey. This practice gap could lead to misalignment between care preferences related to health goals and worries and healthcare providers’ recommendations provided during AWVs and other maintenance visits. The lessons learned from mapping “What Matters” themes (health goals and worries) for patients with MCI/ADRD with IHI’s (IHI, 2022) mentation-mobility-medication components within the 4M framework of an Age-Friendly Health System underscore the potential need for practical health policy considerations to support dementia-friendly AWVs.
The findings of this Texas-based pilot study also will support a national family caregiver interview study using inductive content analysis for diverse populations. Future qualitative or mixed-methods studies should assess the role of social determinants of health and social identities of patients with MCI/ADRD and their family caregivers in “What Matters” most to their health during AWVs. In addition, future research should explore strategies (e.g., engaging the patient in expressing his or her activity preferences through showing pictures of gardening or baking) to identify “What Matters” most to the patient with MCI/ADRD and align the patient’s preferences with “What Matters” most to the family caregivers of the same patient. Eliciting “What Matters” most to family caregivers of the patients with MCI/ADRD is important and valuable as the dementia progresses. Healthcare providers should anticipate disagreements among family caregivers and resolve them with the best interest of the patient at heart.
Conclusions and Policy Implications
Our study is the first to seek to understand “What Matters” to Medicare beneficiaries with MCI/ADRD or their caregivers in the context of AWVs and to map the identified “What Matters” themes (health goals and worries) with IHI’s mentation, mobility, and medication components related to the 4Ms framework of an Age-Friendly Health System (IHI, 2022). The identified “What Matters” themes were mapped to at least one of the IHI’s mentation, mobility, and medication components, indicating the potential for addressing these through AWVs. The valuable lessons learned in this study underscore the potential need for practical health policy considerations to support dementia-friendly AWVs so that “What Matters” to patients with MCI/ADRD and “What Matters” to their family caregivers can be heard and discussed during AWVs.
Supplemental Material
sj-docx-1-ggm-10.1177_30495334251358620 – Supplemental material for “What Matters” to Community-Dwelling Older Adults With Dementia and Their Family Caregivers: A Qualitative Pilot StudySupplemental material, sj-docx-1-ggm-10.1177_30495334251358620 for “What Matters” to Community-Dwelling Older Adults With Dementia and Their Family Caregivers: A Qualitative Pilot Study by Huey-Ming Tzeng, Yong-Fang Kuo, Monique R. Pappadis, Elizabeth A. Hennessy, Maribel M. Marquez-Bhojani, Samuel V. David, Demetress Harrell and Mukaila A. Raji in Sage Open Aging
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bogardus S. T. Bradley E. H. Tinetti M. E. (1998). A taxonomy for goal setting in the care of persons with dementia. Journal of General Internal Medicine, 13(10), 675–680. 10.1046/j.1525-1497.1998.00203.x 9798814 PMC 1500896 · doi ↗ · pubmed ↗
- 2Centers for Medicare and Medicaid Services Medicare Learning Network. (2025). Medicare wellness visits: Annual wellness visit health risk assessment. https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLN Products/preventive-services/medicare-wellness-visits.html#AWV
- 3Di Benedetti D. B. Slota C. Wronski S. L. Vradenburg G. Comer M. Callahan L. F. Winfield J. Rubino I. Krasa H. B. Hartry A. Wieberg D. Kremer I. N. Lappin D. Martin A. D. Frangiosa T. Biggar V. Hauber B. (2020). Assessing what matters most to patients with or at risk for Alzheimer’s and care partners: A qualitative study evaluating symptoms, impacts, and outcomes. Alzheimer s Research & Therapy, 12(1), 90. 10.1186/s 13195-020-00659-6PMC 739391632731886 · doi ↗ · pubmed ↗
- 4Downer B. Al Snih S. Chou L. N. Kuo Y. F. Raji M. Markides K. S. Ottenbacher K. J. (2021). Changes in health care use by Mexican American Medicare beneficiaries before and after a diagnosis of dementia. Journals of Gerontology. Series A, Biological Sciences and Medical Sciences, 76(3), 534–542. 10.1093/gerona/glaa 23632944734 PMC 7907487 · doi ↗ · pubmed ↗
- 5Downer B. Chou L. N. Al Snih S. Barba C. Kuo Y. F. Raji M. Markides K. S. Ottenbacher K. J. (2021). Documentation of dementia as a cause of death among Mexican-American decedents diagnosed with dementia. Journal of Alzheimer’s Disease, 82(4), 1727–1736. 10.3233/jad-210361 PMC 838469834219726 · doi ↗ · pubmed ↗
- 6Gozalo P. Teno J. M. Mitchell S. L. Skinner J. Bynum J. Tyler D. Mor V. (2011). End-of-life transitions among nursing home residents with cognitive issues. New England Journal of Medicine, 365(13), 1212–1221. 10.1056/nejmsa 110034721991894 PMC 3236369 · doi ↗ · pubmed ↗
- 7Hauber B. Paulsen R. Krasa H. B. Vradenburg G. Comer M. Callahan L. F. Winfield J. Potashman M. Hartry A. Lee D. Wilson H. Hoffman D. L. Wieberg D. Kremer I. N. Taylor G. A. Taylor J. M. Lappin D. Martin A. D. Frangiosa T. . . . Di Benedetti D. B. (2023). Assessing what matters to people affected by Alzheimer’s disease: A quantitative analysis. Neurology and Therapy, 12(2), 505–527. 10.1007/s 40120-023-00445-036763306 PMC 10043143 · doi ↗ · pubmed ↗
- 8IBM Corp. (2021). IBM SPSS statistics for windows, version 28.0. IBM Corp.