Puberty, but not precocious puberty is influenced by weight gain in the first years of life
Vittorio Ferrari, Alessandra Li Pomi, Daniele Ciofi, Malgorzata Gabriela Wasniewska, Stefano Stagi

TL;DR
The study finds that weight gain in early life affects normal puberty timing but not precocious puberty in girls.
Contribution
This study clarifies that weight gain does not influence precocious puberty, distinguishing it from general puberty trends.
Findings
Weight gain in early life correlates with earlier puberty onset in the general population.
Precocious puberty is not associated with weight gain in early life.
Other factors likely contribute to precocious puberty.
Abstract
Factors favouring the secular trend of decreasing average age of puberty include eating habits, environmental endocrine disruptors, genetics, stress and lifestyle. The association between higher BMI and timing and tempo of puberty has long been documented in the general population but data for children with precocious puberty are poor. To evaluate the relationship between the role of weight gain in the first years of life on the onset of central precocious puberty. We analyzed the data of 120 Caucasian girls diagnosed with CPP between May 2020 and March 2021 (group 1) and a control group of 540 girls. Patients with CPP associated with hypothalamic–pituitary congenital malformations, neurological, neurosurgical and/or genetic diseases, psychomotor delay, oncological diseases, other endocrine impairments requiring hormonal treatments, or taking drugs that may interfere with pubertal…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
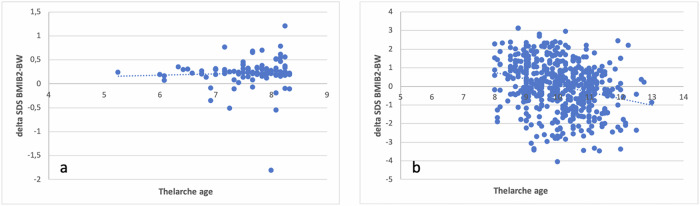 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBirth, Development, and Health · Hypothalamic control of reproductive hormones · Regulation of Appetite and Obesity
Introduction
Puberty is the developmental stage during which secondary sexual characteristics and reproductive capacity are acquired. Over the last few decades, there has been a progressive decrease in the age of pubertal development, especially in girls [1–3]. The factors involved include eating habits, environmental endocrine disruptors, genetics, stress and other lifestyle factors [1, 2, 4, 5].
During the Sars-CoV2 pandemic in Italy, especially in the months of lockdown from March to May 2020, an increase in cases of central precocious puberty (CPP) and rapidly progressing puberty was observed [6–8]. The data suggest that environmental factors, such as nutrition and excessive use of electronic devices, play a role in the early onset of pubertal development [6, 9–12].
The association between higher BMI and earlier onset of puberty has long been known. Increased adiposity is associated with an earlier onset of breast buttons [13–16] and menarche [13, 17] in girls and with an acceleration of pubertal progression [6].
In investigating how BMI affects the process of pubertal development, researchers have focused on the endocrine activity of white adipose tissue, including the production of adipokines and the conversion of androgens to estrogens via the enzyme aromatase [18]. Some studies indicate that important increases in BMI during the first 20 months of life [16], in the first five years [19] and between two and eight years of age [20] are associated with an earlier onset of puberty. Furthermore, there seems to be a relationship between birth weight (BW) and age at puberty [19, 21]. Insulin resistance and excess hepato-visceral fat may play an important role in determining the appearance of the first signs of pubertal development. The early appearance of pubertal development could therefore be a mechanism to minimize increases in central ectopic fat [22]. Variations between BW and childhood BMI could represent a marker for predicting the timing and tempo of puberty [22].
A recent study on a cohort of 577 girls in central Italy showed that a greater variation between BW and Z-score of BMI during childhood corresponds to an earlier onset of puberty and a greater speed of development (defined as a shorter time between thelarche and menarche) [13].
There is no clear evidence regarding the impact of weight gain in the first years of life on the onset of central precocious puberty (CPP). Some studies indicate that a prolonged period of obesity in the first years of life is associated with CPP [23, 24].
Our study aims to evaluate whether these is a correlation between weight gain from birth to the appearance of secondary sexual characteristic and central precocious puberty.
Patients and methods
We carried out a monocentric, retrospective and observational study. We analyzed the data of 120 Caucasian girls diagnosed with CPP by the Auxoendocrinology and Gynecology Unit of Meyer Children Hospital between May 2020 and March 2021 (group 1) and a control group of 540 girls (group 2) who had been referred to the same Operating Unit during the same period for suspected CPP but who did not meet the criteria to receive this diagnosis.
Patients with a diagnosis of CPP and associated hypothalamic–pituitary congenital malformations, neurological, neurosurgical and/or genetic diseases, psychomotor delay, oncological diseases, other endocrine impairments requiring hormonal treatments, or taking drugs that may interfere with pubertal development were excluded from the study. We also excluded children who were born small for gestational age (SGA: birth weight and/or birth length less than 2 SDS below the mean for gestational age) [25], were adopted or had immigrated to Italy as such children have a statistically higher rate of precocious puberty than the general pediatric population.
The study was performed according to the Helsinki II declaration and approved by the local Paediatric Ethical Committee (Paediatric Ethical Committee – Tuscany Region, approval number: 65/2019, in date 03/09/2019). Written informed consent was obtained from the parents of enrolled children.
Study design
All patients underwent periodical auxological examinations during which weight, height, body mass index (BMI) and pubertal progression rate (Tanner scale) were recorded [26]. Birth weight (BW) was collected from the patient’s pediatric booklet. BMI was calculated by dividing the patient’s weight in kilograms by the square of height in meters [27]. Height and BMI were normalized for chronological age by conversion to SD scores [26].
Pubertal development was classified according to the Marshall and Tanner criteria [28]. The age of pubertal onset was defined as the age at durable Tanner B2 stage, confirmed by auxological, endocrinological and/or radiological results [29].
Precocious puberty was defined as the development of pubertal changes at an age that was younger than the accepted lower limits for onset of puberty (before the age of 8 years in girls) [30]. We considered peak LH values of > 5 IU/L on the GnRH stimulation test in the presence of pubertal signs or a basal LH value of > 1.1 IU/L and a ratio of stimulated LH to stimulated FSH of > 1.0 combined with isolated pubic and/or axillary hair growth accompanied by breast development [30] to be indicative of activation of the hypothalamic GnRH pulse generator.
Auxological evaluation
Height was measured using Harpenden’s stadiometer in triplicate to the nearest 0.1 cm. Weight was determined to the nearest 0.1 kg using a balance scale. To calculate the standard deviation scores of the neonatal data (weight and length at birth) we considered the Italian Neonatal Study [INeS] charts [31]; for auxological parameters (height, weight and BMI at the time of thelarche) we used the Italian cross sectional growth charts of Cacciari et al. [32]. Girls with a BMI above the 85th centile (+1 SDS) were considered overweight [33]. To evaluate the influence of the accumulation of central ectopic fat on the age of pubertal development we used the formula described by de Zegher et al. [22, 34].
Within the group of girls diagnosed with CPP, we calculated the delta SDS between BMI at the onset of B2 and birth weight (delta SDS BMIB2-BW) [22] and subsequently looked for any correlation between this value and the age of onset of pubertal development (attainment of Tanner stage B2).
Statistical analysis
Statistical analyses were performed with SPSS X software (SPSSX Inc., Chicago, IL, USA). The characteristics of the study population were described using frequency distributions for categorical variables and mean and standard deviation (SD) values, medians, and ranges for continuous variables, depending on whether the data were normally distributed. The statistical significance of the continuous variable comparisons was assessed using the Student t test and the Mann-Whitney U test, depending on the distribution of the analyzed variable; the comparison of categorical variables was conducted using the chi square test or Fisher’s Exact test if there was a small (<5) expected cell size. The Pearson correlation test was used to determine the correlation coefficients. All statistical tests were two-tailed and a p < 0.05 was considered statistically significant.
Results
The mean age at the onset of B2 within girls diagnosed with CPP (group 1) was 7.67 ± 0.88 years; the mean BMI of this group was 17.43 ± 2.29 kg/m^2^ (0.14 ± 0.88 SDS), average BW was 3097.150 ± 507.179 gr (−0.08 ± 1.04 SDS) and the mean height was 129.99 ± 7.58 cm (0.60 ± 0.94 SDS). Evaluating the delta SDS BMIB2-BW, we did not observe any statistically significant relationship between these values (R: 0.037; p = 0.85) (Table 1).Table 1. Main results observed in the two study groupsSubjects (n°)Mean age at B2 (years)BW (g)SDS BW^a^BMI at B2 (kg/m^2^)SDS BMI at B2^b^Correlation coefficient (R)P valueGroup 11207.67 ± 0.883097.150 ± 507.179−0.08 ± 1.0417.43 ± 2.290.14 ± 0.880.0370.85Group 254010.06 ± 1.033182.600 ± 460.458−0.03 ± 0.9318.57 ± 2.94−0.02 ± 1.010.27<0.0001^a^According to the the Italian Neonatal Study [INeS] charts [28]^b^According to the Italian cross-sectional growth charts of Cacciari et al. [29]
The mean age of onset of B2 for girls in the control group (group 2) was 10.06 ± 1.03 years, whereas mean BMI was 18.57 ± 2.94 kg/m^2^ (−0.02 ± 1.01 SDS), mean BW was 3182.600 ± 460.458 gr (−0.03 ± 0.93 SDS) and average height was 141.00 ± 7.57 cm (0.29 ± 1.03 SDS) Fig. 1. In this group, we observed a statistically significant relationship between delta SDS BMIB2-BW and age at thelarche (R: 0.27; p < 0.0001), confirming findings previously reported by Ferrari et al. [13].Fig. 1. Correlation between delta SDS BMIB2-BW and thelarche age in: a girls diagnosed with CPP (group 1; R: 0.037; p = 0.85); b control group (group 2; R: 0.27; p < 0.0001
Among the overweight girls in group 1 (18 out of 120 patients, 15%), mean age at onset of pubertal development was 7.29 ± 1.7 years, with a mean height of 129.64 ± 12.92 cm (0.89 ± 1.03 SDS), an average BW of 3763.666 ± 354.795 gr (0.37 ± 1.44 SDS) and an average BMI of 21.38 ± 2.03 kg/m^2^ (1.41 ± 0.33 SDS). In this subgroup we did not observe a statistically significant intercurrent relationship between delta SDS BMIB2-BW and age at thelarche (R: 0.094; p = 0.81), although the small number of girls in this group must be taken into account.
Discussion
Our data confirm the influence of weight change from birth to the time of Tanner stage B2 (delta SDS BMIB2-BW) on the age of pubertal development in healthy girls as previously observed in a study by Ferrari et al. [13].
We did not observe the same relationship in the group of girls diagnosed with CPP, and we thus hypothesize that other factors play a crucial role in the development of this condition.
Even in the overweight girls of the group, there would was no association between pubertal development and weight variation from birth. However, we acknowledge that this subgroup was small. In fact, in our cohort of girls diagnosed with CPP only 18 out of 120 (15%) were overweight at the time of diagnosis.
Our study suggests that precocious puberty is not triggered or aggravated by weight variation in the first years of life.
These observations are in contrast with findings in healthy children in the general population in whom weight gain does lead to earlier onsets of puberty [13–16]. Moreover, SGA patients also show an age at menarche earlier and a pubertal progression slightly faster than general population, related also to a premature adrenarche and an accelerated weight gain during early childhood [25].
The interaction between adipokines and neuronal circuits involved in regulating the timing of pubertal development has been extensively studied. As far as we know, the adipokines produced by adipose tissue are among the main regulators of eating behavior and carry out their role by acting on the hypothalamus. The leptin-kisspeptin axis is the most fully understood of the interaction systems between adipokines and neuronal networks [18]. Leptin is an appetite suppressant hormone that regulates the level of body mass in the long term and operates by turning off hunger neurons at the hypothalamic level [35]. After binding to its receptor, it causes the activation of kisspeptin-secreting neurons, that inform the body that there are sufficient energy reserves to start a period of fertility. It has been shown that leptin concentration increases before the onset of puberty in girls and a leptin peak precedes that of gonadotropins [36, 37]. Also noteworthy is the negative correlation found by Matkovic et al. between age of menarche and leptin concentration in girls [38].
Another metabolic regulator which behaves in the opposite way to leptin is ghrelin, which is secreted when the stomach is empty and when there is a negative metabolic balance [39]. Ghrelin depresses kisspeptin expression at the arcuate nucleus of the hypothalamus [39].
We also know that receptors for adiponectin are present at hypothalamic, pituitary and gonadal levels. Adiponectin inhibits the activity of GnRH neurons via AMP kinase pathways and has an insulin-sensitizing action [40]. Its lower concentration in obese patients compared to healthy controls could play a role in the earlier onset of puberty in the former [41].
We have been aware of the association between increased BMI and hyperinsulinemia for a long time [42] and we know that elevated levels of insulinemia are associated with a reduction in the concentration of sex-hormone-binding-globulins. This would determine a greater bioavailability of sex hormones [43] and consequently it could influence the timing of pubertal development.
Our study suggests that weight gain plays a crucial role in the trend of earlier puberty in the general population, but that there are other important factors at play in patients with real precocious puberty. These might include genetics, endocrine disruptors and lifestyle habits (e.g. increased use of electronic devices) [6, 9–12].
In conclusion, it is undoubtedly necessary to conduct studies on larger cohorts of girls diagnosed with CPP to better understand the role of weight gain in the first years of life in the early development of sexual characteristics. At the same time, our study suggests that it is equally important to investigate other factors which may trigger or aggravate this pathological condition.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Turriziani Colonna, A.; Curatola, A.; Sodero, G.; Lazzareschi, I.; Cammisa, I.; Cipolla, C. Central precocious puberty in children after COVID-19 outbreak: a single-center retrospective study. Minerva Pediatr. (2022) 10.23736/S 2724-5276.22.06827-610.23736/S 2724-5276.22.06827-635586885 · doi ↗ · pubmed ↗
- 2C.B. Weir, A. Jan, BMI classification percentile and cut off points. in: Stat Pearls. (Treasure Island (FL), 2023). Stat Pearls Publishing; 202531082114 · pubmed ↗