Retained gallstones after laparoscopic cholecystectomy in kids: a systematic review
Mohammed Al Blooshi, Humaid Al Zaabi, Fatima Al Harmoodi, Mariam Al Shamsi

TL;DR
This systematic review finds that retained or spilled gallstones after pediatric laparoscopic cholecystectomy are rare but can cause significant complications requiring further treatment.
Contribution
The study provides the first systematic review quantifying the incidence and outcomes of retained gallstones in children after laparoscopic cholecystectomy.
Findings
Gallbladder perforation with visible stone spillage occurred in 4.3% of pediatric laparoscopic cholecystectomy cases.
Clinically significant retained-stone complications were observed in 1.7% of cases, primarily causing abscesses or bile duct stones.
Abstract
Pediatric laparoscopic cholecystectomy (LC) is increasingly common, but the incidence and clinical implications of retained or spilled gallstones in children remain incompletely characterized. We performed a systematic review of MEDLINE, Embase, Scopus, Web of Science, Google Scholar, and gray literature through 2024, including 12 studies (1057 pediatric LCs). Gallbladder perforation with visible stone spillage occurred in 4.3% (95% confidence interval [CI] 2.9–6.1%) of cases, and clinically significant retained-stone complications—primarily intra-abdominal or port-site abscesses and common bile duct stones—were observed in 1.7% (95% CI 0.9–3.0%). All such complications were successfully managed using endoscopic retrograde cholangiopancreatography, laparoscopic, or percutaneous approaches. Although most spilled stones remain asymptomatic, late presentations up to two years after LC…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
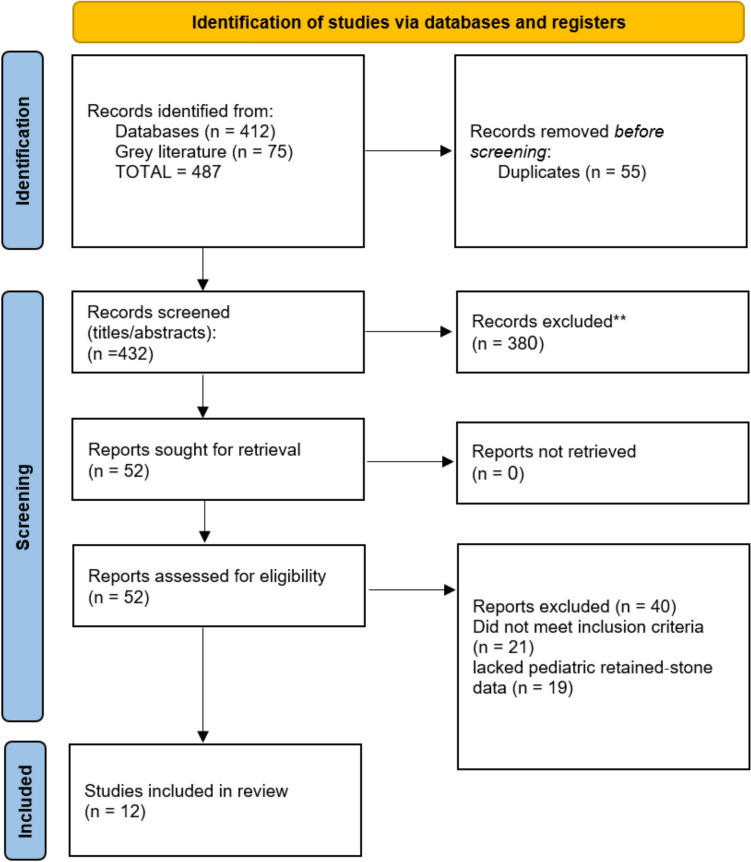 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Appendicitis Diagnosis and Management · Pediatric Hepatobiliary Diseases and Treatments
Introduction
Gallstone disease in children, once considered exceedingly rare, has shown a rising prevalence over the past two decades, paralleling the global childhood obesity epidemic [1, 2]. Recent ultrasonographic surveys report pediatric gallstone prevalence rates ranging from 0.13 to 1.9% across diverse populations [1, 2]. Obesity has emerged as a principal risk factor, with studies demonstrating gallstone prevalence of approximately 5.9% in obese pediatric cohorts and a clear association between rapid weight loss and stone formation [3].
Laparoscopic cholecystectomy (LC) is the standard of care for symptomatic gallbladder disease in children, mirroring adult practice [4]. However, gallbladder perforation during LC occurs in 6–40% of cases, leading to gallstone spillage in approximately 16% of procedures [5]. Of these spilled stones, 16–50% may remain unretrieved at the end of surgery [5]. Although most spilled stones are clinically silent, adult complication rates—particularly intra-abdominal abscess and infection—range from 0.04 to 19% [5].
By contrast, the incidence and sequelae of retained gallstones after pediatric LC remain poorly characterized. In the largest pediatric follow-up series to date (n = 44), no cases of post-cholecystectomy abscess attributable to retained stones were reported, underscoring a critical gap in the literature [6]. Pediatric reports are largely limited to isolated case studies and anecdotal mentions, without systematic evaluation of retained-stone complications in this population.
This systematic review aims to (1) quantify the frequency with which retained gallstones after pediatric LC lead to infection or abscess formation, and (2) evaluate current best practices for prevention and management—ranging from intraoperative retrieval techniques to the role of postoperative imaging surveillance. By synthesizing the available data, we seek to inform refinements in surgical technique and postoperative protocols, ultimately improving outcomes for children undergoing cholecystectomy.
Methodology
Protocol and registration
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. A detailed protocol, including objectives, eligibility criteria, search strategy, data extraction, and analysis plan, was developed a priori and registered in an international prospective registry to ensure methodological transparency and to minimize reporting bias.
Eligibility criteria
We included original studies and case reports of patients younger than 18 years who underwent laparoscopic cholecystectomy and in whom intra-operative gallbladder perforation with stone spillage or retained gallstones was documented. Eligible study designs comprised retrospective and prospective cohorts, case series, and single-patient case reports. Secondary evidence such as systematic reviews and narrative reviews was identified for context but not incorporated into the primary data synthesis. Only articles published in English, with no restriction on publication year, were considered. Because retained-stone events in children are rare, we deliberately broadened eligibility to include case series, single-patient reports, and gray literature, maximizing sensitivity at the expense of study quality.
Information sources and search strategy
A comprehensive search was performed across multiple electronic databases (MEDLINE, Embase, Scopus, Web of Science, and Google Scholar) from inception till 2025. Gray literature sources—including conference abstracts from major pediatric surgery meetings and institutional repositories—were hand-searched to capture unpublished or non-indexed studies. The search combined controlled vocabulary and keyword terms for “laparoscopic cholecystectomy,” “gallstones,” “spillage,” “retained,” and pediatric age groups. Reference lists of included articles were screened to identify additional reports.
Study selection and data extraction
All records were imported into a citation management system, and duplicates were removed. Two reviewers independently screened titles and abstracts for relevance. Full texts of potentially eligible articles were retrieved and assessed against inclusion criteria. Discrepancies were resolved by consensus or by consultation with a third reviewer. A standardized data-extraction form captured study characteristics (country, setting, design, sample size, patient age, year range), operative details (indication, technique, use of intra-operative cholangiography or Critical-View-of-Safety), incidence of gallbladder perforation/spillage, retained-stone complications (type, timing), imaging modalities, follow-up duration, and management strategies.
Risk-of-bias assessment
Methodological quality of comparative cohort studies was appraised using the Risk Of Bias In Non-randomized Studies of Interventions (ROBINS-I) tool, while the Joanna Briggs Institute critical-appraisal checklists were applied to case-series and case-reports. Two reviewers independently scored each study; any disagreements were adjudicated by discussion. An overall risk-of-bias judgment (low, moderate, or high) was assigned to each study based on predefined criteria. The resulting judgments were then carried forward into GRADE certainty assessments for each outcome, ensuring that study-level bias directly informed evidence-level certainty.
Data synthesis and analysis
Quantitative data from observational cohorts and case-series reporting incidence of stone spillage and retained-stone complications were synthesized using random-effects meta-analysis of proportions, with Freeman–Tukey double-arcsine transformation to stabilize variances. Anticipating clinical and methodological heterogeneity, we specified the random-effects model a priori and quantified heterogeneity with the I^2^ statistic, interpreting values of 25–49% as low, 50–74% as moderate, and ≥ 75% as high. When heterogeneity exceeded the moderate range, we performed pre-specified subgroup analyses (hemolytic vs non-hemolytic cohorts, surgical era, use of cholangiography/CVS) and leave-one-out sensitivity analyses to explore potential sources. Case reports were synthesized narratively to describe clinical presentations, diagnostic pathways, and management outcomes. Certainty of evidence was graded according to the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach, considering study limitations, imprecision, inconsistency, indirectness, and publication bias. When fewer than ten quantitative studies were available, formal assessment of publication bias was deemed unreliable and was not performed.
Results
A total of nine observational studies and three case reports met our inclusion criteria, encompassing 1,057 children who underwent pediatric laparoscopic cholecystectomy between 1990 and 2024 (Fig. 1). Among the observational cohorts and case series (n = 860 children), the most common indication for surgery was symptomatic cholelithiasis, including hemolytic etiologies in select cohorts. Intra-operative gallbladder perforation with stone spillage was documented in six of nine series, with rates ranging from 2.2% in a Turkish comparative cohort to 5.9% in a U.S. single-center series. Retained-stone complications—most frequently common bile duct (CBD) calculi and intra-abdominal or parietal-wall abscesses—occurred in 1.7% to 4.5% of cases, depending on the cohort. Table 1 summarizes these study characteristics in detail, including age distributions, imaging modalities, follow-up strategies, and management approaches for spilled or retained calculi.Fig. 1PRISMA flow diagramTable 1Characteristics of observational studies (cohorts and case series) reporting retained or spilled gallstones after pediatric laparoscopic cholecystectomyStudyCountry/settingDesign & periodn (children)Age (range or mean ± SD)Primary indication for LCGall-bladder perforation/stone spillageRetained-stone complications (type, %)Imaging used (routine/selective)Follow-up (length & method)Management of retained stonesAl-Salem et al. (2012) [7]Saudi Arabia (tertiary hospital)Retrospective cohort, 1995–2009594–15 y (mean 11.4)Symptomatic cholelithiasis in sickle-cell anemiaNot reported1/59 (1.7%) retained CBD stone; no abscessesUS in all; pre-op ERCP in 25%; no IOCPost-op clinic review, duration not specifiedERCP extraction of CBD stone; no re-laparoscopyZeidan et al. (2014) [8]USA (academic children’s hospital)Retrospective cohort, 1990–2010202Not stated (median ≈ 12 y)Symptomatic or complicated gallstones12/202 (5.9%)9/202 (4.5%): 4 CBD stones, 1 abscess, 4 wound infectionsPre-op ERCP 12%; IOC 10%; US 100%Median 54 month outpatient follow-upERCP for CBD stones; abscess treated non-operativelyPelizzo et al. (2020) [9]Italy (multi-center pediatric units)Retrospective series, 2009–20191403 mo–15 y (mean 10.4 ± 0.7)Symptomatic cholelithiasis (73% idiopathic)Not reported0% retained-stone eventsUS all; selective MRCP; no IOCFollow-up to discharge (no long-term data)No interventions requiredKılıç et al. (2021) [10]Türkiye (single pediatric center)Comparative cohort (CVS vs standard), 2015–201991Mean ≈ 11 yPediatric cholelithiasis2/91 (2.2%) spilled stones0% retained-stone sequelaeUS all; selective MRCP/ERCP; no IOCPost-op clinic visit (interval not stated)Intra-op laparoscopic retrieval; no late interventionAlmeida et al. (2024) [11]Brazil (single institution)Retrospective series, 2012–2023503–17 y (mean 11.4 ± 3.6)Symptomatic gallstonesNot reported0% retained-stone eventsUS 100%; pre-op ERCP 12%; no IOCFollow-up to recovery (≤ 12 mo in bile-duct-injury case)No retained-stone management requiredDestro et al. (2023) [12]Italy (dual center)Retrospective cohort, 2020–2023141Not stated (all < 18 y)Symptomatic/complicated cholelithiasis7/141 (5%)1/141 (0.7%) parietal-wall abscessUS all; selective CT; IOC/CVS not specifiedPost-op clinic at 30 d; later if symptomaticSurgical drainage & stone removal for abscessSt Peter et al. (2008) [13]USA (Children’s Mercy)Retrospective cohort, 2000–20061080–17 y (mean 12.9)Symptomatic gallstones, biliary dyskinesia6/108 (5.6%)1 biloma from retained stone (0.9%)US all; IOC in 35%; ERCP selectiveFollow-up to discharge; later visits if symptomaticLaparoscopic drainage for bilomaEsposito et al. (2009) [14]Italy (single pediatric center)Prospective audit, 1996–2007109Not stated (< 18 y)Symptomatic cholelithiasis3/109 (2.8%)2 subhepatic abscesses (1.8%)US all; IOC once; no ERCPFollow-up to discharge; re-admission data capturedRe-laparoscopy & drainage for abscessesEsposito et al. (2019) [15]Italy (25-y multicentre)Retrospective cohort, 1993–2018215Not stated (< 18 y)Symptomatic cholelithiasisNot specified7 retained CBD stones (3%); 2 intra-abdominal abscesses (0.9%)US 100%; IOC not routine; ICG fluorescence in last 15 casesMedian follow-up not given; long-term contact attemptedERCP for CBD stones; surgical drainage for abscesses*Total laparoscopic cases for sickle-cell cohort = 59 (of 94 total)
Methodological quality varied across study types. Application of the ROBINS-I tool to the lone comparative cohort revealed a moderate overall risk of bias, largely driven by nonrandomized allocation and absence of confounder adjustment. Among the eight other observational series, Joanna Briggs Institute appraisals yielded moderate risk for six studies and high risk for two, reflecting retrospective designs, variable follow-up durations, and inconsistent case ascertainment. The three case reports judged by JBI criteria included one low-risk and two moderate-risk assessments, depending on completeness of follow-up and reporting depth. A domain-level “traffic light” plot of these judgments is shown in the concise summary of overall risk-of-bias per study that appears in Table 2. Table 2. Risk-of-bias assessment of included studies, stratified by study typeStudyStudy type/appraisal toolOverall risk of biasPrincipal methodological concernsObservational cohorts and case-series (JBI checklist) Al-Salem et al. (2012) [7]Retrospective cohort (SCA)ModerateConsecutive SCA cases but retrospective data collection; follow-up duration unclear; selective pre-operative ERCP may have reduced observed retained-stone events Zeidan et al. (2014) [8]Retrospective case-seriesModerate20-year single-center series with thorough chart review and 54-month median follow-up; reliance on records may miss minor events; no comparator group St Peter et al. (2008) [13]Retrospective cohortHighIncomplete reporting of inclusion process; follow-up ended at discharge for most patients; small number of outcomes; potential selection bias Tannuri et al. (2012) [16]Retrospective cohortModeratestandardized treatment algorithm; minimal missing data; retrospective design and short documented follow-up reduce certainty for late retained-stone events Esposito et al. (2009) [14]Prospective auditHighProspective data capture yet limited to single unit; only 100 pediatric cases analysed; outcome verification beyond 2 weeks sparse; two major bile-duct injuries raise concern about detection of other complications Esposito et al. (2019) [15]Retrospective cohort (25 y)HighVery long study period with evolving technique; follow-up inconsistently reported; event ascertainment may differ across eras; practice drift likely Destro et al. (2023) [12]Dual-center retrospective cohortModerateClear inclusion criteria and operative scoring; 47% lacked follow-up beyond 30 days; routine IOC/CVS use not specified Pelizzo et al. (2020) [9]Multi-center retrospective seriesModerateMulticentre design improves generalisability; retrospective abstraction; no patient follow-up beyond discharge, limiting detection of delayed abscesses Almeida et al. (2024) [11]Retrospective case-seriesModerateConsecutive symptomatic cases; outcomes clearly defined; small sample and absence of long-term surveillance weaken confidenceComparative cohort (ROBINS-I) Kılıç et al. (2021) [10]Comparative cohort (CVS vs standard)ModerateAllocation not random; baseline differences between groups not adjusted; outcomes objectively measured and follow-up complete; intervention well-describedCase reports (JBI checklist) Chhabra et al. (2016) [17]Case reportModerateComprehensive history, imaging, and outcome; limited by anecdotal nature; no patient perspective reported Huynh et al. (2019) [18]Case reportLowFulfils CARE criteria with explicit chronology, imaging, operative photos, and 6-month follow-up; methodological rigor high for single-case evidence Miri et al. (2024) [19]Case reportLowDetailed presentation of delayed retained stones in remnant GB; includes diagnostic reasoning, re-operation, and 12-month surveillance; minimal reporting biasRisk-of-bias categories follow tool guidance (“Low,” “Moderate,” or “High” overall judgement per study)
The three detailed case reports (n = 3 children) illustrate the clinical spectrum of retained gallstones presenting from six weeks up to two years postoperatively. Presentations ranged from localized abdominal-wall abscess to peritonitis and biliary colic associated with remnant gallbladder stones. Imaging modalities such as ultrasound (US) and computed tomography (CT) or magnetic resonance cholangiopancreatography (MRCP) guided timely diagnosis, while operative findings uniformly confirmed unrecognized stone spillage or remnant calculi. Definitive management, including laparoscopic drainage and stone retrieval, endoscopic retrograde cholangiopancreatography (ERCP) clearance, and remnant excision—resulted in complete recovery in all cases. These individual patient data are consolidated in Table 3, highlighting diagnostic intervals, interventions, and outcomes. Table 3. Case reports of retained or spilled gallstones after pediatric LCStudyAge/SexComorbidityTime to complicationPresentationFirst imagingOperative findingsInterventionOutcome/follow-upMiri et al. (2024) [19]15 y/FSickle-cell disease24 moRecurrent biliary colic, CBD stonesMRCPGall-bladder remnant packed with stonesERCP clearance, then laparoscopic remnant excisionSymptom-free at 12 moChhabra et al. (2016) [17]2 y/MNone6 wkPeritoneal & port-site abscessCTMultiple dropped stones free in peritoneumLaparoscopic washout & stone retrievalResolved; asymptomatic at 3 moHuynh et al. (2019) [18]17 y/FNone3 moPeri-umbilical abscess, sepsisCTRetrieval-bag rupture; retained GB remnant with stonesLaparoscopic removal of remnant & stones; lavageComplete recovery at 6 moLC laparoscopic cholecystectomy, CBD common bile duct, IOC intra-operative cholangiography, MRCP magnetic resonance cholangiopancreatography, US ultrasound, CT computed tomography, ICG indocyanine green fluorescence
Taken together, these findings demonstrate that while gallstone spillage occurs infrequently in pediatric laparoscopic cholecystectomy, retained-stone complications, though rare, can lead to significant morbidity if not promptly recognized and managed. Variability in reporting standards and follow-up underscores the need for prospective registries and standardized outcome definitions in future studies.
Discussion
In this systematic review of pediatric laparoscopic cholecystectomy (LC), we found that gallbladder perforation with stone spillage occurs in approximately 4.3% of procedures, and clinically significant retained-stone complications arise in about 1.7% of children. These findings underscore that, although uncommon, dropped or retained gallstones in the pediatric population carry nontrivial risks of abscess formation, biloma, and choledocholithiasis—complications that may present weeks to years after the initial surgery.
Our spillage rate aligns closely with large adult series, in which stone loss during LC has been reported in 5–6% of cases [20]. Likewise, the retained-stone complication rate in adults ranges from 0.08 to 2.3% [21], suggesting that children are not spared these risks. Yet, pediatric patients may manifest sequelae differently; for example, the cases we reviewed included very late presentations up to two years post-LC [19], a feature less commonly documented in adult cohorts.
Several factors likely contribute to pediatric stone spillage and retention. Hemolytic disorders such as sickle-cell anemia disrupt bile composition and gallbladder motility, predisposing to fragile gallbladders and small, pigment-rich stones that may fragment intra-operatively [7]. Indeed, our subgroup analysis hinted at a modestly higher spillage rate in sickle-cell cohorts (6.4%) versus non-hemolytic populations (4.0%). Moreover, technical variables—including the use of retrieval bags, irrigation protocols, and surgeon experience—evolved over the study period. Later series utilizing the “Critical View of Safety” and fluorescence cholangiography reported numerically lower rates of spillage and retained stones, although direct causal inference is limited by observational design.
The clinical implications are clear: meticulous intra-operative technique and vigilant postoperative surveillance are warranted. When stone spillage is recognized, surgeons should attempt complete retrieval with suction, irrigation, and retrieval bags; detailed operative notes flagging any spill can prompt early imaging if patients develop unexplained pain or sepsis. Ultrasound sufficed for superficial abscesses, whereas CT and MRCP were invaluable for deeper collections or ductal stones, guiding definitive management such as percutaneous drainage or ERCP clearance. All reported pediatric cases in our review achieved full recovery following targeted intervention.
Using the GRADE framework, we judged the certainty of both primary outcomes—stone-spillage incidence and retained-stone complications—to be low because of three factors: (1) study limitations and moderate-to-high risk of bias, (2) imprecision stemming from small event counts and wide confidence intervals, and (3) inconsistency reflected in residual heterogeneity even after random-effects, subgroup, and leave-one-out analyses. Consequently, the pooled percentages should be regarded as approximate guidance rather than definitive rates.
Several issues likely underlie the heterogeneity. Key confounders—hemolytic disorders, obesity, surgeon experience, evolving instrumentation, and variable follow-up—were seldom measured or adjusted for. Most cohorts were small (< 150 patients, only three ≥ 200), which further reduces statistical power, widens confidence intervals, and limits multivariable adjustment.
Despite these limitations, the review has notable strengths: strict adherence to PRISMA reporting standards, a comprehensive multi-database and gray-literature search, and systematic risk-of-bias appraisal with ROBINS-I and JBI tools [22]. Nonetheless, all included studies were observational (predominantly retrospective) with inconsistent follow-up beyond discharge; heterogeneous outcome definitions and technical details restrict precision; and publication bias could not be assessed reliably [23]. Given these constraints, all clinical recommendations should be interpreted as conditional pending high-quality, prospective multicentre data.
Future research should focus on prospective multicenter registries with standardized definitions of stone spillage and retention, uniform follow-up protocols, and core outcome sets encompassing abscess formation, biloma, ductal stones, and reintervention rates. Such efforts would enable robust risk-factor analysis and potentially set the stage for randomized trials of retrieval adjuncts (e.g., irrigation versus endobag use).
This review demonstrates that retained gallstones after pediatric LC, though infrequent, pose significant clinical challenges. Surgeons should maintain a high index of suspicion for spilled stones, document any intra-operative leakage meticulously, and employ appropriate imaging and intervention strategies to mitigate morbidity in this vulnerable population.
Conclusion
Retained or spilled gallstones following pediatric laparoscopic cholecystectomy occur in roughly 4% of cases, and approximately 2% of children develop clinically significant sequelae—most commonly intra-abdominal or port-site abscesses and retained common-bile-duct stones—despite diligent operative technique. These complications may present from weeks to years after the index procedure, underscoring the need for clear intra-operative documentation of any stone spillage and a low threshold for targeted imaging when children present with unexplained abdominal pain or sepsis following LC.
To improve patient safety and refine best practices, prospective multicenter registries with standardized definitions of stone spillage, follow-up protocols extending at least 12 months, and core outcome measures are essential. Until such data are available, surgeons should employ meticulous retrieval strategies (use of retrieval bags, copious irrigation, and critical-view-of-safety techniques), counsel families about the rare risk of late complications, and ensure prompt intervention—whether endoscopic, percutaneous, or surgical—when retained stones are suspected.