Geotrichosis Due to Magnusiomyces capitatus: A Severe Emerging Invasive Fungal Disease
Fatima Zahra Lfaquir, Abderrahim Chour, Imane Zouaoui, Khalil Zimi, Sarra Aoufi

TL;DR
A rare and severe fungal infection caused by Magnusiomyces capitatus in a cancer patient highlights the need for rapid and accurate diagnosis.
Contribution
Reports a fatal case of invasive M. capitatus infection and emphasizes the importance of modern diagnostic tools.
Findings
M. capitatus was identified using MALDI-TOF mass spectrometry in a neutropenic cancer patient.
The patient died despite appropriate antifungal treatment, underscoring the severity of the infection.
Invasive M. capitatus infections are rare but life-threatening in immunocompromised individuals.
Abstract
Geotrichosis is a rare opportunistic mycosis caused by emerging yeasts rarely associated with fungemia. We report a case of invasive Magnusiomyces capitatus (M. capitatus) infection in a neutropenic patient. A 71-year-old man with rectosigmoid cancer undergoing chemotherapy was admitted to the emergency department with septic shock. Laboratory tests revealed a severe inflammatory response, agranulocytosis, and acute renal failure requiring hemodialysis via a femoral catheter. An infectious workup performed at the Central Parasitology and Mycology Laboratory of Ibn Sina University Hospital in Rabat included blood cultures, urine samples, hemodialysis catheter samples, and a protected distal specimen (PDS). Empirical broad-spectrum antibiotic therapy was initiated, followed by caspofungin due to a lack of clinical improvement. Microscopic examination of urine, catheter, and PDS specimens…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
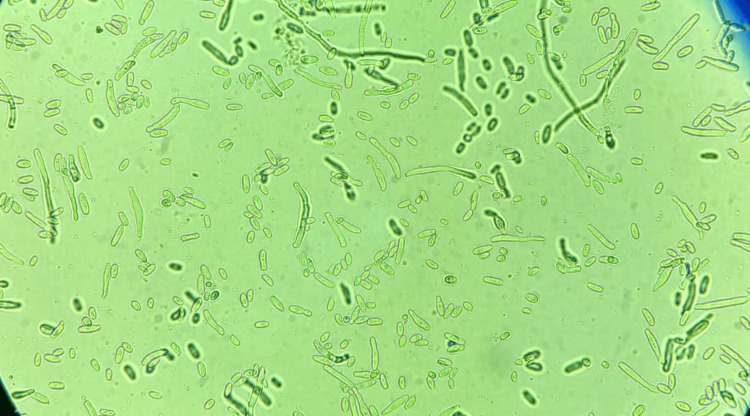 Figure 1
Figure 1| Parameter | Patient result | Normal range/reference values |
| C-reactive protein (CRP) | 492 mg/L | <5 mg/L |
| Creatinine | 28 mg/L | 7.2-12.5 mg/L |
| Urea | 0.12 g/L | 0.03-0.07 g/L |
| Sodium (Na⁺) | 140 mEq/L | 135-145 mEq/L |
| Potassium (K⁺) | 5.8 mEq/L | 3.5-5.1 mEq/L |
| Chlorides (Cl⁻) | 105 mEq/L | 98-107 mEq/L |
| Bicarbonates (HCO₃⁻) | 18 mEq/L | 22-28 mEq/L |
| Neutrophils (agranulocytosis) | 0.4 × 10³/μL | 6-26 × 10³/μL |
| Platelets (thrombocytopenia) | 6 G/L | 150-450 G/L |
| Hemoglobin | 8 g/dL | 13.4-19.8 g/dL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntifungal resistance and susceptibility · Infectious Diseases and Mycology · Fungal Infections and Studies
Introduction
Geotrichosis is a rare opportunistic fungal infection caused by emerging yeasts belonging to the genus Geotrichum. This genus was recently reclassified as *Magnusiomyces capitatus (M. capitatus) *(formerly Geotrichum capitatum). These yeasts are ubiquitous in the environment and form part of the normal microbiota of the respiratory and gastrointestinal tracts. It is believed that infection primarily occurs through inhalation or translocation from the gut in immunocompromised patients [1]. Although M. capitatus-caused invasive infections are increasingly recognized as emerging pathogens, they remain uncommon and poorly understood in clinical practice [2]. These infections primarily affect immunocompromised patients, especially those undergoing intensive treatments such as chemotherapy. This population is at a higher risk for severe complications.
Furthermore,* M. capitatus *exhibits intrinsic resistance to certain antifungal agents, particularly echinocandins, which are commonly used to treat invasive fungal infections. This resistance complicates therapeutic management significantly and may lead to increased morbidity and mortality associated with these infections [3]. Therefore, improving our understanding of the clinical, microbiological, and therapeutic characteristics of this emerging mycosis is essential to enabling earlier diagnoses and tailoring antifungal strategies to optimize patient outcomes. This study reports a case of invasive geotrichosis caused by *M. capitatus *in a neutropenic patient with rectosigmoid carcinoma undergoing chemotherapy.
Case presentation
This 71-year-old patient has no prior medical history and is being treated for rectosigmoid carcinoma. He was receiving chemotherapy according to the FOLFIRINOX protocol, which included oxaliplatin (85 mg/m²), irinotecan (180 mg/m²), leucovorin (400 mg/m²), followed by a 5-fluorouracil bolus (400 mg/m²) and a continuous infusion (2400 mg/m² over 46 hours), administered every two weeks. One month after beginning treatment, the patient was admitted to the emergency department in septic shock. He presented with a fever, persistent hypotension despite fluid resuscitation, tachycardia, and altered mental status. Laboratory tests revealed severe inflammation, agranulocytosis, thrombocytopenia, and acute renal failure requiring hemodialysis (Table 1).
Based on the clinical and laboratory findings, including blood cultures, urine specimens, hemodialysis catheter samples, and a protected distal specimen (PDS), an infectious disease assessment was carried out. The samples were sent to the Central Parasitology and Mycology Laboratory at Ibn Sina University Hospital in Rabat. Broad-spectrum antibiotic therapy was promptly initiated. However, due to the absence of clinical improvement, fungemia was suspected, and antifungal treatment with caspofungin was initiated, administered intravenously at a dose of 70 mg per day. Microscopic examination of the urine, the hemodialysis catheter, and the PDS revealed filaments fragmenting into arthrospores at 40x magnification. Blood cultures were positive after 20 hours of incubation. After 24 hours of incubation in aerobic conditions at 37°C on Sabouraud-Chloramphenicol and Sabouraud-Cycloheximide media, cultures of all samples showed whitish colonies with a dry appearance and irregular contours. Microscopic examination of the cultures revealed filaments with arthrospores, indicating* Geotrichum spp*. (Figure 1).
Microscopic view of the arthrospores of Geotrichum spp. after culture at 40x magnification
Mass spectrometry (matrix-assisted laser desorption/ionization time-of-flight (MALDI-TOF)) revealed that the fungal agent was precisely identified as M. capitatus. Despite intensive voriconazole treatment, the patient's condition deteriorated. The patient died 10 days after being admitted to the hospital.
Discussion
*M. capitatus *is a cosmopolitan, opportunistic yeast that is saprophytic in the external environment and commensal in the digestive, respiratory, and skin tracts of humans. It can cause serious invasive infections, primarily in immunocompromised patients [4,5].
Systemic infections with M. capitatus in immunocompromised patients are less common than invasive candidiasis and aspergillosis [6]. Similar risk factors have been identified, including profound neutropenia secondary to chemotherapy, dysbiosis due to prophylactic antibiotic use, and the presence of invasive devices such as catheters [4,5,7]. Our patient had all these risk factors: he had a solid tumor and was receiving hematotoxic chemotherapy, which induced profound neutropenia. He was also receiving broad-spectrum antibiotic therapy and had a hemodialysis catheter.
The clinical manifestations of invasive geotrichosis generally resemble those of other invasive fungal infections, particularly candidiasis. The infection most often begins with an acute fever that does not respond to antibiotics. It usually progresses rapidly, leading to multiple organ failure despite appropriate antifungal treatment [8].
In our patient's case, the persistence of fever despite the initiation of broad-spectrum antibiotic therapy strongly suggested an invasive fungal infection, justifying treatment with caspofungin at a dose of 70 mg intravenously.
The diagnosis of invasive geotrichosis is primarily based on blood culture, which remains the gold standard for detecting the spread of this fungus. According to data from the literature, 75% of disseminated *M. capitatus *infections are diagnosed by blood culture [9]. In our case, blood cultures also proved positive within 24 hours.
M. capitatus was detected in several locations, including the urine, the hemodialysis catheter, and the PDS. This is consistent with data from the literature, where approximately 43% of cases involved more than one site [9]. The fact that the fungus was isolated from multiple sites suggests hematogenous spread of the infection.
The treatment of invasive* M. capitatus* infections is complicated by their rarity and the fact that they are often confused with invasive candidiasis due to their similar clinical presentation. This similarity can lead to diagnostic errors and inappropriate initial treatment choices. Indeed, several studies have shown that all M. capitatus isolates have high minimum inhibitory concentrations (MICs) for echinocandins, revealing intrinsic resistance to this class of antifungal agents [3]. Combined with the lack of official treatment recommendations and standardised sensitivity thresholds, this resistance makes management difficult and treatment responses highly variable, highlighting the need for an individualised therapeutic approach [10]. Furthermore, current recommendations advocate empirical antifungal treatment with caspofungin or lipid amphotericin B for patients with fever and neutropenia. In our case, treatment with caspofungin was initially initiated due to suspicion of invasive candidiasis, but it proved ineffective.
Invasive M. capitatus infections are associated with a poor prognosis due to nonspecific clinical signs and diagnostic difficulties. The outcome is particularly serious in patients with severe neutropenia. Despite the use of antifungal treatments such as liposomal amphotericin B, itraconazole, or flucytosine, mortality can reach 90% [11]. In our case, the patient died 10 days after admission despite intensive treatment with voriconazole.
Conclusions
The presented case underscores the severity of *M. capitatus *infections in immunocompromised patients and highlights the importance of rapid, accurate diagnosis and therapeutic management. Clinicians must be vigilant about the emergence of these mycoses, especially in immunocompromised individuals. Furthermore, rapid and reliable identification of fungi, notably through techniques such as mass spectrometry, is essential to selecting appropriate antifungal therapy. This will reduce associated mortality and optimize the management of invasive fungal infections.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Outbreak of Saprochaete clavata sepsis in hematology patients: combined use of MALDI-TOF and sequencing strategy to identify and correlate the episodes Front Microbiol Lo Cascio G Vincenzi M Soldani F 841120203208229310.3389/fmicb.2020.00084 PMC 7004961 · doi ↗ · pubmed ↗
- 2Blastoschizomyces capitatus pulmonary infections in immunocompetent patients: case report, case series and literature review Epidemiol Infect Tanabe MB Patel SA 586414620182919820310.1017/S 0950268817002643 PMC 9134742 · doi ↗ · pubmed ↗
- 3Yeast-like filamentous fungi: molecular identification and in vitro susceptibility study Med Mycol Esposto MC Prigitano A Lo Cascio G 9099135720193052100710.1093/mmy/myy 133 · doi ↗ · pubmed ↗
- 4Saprochaete clavata infections in patients undergoing treatment for haematological malignancies: a report of a monocentric outbreak and review of the literature Mycoses Stanzani M Cricca M Sassi C 110011076220193136516110.1111/myc.12978 · doi ↗ · pubmed ↗
- 5Predisposing factors and outcome of uncommon yeast species-related fungaemia based on an exhaustive surveillance programme (2002-14)J Antimicrob Chemother Bretagne S Renaudat C Desnos-Ollivier M Sitbon K Lortholary O Dromer F 178417937220172833325910.1093/jac/dkx 045 · doi ↗ · pubmed ↗
- 6ESCMID and ECMM joint clinical guidelines for the diagnosis and management of rare invasive yeast infections Clin Microbiol Infect Arendrup MC Boekhout T Akova M Meis JF Cornely OA Lortholary O 769820201410.1111/1469-0691.1236024102785 · doi ↗ · pubmed ↗
- 7Case of fatal Blastoschizomyces capitatus infection occurring in a patient receiving empiric micafungin therapy Antimicrob Agents Chemother Chittick P Palavecino EL Delashmitt B Evans J Peacock JE Jr 530653075320091973800510.1128/AAC.00710-09PMC 2786321 · doi ↗ · pubmed ↗
- 8Saprochaete clavata invasive infections-z new threat to hematological‑oncological patients Front Microbiol Buchta V BolehovskáR HovorkováE Cornely OA Seidel D Žák P 21961020193173688310.3389/fmicb.2019.02196 PMC 6830389 · doi ↗ · pubmed ↗