A Case of Nontuberculous Mycobacterial Pulmonary Disease Complicating Massive Pulmonary Embolism
Yasuyuki Hayashi, Akihiko Sokai, Toshiyuki Iwata, Yuki Sakai, Naoaki Yasuda, Takashi Nishimura

TL;DR
A man developed a rare lung infection caused by non-tuberculosis mycobacteria two years after being treated for a severe blood clot in his lung.
Contribution
This case suggests a possible link between chronic pulmonary embolism and the later development of nontuberculous mycobacterial disease.
Findings
The patient was diagnosed with a large pulmonary embolism and treated with anticoagulants.
Two years later, he developed Mycobacterium avium infection in the same lung area.
The authors suggest that chronic pulmonary embolism may predispose to nontuberculous mycobacterial disease.
Abstract
A 39‐year‐old man presented with fever and dyspnoea for 1 week. Imaging suggested bacterial pneumonia with infiltrates in the right lung. However, the symptoms persisted despite antibiotics. Bronchoscopy revealed coagulation necrosis, and enhanced computed tomography identified a large thrombus in the right pulmonary artery, leading to a diagnosis of pulmonary infarction. The patient was treated with direct oral anticoagulants. Two years later, new nodular lesions with cavities were observed in the upper lobe of the right lung. Bronchoscopy revealed a Mycobacterium avium infection. We hypothesise that nontuberculous mycobacterial (NTM) pulmonary disease may complicate chronic pulmonary embolism. We report a rare case of non‐tuberculous mycobacterial disease 2 years after treatment for pulmonary embolism. If a persistent cough or sputum is present after pulmonary embolism, it may be…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
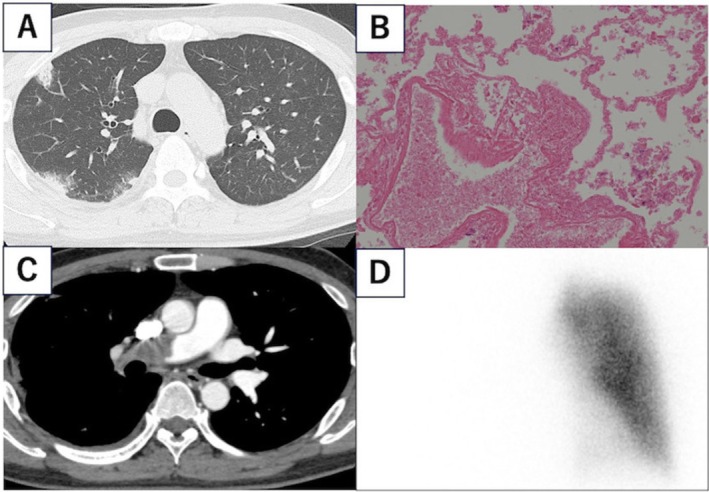 FIGURE 1
FIGURE 1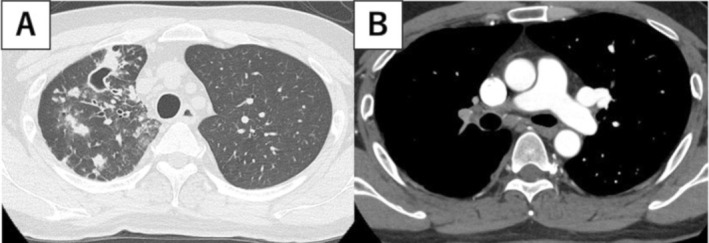 FIGURE 2
FIGURE 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMycobacterium research and diagnosis · Infectious Diseases and Mycology
Introduction
1
We report a rare case of NTM pulmonary disease 2 years after treatment for pulmonary embolism. Chronic embolism‐induced blood flow disorders may contribute to the development of NTM. If a persistent cough or sputum is present after pulmonary embolism, it may be necessary to consider the possibility of NTM pulmonary disease and perform imaging tests.
Case Report
2
A 39‐year‐old man was referred to our hospital with fever and dyspnoea lasting 1 week. He had a history of Mycobacterium kansasii infection at Age 24, which was treated successfully over a year. He had no history of other infectious diseases. He was found to be HIV‐negative, but no other tests for immunodeficiency were performed. On admission, his oxygen saturation level was 94% on room air. Laboratory tests showed a C‐reactive protein (CRP) of 15.3 mg/dL and D‐dimer of 4.4 μg/mL. Computed tomography (CT) showed scattered infiltrates in the peripheral areas of the right lung lobe and right pleural effusion (Figure 1A). Initially diagnosed with bacterial pneumonia, the patient's condition worsened despite antibiotic administration.
Radiographic and pathological images at first examination. (A) Plain computed tomography (CT) showing scattered infiltrations in the peripheral areas of the right lung lobe. (B) Haematoxylin and eosin staining showing that nuclear staining has disappeared in the blood vessels and alveolar regions, but the structure is preserved. It is an image of coagulation necrosis, suggesting ischaemic changes such as pulmonary infarction. (C) Additional contrast CT showing a massive thrombus in the main trunk of the right pulmonary artery. (D) Lung perfusion scan showing disruption in blood flow to the right lung.
Transbronchial biopsy of the infiltrates in the right lung showed coagulative necrosis, suggesting a pulmonary embolism (Figure 1B). Enhanced CT identified a large thrombus in the main trunk of the right pulmonary artery (Figure 1C), and lung perfusion scintigraphy showed no blood flow in the right lung (Figure 1D). The patient was diagnosed with pulmonary infarction due to pulmonary embolism. Treatment with direct oral anticoagulants (DOACs) was initiated instead of thrombolytic therapy and thrombectomy as the patient was hemodynamically stable and did not require oxygen supply.
After starting treatment for pulmonary infarction, chest CT scans performed every 6 months showed no obvious cavitary lesions or bronchiectasis. However, the chest CT scan performed 2 years later revealed new nodules with cavities in the right upper lobe (Figure 2A) The thrombus remained, with developed collateral blood vessels (Figure 2B). Bronchoscopy identified Mycobacterium avium in the bronchoalveolar lavage fluid and tissue culture from the right upper lobe. The diagnostic criteria for NTM pulmonary disease were met based on CT and bronchoscopy findings. Drug susceptibility testing for NTM was not performed due to resource limitations, so susceptibility was unknown. The patient was diagnosed with NTM pulmonary disease, complicating pulmonary infarction, and treated with rifampicin, clarithromycin, and ethambutol. After 2 years of oral treatment, some nodules in the right lung shrank, whereas the cavities persisted. The treatment response was slow. However, there was no worsening of imaging findings or subjective symptoms, so medication was discontinued after 2 years of treatment. Sputum cultures remained negative throughout the treatment period, and there was no radiological deterioration or microbiology to suggest recurrence for more than 2 years after treatment completion.
Radiographic images taken 2 years after the first examination. (A) CT showing new nodules with cavities in the upper right lobe. (B) CT showing a residual thrombus in the main trunk of the right pulmonary artery.
Discussion
3
NTM are environmental organisms capable of causing opportunistic pulmonary disease when bacteria are inhaled from water sources or soil [1]. Host factors, including immunosuppressive conditions and lung structural abnormalities, such as COPD and bronchiectasis, significantly contribute to the risk of NTM pulmonary disease [2]. A retrospective study reported that Chronic Thromboembolic Pulmonary Hypertension (CTEPH) may predispose individuals to NTM pulmonary disease, with a higher incidence in segments of the lung where the pulmonary artery is obstructed compared to healthy segments [3]. It has been suggested that the macrophage activity and interferon gamma may affect NTM susceptibility [4, 5]. In patients with pulmonary embolism, including those with CTEPH, chronic embolism‐induced blood flow disorders may contribute to the development of NTM. Restoration of blood flow by pulmonary endarterectomy (PEA) may enhance immune response and improve treatment outcomes for NTM in these patients [3]. Therefore, NTM pulmonary disease may complicate chronic pulmonary embolism, with interruption of pulmonary blood flow potentially leading to a poor response to treatment.
Author Contributions
Yasuyuki Hayashi and Akihiko Sokai conceptualised and drafted the initial manuscript. All authors reviewed and edited the manuscript.
Consent
The authors declare that written informed consent was obtained for the publication of this manuscript and accompanying images using the consent form provided by the Journal.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1C. L. Tzou , M. A. Dirac , A. L. Becker , et al., “Association Between Mycobacterium Avium Complex Pulmonary Disease and Mycobacteria in Home Water and Soil,” Annals of the American Thoracic Society 17 (2020): 57–62, 10.1513/Annals ATS.201812-915OC.31644315 PMC 6944351 · doi ↗ · pubmed ↗
- 2M. A. Dirac , K. L. Horan , D. R. Doody , et al., “Environment or Host?: A Case‐Control Study of Risk Factors for Mycobacterium avium Complex Lung Disease,” American Journal of Respiratory and Critical Care Medicine 186 (2012): 684–691, 10.1164/rccm.201205-0825 OC.22859521 PMC 5450977 · doi ↗ · pubmed ↗
- 3F. Kuroda , N. Tanabe , H. Igari , et al., “Nontuberculous Mycobacterium Diseases and Chronic Thromboembolic Pulmonary Hypertension,” Internal Medicine 53 (2014): 2273–2279, 10.2169/internalmedicine.53.2558.25318788 · doi ↗ · pubmed ↗
- 4P. Sexton and A. C. Harrison , “Susceptibility to Nontuberculous Mycobacterial Lung Disease,” European Respiratory Journal 31 (2008): 1322–1333, 10.1183/09031936.00140007.18515557 · doi ↗ · pubmed ↗
- 5W. J. Koh , O. J. Kwon , E. J. Kim , K. S. Lee , C. S. Ki , and J. W. Kim , “NRAMP 1 Gene Polymorphism and Susceptibility to Nontuberculous Mycobacterial Lung Diseases,” Chest 128 (2005): 94–101, 10.1378/chest.128.1.94.16002921 · doi ↗ · pubmed ↗