A Whispering Heart: Viral Myocarditis Hiding in Plain Sight
Khaja Shafiuddin, Noor Sadiq Syed, Trang Singhal

TL;DR
A 14-year-old girl with celiac disease developed severe heart issues from myocarditis and made a full recovery after intensive treatment.
Contribution
This case highlights myocarditis as a rare but critical cause of sudden heart block and shock in pediatric patients.
Findings
A 14-year-old girl with celiac disease developed fulminant myocarditis leading to complete heart block and cardiogenic shock.
The patient recovered after treatment with inotropic support, hyperkalemia management, and ECMO.
The case emphasizes the need for high clinical suspicion of myocarditis in pediatric patients with conduction abnormalities and shock.
Abstract
We present the case of a 14-year-old girl with a background of celiac disease and no other significant medical history who developed acute complete heart block and cardiogenic shock secondary to fulminant myocarditis. She presented with persistent vomiting and lethargy. An electrocardiogram (ECG) revealed ST-segment elevation. A bedside echocardiogram revealed global hypokinesia. She was found to be in complete heart block and showed biochemical evidence of multi-organ hypoperfusion. Management included emergency inotropic support, hyperkalemia treatment, and extracorporeal membrane oxygenation (ECMO). She made a remarkable recovery, with near normalization of cardiac function and resolution of arrhythmias. This case highlights the importance of high clinical suspicion for myocarditis in pediatric patients presenting with conduction abnormalities and shock.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
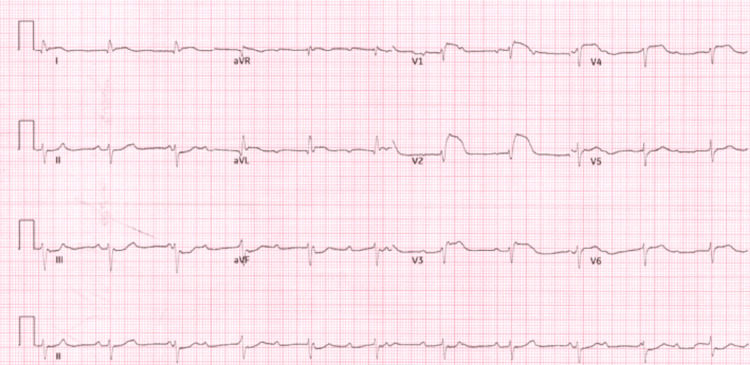 Figure 1
Figure 1 Figure 2
Figure 2| Parameter | Result | Unit | Normal Range |
| pH | 7.45 | - | 7.35 - 7.45 |
| pCO₂ | 2.3 | kPa | 4.7 - 6.0 |
| pO₂ | 12.3 | kPa | 10 - 13 |
| Sodium (Na⁺) | 129 | mmol/L | 135 - 145 |
| Potassium (K⁺) | 7.5 | mmol/L | 3.5 - 5.0 |
| Calcium (Ca²⁺) | 1.25 | mmol/L | 2.1 - 2.6 |
| Glucose (Glu) | incalc | mmol/L | 3.9 - 5.8 |
| Lactate (Lac) | 8.7 | mmol/L | < 2.0 |
| Total Hb (tHb) | — | - | 120 - 180 g/L |
| Oxyhemoglobin (O₂Hb) | 96.7 | % | 95 - 98% |
| Carboxyhemoglobin (COHb) | 1.7 | % | < 2% |
| Methemoglobin (MetHb) | 0.6 | % | < 1.5% |
| Deoxyhemoglobin (HHb) | 1.0 | % | < 2% |
| Oxygen Saturation (sO₂) | 99.0 | % | > 94% |
| Base Excess (BE(B)) | -9.4 | mmol/L | -2 to +2 |
| Bicarbonate (HCO₃⁻(c)) | 11.8 | mmol/L | 22 - 28 |
| Standard Bicarb (HCO₃⁻ std) | 17.6 | mmol/L | 22 - 28 |
| Hematocrit (Hct(c)) | 41 | % | 36 - 50% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsViral Infections and Immunology Research · Viral gastroenteritis research and epidemiology · Whipple's Disease and Interleukins
Introduction
Myocarditis is a rare but potentially life-threatening inflammatory condition of the myocardium, particularly in the pediatric population. Clinical presentation can range from mild symptoms to fulminant heart failure and arrhythmias. Complete heart block (CHB) is an uncommon manifestation but may signify severe myocardial involvement. Early diagnosis and prompt multidisciplinary management are crucial to improving outcomes [1-3].
Case presentation
A 14-year-old girl with known celiac disease presented to the emergency department with a one-day history of persistent vomiting (approximately 15-20 episodes), profound fatigue, and clamminess. She reported a brief viral illness two weeks prior to presentation. On examination, she appeared pale, hypotensive (blood pressure 85/42 mmHg), and bradycardic (heart rate 40-60 bpm), with prolonged capillary refill and weak peripheral pulses. She was alert and oriented (Glasgow Coma Scale (GCS) 15).
Electrocardiography (ECG) (Figure 1) revealed CHB with ST-elevation in leads V1-V4 and ST-depression in the inferior leads. Point-of-care echocardiography (Figure 2) demonstrated global hypokinesia. Capillary blood (Table 1) gas showed compensated metabolic acidosis (pH 7.45, base excess -9.4, bicarbonate (HCO_3_) 11.8), elevated lactate (8.7 mmol/L), hyperkalemia (K+ 7.5 mmol/L), and hyponatremia (Na+ 129 mmol/L). Cardiac biomarkers were markedly elevated, with a troponin I level of 8506 ng/L.
Electrocardiograph demonstrating ST-elevation in leads V1-V4 and ST-depression in the inferior leads
Point-of-care ultrasound demonstrating global hypokinesia
Initial management included calcium gluconate, insulin-dextrose infusion, magnesium sulfate, and low-dose peripheral adrenaline infusion. An arterial line was placed, and arrangements were made for urgent transfer to a tertiary pediatric cardiology center via the Embrace transport team. Following further assessment, she was diagnosed with fulminant viral myocarditis. Due to severe biventricular dysfunction and ongoing cardiogenic shock, veno-arterial extracorporeal membrane oxygenation (ECMO) was initiated. During ECMO support, the patient regained sinus rhythm, and echocardiographic parameters progressively improved. A residual atrial septal defect (iatrogenic from ECMO) was noted. She recovered well and was discharged with a loop recorder in situ and on a stable regimen of bisoprolol and spironolactone.
Discussion
This case illustrates the importance of maintaining a high index of suspicion for myocarditis in children presenting with nonspecific systemic symptoms and cardiac conduction abnormalities. Myocarditis may present subtly, but fulminant forms can cause rapid hemodynamic compromise. Electrocardiographic abnormalities such as ST elevation and CHB, especially when coupled with elevated cardiac enzymes and echocardiographic evidence of ventricular dysfunction, should prompt urgent intervention [1,3,4].
In pediatric populations, myocarditis is most often post-viral in etiology. The pathophysiology involves myocardial inflammation and necrosis, leading to impaired contractility and arrhythmogenesis. Timely initiation of mechanical circulatory support such as ECMO can be life-saving and has been associated with favorable neurological and cardiac outcomes [5,6].
The diagnostic workup for suspected myocarditis should include ECG, cardiac biomarkers, echocardiography, and MRI when feasible. Endomyocardial biopsy remains the gold standard but is often reserved for select cases [2,7]. Long-term follow-up is essential to monitor for recurrent arrhythmias or late-onset cardiomyopathy [3,8].
Conclusions
Acute fulminant myocarditis should be considered in any child presenting with arrhythmia, shock, or unexplained cardiac dysfunction. Prompt ECG interpretation and bedside echocardiography are essential for diagnosis. Early multidisciplinary intervention, including ECMO, can significantly improve patient outcomes and facilitate complete recovery.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases Eur Heart J Caforio AL Pankuweit S Arbustini E 263626482636-48, 2648 a-2648 d 3420132382482810.1093/eurheartj/eht 210 · doi ↗ · pubmed ↗
- 2Myocarditis Lancet Sagar S Liu PP Cooper LT Jr 73874737920122218586810.1016/S 0140-6736(11)60648-XPMC 5814111 · doi ↗ · pubmed ↗
- 3Update on myocarditis J Am Coll Cardiol Kindermann I Barth C Mahfoud F 7797925920122236139610.1016/j.jacc.2011.09.074 · doi ↗ · pubmed ↗
- 4Myocarditis N Engl J Med Cooper LT Jr 1526153836020091935740810.1056/NEJ Mra 0800028 PMC 5814110 · doi ↗ · pubmed ↗
- 5Extracorporeal membrane oxygenation in cardiopulmonary disease in adults J Am Coll Cardiol Abrams D Combes A Brodie D 276927786320142481448810.1016/j.jacc.2014.03.046 · doi ↗ · pubmed ↗
- 6Enalapril in infants with single ventricle: results of a multicenter randomized trial Circulation Hsu DT Zak V Mahony L 33334012220102062511110.1161/CIRCULATIONAHA.109.927988 PMC 3692364 · doi ↗ · pubmed ↗
- 7Diagnosis of myocarditis: death of Dallas criteria Circulation Baughman KL 5935951132006 https://www.ahajournals.org/doi/10.1161/circulationaha.105.5896631644973610.1161/CIRCULATIONAHA.105.589663 · doi ↗ · pubmed ↗
- 8Myocarditis: current trends in diagnosis and treatment Circulation Magnani JW Dec GW 87689011320061647686210.1161/CIRCULATIONAHA.105.584532 · doi ↗ · pubmed ↗