Bilateral cavernous sinus and left dural sigmoid sinus thrombosis associated with extreme exertion: a case report
Chong Wern-Yih, Chan Jan-Bond, Menon Sudha, Abu Norlelawati, Ismail Shatriah

TL;DR
A 20-year-old military trainee developed rare sinus thrombosis after intense exercise, but recovered fully with treatment.
Contribution
This case report highlights septic cavernous sinus thrombosis in an immunocompetent young adult linked to extreme physical exertion.
Findings
The patient showed rapid improvement in visual acuity and proptosis after intravenous antibiotics and corticosteroids.
Full ocular motility was restored in the right eye with minor residual issues in the left eye.
No recurrence or long-term complications were observed at 3 months follow-up.
Abstract
Septic cavernous sinus thrombosis is a rare but often debilitating and potentially fatal disease. We describe a case of bilateral orbital cellulitis with rapidly progressing cavernous sinus thrombosis and left sigmoidal sinus thrombosis in an immunocompetent 20-year-old military man who had undergone intensive physical training. The patient presented with rapid painful swollen left eye for 2 days. The examination results were gross proptosis with total ophthalmoplegia. He was treated with intravenous antibiotics and corticosteroid. At 1 week, visual acuity improved to 20/20 OU, with a normal intraocular pressure. There was a significant improvement in proptosis. The ocular motility of the right eye was fully restored, with slight residual ophthalmoplegia in the left eye. There was no residual illness or recurrence of illness at 3 months’ follow-up.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
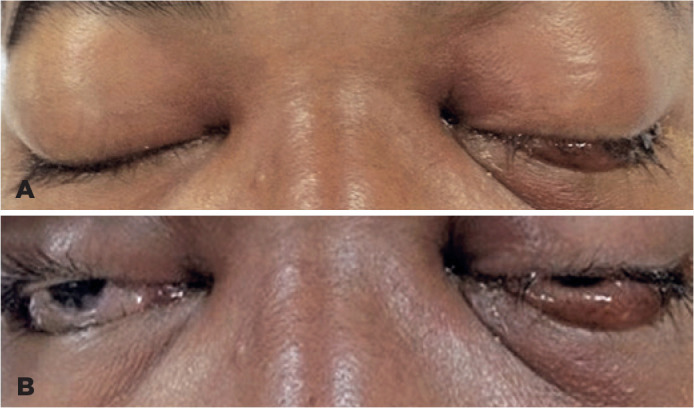 Figure 1
Figure 1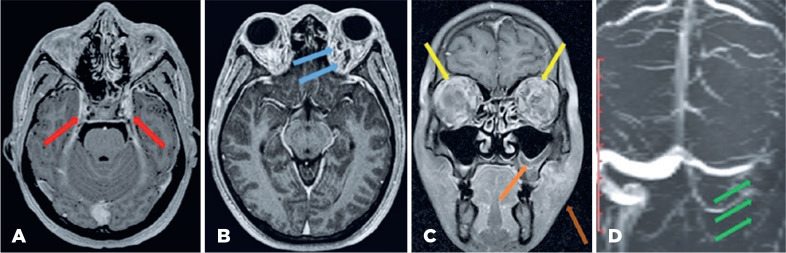 Figure 2
Figure 2 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCerebral Venous Sinus Thrombosis · Sinusitis and nasal conditions · Ocular Diseases and Behçet’s Syndrome
INTRODUCTION
Cavernous sinus thrombosis (CST) has become an uncommon condition with the availability of antibiotics. The most common causes of CST are sinusitis, otitis, and odontogenic and facial skin infections^(1)^. In contrast to common belief, athletes and sportsmen are at increased risk of infections, especially during periods of heavy training^(2-3)^. We describe a case of rapidly progressing CST with left sigmoidal sinus involvement in an immunocompetent young man who had undergone intensive physical training.
CASE REPORT
A 20-year-old healthy military man complained of a sudden, rapidly progressing painful and swollen left eye of 2 days’ duration. It was associated with blurring of vision, diplopia, and swelling of the left cheek. The patient had undergone intensive training in a military camp for 5 days, consisting of a total of 8 hours of running, marching, and physical strength training.
The patient was restless and febrile. The left maxillary area was swollen, tender, and warm. The neurological examination was normal except for a positive Kernig’s sign. Examinations of other systems were not suggestive of infection.
Visual acuity was 20/30 OD and 20/60 OS. There was gross proptosis bilaterally (23 mm OD and 24 mm OS). There was total ophthalmoplegia with swollen and chemotic conjunctiva (Figure 1). The intraocular pressure was elevated (24 mmHg OD and 30 mmHg OS). No relative afferent pupillary defect was observed. The anterior and posterior segment examinations were normal.
Figure 1(A, B). Photographs on presentation showing bilateral gross proptosis and chemosis with left periorbital swelling.
The total white cell count was elevated to 23,000/µl, with predominantly neutrophils (86%). Blood culture was repeated twice and grew methicillin-sensitive Staphylococcus aureus. Lumbar puncture showed normal glucose and protein levels with negative culture results. Screening for thrombophilia, which included protein C, protein S, anti-thrombin III, activated protein C resistance, and lupus anticoagulant screening, was negative.
Contrast-enhanced computed tomography (CECT) showed bilateral prominent superior ophthalmic veins, proptosis, and frontal soft tissue swelling with an absence of loculation. However, no sign of distended cavernous sinus with a non-fat density-filling defect was observed.
Magnetic resonance imaging (MRI) revealed proptosis of both eyes with diffuse, symmetrical soft tissue thickening and areas of enhancement with engorgement of orbital vessels and inflammatory fat stranding involving the preseptal, postseptal, intraconal, and extraconal spaces. Magnetic resonance venography (MRV) did not show flow-related enhancement at the left sigmoid sinus. T2-weighted MRI showed a persistent filling defect within the cavernous sinus on both sides and the left sigmoid sinus. The sphenoid, left maxillary, and left ethmoidal sinuses showed mucosal thickening with an air-fluid level (Figure 2).
Figure 2(A) Magnetic resonance imaging (MRI) showed features suggestive of bilateral cavernous sinus thrombosis (red arrow), (B) distended superior ophthalmic vein (blue arrow), (C) bilateral orbital cellulitis (yellow arrow), left maxillary sinusitis (orange arrow), and left cheek soft tissue swelling (brown arrow), (D) left sigmoid dural sinus thrombosis (green arrow).
A diagnosis of bilateral orbital cellulitis and CST with evidence of left sigmoid sinus thrombosis complicated by sphenoid, left ethmoidal, and maxillary sinusitis was made. The patient was started on IV ceftriaxone 2 g twice daily, IV cloxacillin 1 g 6 hourly, IV hydrocortisone 50 mg 8 hourly, and IV heparin 6000 IU 6 hourly. Gutta moxifloxacin 4 hourly, gutta timolol 12 hourly, and gutta hydroxypropylmethylcellulose 6 hourly were prescribed for both eyes.
At 1-week, visual acuity improved to 20/20 OU, with a normal level of intraocular pressure. There was a significant improvement in proptosis. Ocular motility of the right eye was fully restored, with slight residual ophthalmoplegia in the left eye (Figure 3). There was no residual illness or recurrence of illness at 3 months’ follow-up.
Figure 3. Photographs after completion of treatment. Nine-gaze photographs showed resolution of proptosis and ophthalmoplegia.
DISCUSSION
CST is the rarest form of dural venous sinus thrombosis, with a mortality rate of up to 30% and a morbidity rate as high as 22%^(2)^. The most common causes are sinusitis, otitis, and odontogenic and facial skin infections^(1)^ due to the close proximity of the structures^(3)^. Our case report showed an increased risk of infection in a healthy individual due to extreme physical exertion.
It has been reported that intensive training and overtraining are associated with immunodepression and susceptibility to infection^(2,3)^. The “inverted J hypothesis” in exercise immunology suggested that disease susceptibility increased in sedentary and over-trained subjects in comparison with subjects who underwent regulated, moderate training. Depression of natural killer cell function, reduction in expression of toll-like receptors, and increased release of cortisol and proinflammatory cytokines, such as tumor necrosis factor, interleukin-1b, and interleukin-6, are well-documented mechanisms that may have contributed to the immunocompromised state of our patient^(4)^.
Another possible mechanism of the rapid progression of CST to intracranial thrombosis is the rebalanced hemostatic state, simultaneously causing hypercoagulability and enhanced fibrinolysis induced by extreme physical exertion. Hypercoagulability appears to persist longer, from a few hours to a day, than fibrinolytic activities after strenuous training^(5)^. Hence, we presumed that our patient was likely in a prothrombic state, which favored intracranial thrombus formation.
Staphylococcus aureus is the most common organism isolated in CST. Other organisms, including Streptococcus, fungi, Enterobacteriaceae, and anaerobes, have also been reported^(6)^. Predisposed to an increased risk of in fection associated with extreme physical exertion^(4)^, our patient developed methicillin-sensitive S. aureus septicemia from uncomplicated sinusitis and progressed to bilateral CST with left sigmoid sinus involvement. Our case is similar to the cases described by van der Poel et al., who reported that most of their patients recovered without any permanent deficits^(7)^.
High-resolution CECT provides superb bone-air soft tissue details of the orbit and sinuses. CST may present as multiple irregular filling defects in the cavernous sinus on CECT. Our patient had normal CECT scan findings, similar to the report of Komatsu et al.^(8)^. Thus, the managing clinician should have a high index of suspicion towards the diagnosis of CST based on clinical presentation, even if the CECT scan is normal.
High-resolution MRI visualizes the enlargement of the CST as filling defects over time. Thin-slice gradient recalled echo sequences with gadolinium contrast have been shown to be more sensitive than routine MRI pulse sequences for detection of filling defects in the cavernous sinus^(9)^. MRV is helpful when the clinician suspects that dural sinuses are involved. In our case, MRI and MRV mapped out the complete extension of the CST in detail.
CST remains a life-threatening condition. Our case is an example of intensive physical training as a possible cause of thrombosis in a young patient with a rapid onset of intracranial thrombosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Weerasinghe D Lueck CJ. Septic cavernous sinus thrombosis: Case report and review of the literature Neuroophthalmology 20164062632762792841710.1080/01658107.2016.1230138 PMC 5120738 · doi ↗ · pubmed ↗
- 2Desa V Green R. Cavernous sinus thrombosis: current therapy J Oral Maxillofac Surg 2012709208520912232617310.1016/j.joms.2011.09.048 · doi ↗ · pubmed ↗
- 3Kiddee W Preechawai P Hirunpat S. Bilateral septic cavernous sinus thrombosis following the masticator and parapharyngeal space infection from the odontogenic origin: a case report J Med Assoc Thai 20109391107111120873087 · pubmed ↗
- 4Romeo J Wärnberg J Pozo T Marcos A. Physical activity, immunity and infection Proc Nutr Soc 20106933903992056952210.1017/S 0029665110001795 · doi ↗ · pubmed ↗
- 5Kicken CH Miszta A Kelchtermans H De Laat B. Hemostasis during extreme exertion Semin Thromb Hemost 20184476406502972789210.1055/s-0038-1639502 · doi ↗ · pubmed ↗
- 6Lim LH Scawn RL Whipple KM Oh SR Lucarelli MJ Korn BS Spontaneous superior ophthalmic vein thrombosis: a rare entity with potentially devastating consequences Eye (Lond)20142833483512435783810.1038/eye.2013.273PMC 3965813 · doi ↗ · pubmed ↗
- 7van der Poel NA Mourits MP de Win MM Coutinho JM Dikkers FG. Prognosis of septic cavernous sinus thrombosis remarkably improved: a case series of 12 patients and literature review Eur Arch Otorhinolaryngol 20182759238723952999838510.1007/s 00405-018-5062-9PMC 6096574 · doi ↗ · pubmed ↗
- 8Komatsu H Matsumoto F Kasai M Kurano K Sasaki D Ikeda K. Cavernous sinus thrombosis caused by contralateral sphenoid sinusitis: a case report Head Face Med 20139192349746610.1186/1746-160X-9-9PMC 3605125 · doi ↗ · pubmed ↗