Cost-effectiveness of biomarker-directed toripalimab plus chemotherapy for previously untreated extensive-stage small-cell lung-cancer in China
Shuo Kang, Shan Zhao, Xiaohui Wang, Zhenhua Pan

TL;DR
This study evaluates whether using biomarker testing to guide treatment with toripalimab and chemotherapy is cost-effective for treating a type of lung cancer in China.
Contribution
The study introduces a cost-effectiveness analysis of biomarker-directed treatment for extensive-stage small-cell lung cancer in the Chinese healthcare context.
Findings
ITH-testing directed therapy provided 0.14 and 0.29 additional QALYs compared to other treatments.
The incremental cost-effectiveness ratios were below China's willingness-to-pay threshold.
The probability of ITH-directed therapy being cost-effective was 61%.
Abstract
With or without biomarker-directed toripalimab plus chemotherapy could bring significant clinical benefit and acceptable safety profile compared with chemotherapy as first-line treatment for patients with extensive-stage small-cell lung-cancer (ES-SCLC) were demonstrated in EXTENTORCH trial. However, its cost-effective remains uncleared. The current analysis aimed to evaluate the economic value of intratumor heterogeneity (ITH) testing directed toripalimab plus chemotherapy as first-line treatment for patients with ES-SCLC from the Chinese health-care system perspective. A mathematical decision model-based cost-effectiveness analysis, A pharmacoeconomic decision model was developed to simulate 3-week patients transition in 20-year time horizon to access the cost-effectiveness of three competing first-line treatments among ITH-testing directed toripalimab plus chemotherapy,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
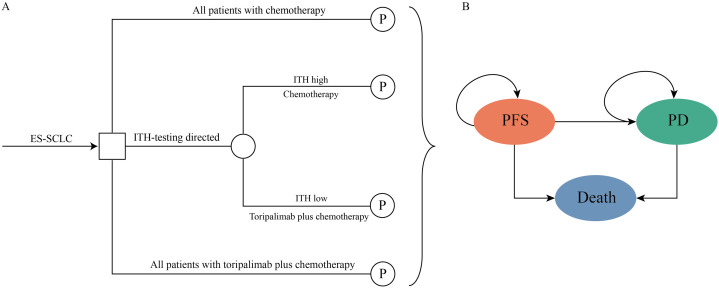 Fig 1
Fig 1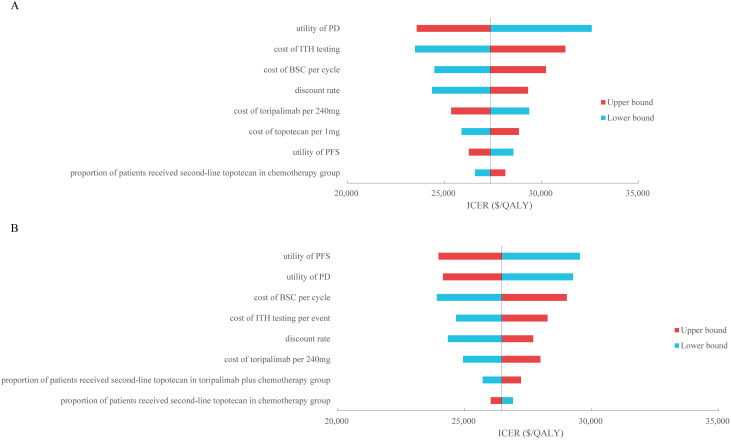 Fig 2
Fig 2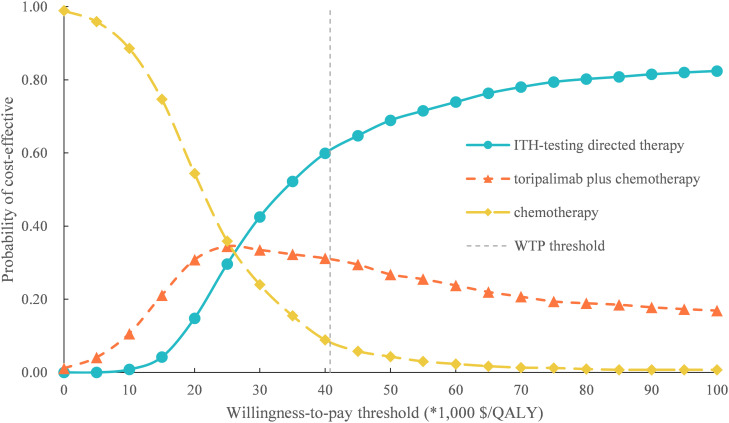 Fig 3
Fig 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Research Studies · Neuroendocrine Tumor Research Advances · Cancer therapeutics and mechanisms
Introduction
Lung cancer has the highest incidence and mortality of all malignancy worldwide [1]. Small-cell lung-cancer (SCLC) is the most aggressive subtype of all lung cancer according to the histological type. Unfortunately, approximately 66% of SCLC patient had progressed to the extensive-stage SCLC (ES-SCLC) with metastasis at the initial diagnosis [2,3], which with the especially poor prognosis and 5-year survival rate was less than 7% [4]. The chemotherapy of platinum plus etoposide was the standard first-line treatment over past 30 years which achieved good initial results but rapidly progressed and resulting the limited median overall survival was only 10 months [5–7].
Recently, immune checkpoint inhibitors (ICIs) could reactive the anti-tumor function of T cells by inhibiting the programmed cell death-1 (PD-1) and programmed cell death receptor ligand-1 (PD-L1) pathway [8–10]. The addition of ICIs such as atezolizumab, durvalumab, and serplulimab to first-line platinum plus etoposide demonstrated the clinical and safety profile compared with chemotherapy alone [11–13]. Toripalimab, is a novel immunoglobulinG4PD-1 blocking antibody, the recent EXTENTORCH trial demonstrated that toripalimab plus chemotherapy could significantly reduce the risk of disease progression or death by 33% (hazard ratio (HR), 0.67, 95% confidence interval: 0.54–0.82) and the risk of death by 20% (HR, 0.80, 95% confidence interval: 0.65–0.98) for untreated ES-SCLC patients compared with chemotherapy alone. Simultaneously, EXTENTORCH trial found that the biomarker of intratumor heterogeneity (ITH) layered selected therapy could further enhance the clinical value of toripalimab plus chemotherapy compared with chemotherapy alone, which could prolong the median progression-free survival (PFS) and median overall survival (OS) for ITH-low patient [14].
Despite toripalimab plus chemotherapy demonstrated clinical benefit compared with chemotherapy alone, we need pay more attention to its cost-effective benefits with the widely used in the clinical practice in resource-limited countries such as China, although the price of toripalimab has significantly decreased since its initial launch, it was still relatively expensive compared with chemotherapy. The aim of the current analysis was to evaluate the cost-effectiveness of adding toripalimab to first-line chemotherapy for patients with previously untreated ES-SCLC from the Chinese health-care system perspective.
Methods
Analytical overview and model structure
A mathematical model combining the decision tree process and partitioned survival model (PSM) was established to evaluate the cost-effectiveness of biomarker-directed toripalimab plus chemotherapy for patients with untreated ES-SCLC. The decision tree displayed a clear process of the decision-making of the three strategies of first-line therapy of ES-SCLC (Fig 1A), among patients used chemotherapy or toripalimab plus chemotherapy without biomarker detection, and biomarker-directed strategy, which patients with ITH low or high used toripalimab plus chemotherapy or chemotherapy alone, respectively. The PSM was developed to simulate the disease course of the ES-SCLC in the hypothetical cohort (Fig 1B), the PSM was constituted by three mutually exclusive health states: PFS, progressed disease (PD), and death. All patients were at PFS state when entered the model, and the patients could not return to the previous health states. The PSM simulated every 3-week patients transition in 20-year time horizon. Patients would progress to another health state or keep at the current health state at the end of each cycle.
The structure of the mathematical decision model.ES-SCLC, extensive-stage small-cell lung-cancer; ITH, intratumor heterogeneity; PFS, progression-free survival; PD, progressed disease.
Total costs, life-years (LYs), quality-adjusted life-years (QALYs) were the model outputs, costs and utility values which used to estimate the QALYs were discounted at an annual rate of 5% according to the Chinese guidelines for pharmacoeconomic evaluations [15]. Costs values were shown in 2023 US dollars (US 1 = CNY 7.047), incremental cost-effectiveness ratio (ICER) was calculated by the following formula: ICER=(C_1_-C_2_)/(E_1_-E_2_), which presented as costs per additional QALY gained to judge the cost-effective of competing first-line treatment. Three times of per capita gross domestic product (GDP) of China in 2024 (40,761/QALY) was set to be the WTP threshold in line with the WHO recommendations [16–18]. This research did not involve any human or animal subjects, thus ethical approval and consent to participate were not required.
Clinical data
The clinical survival and safety data were gathered from the EXTENTORCH trial. Individual time-to-event data were reconstructed by using the standard algorithm developed by Guyot et al [19], then the individual patient data were used to fit the following parametric survival model among, Exponential, Gamma, Generalized Gamma, Weibull, Log-normal, Log-logistic, Gompertz [20]. Goodness between the fitting survival model and the Kaplan-Meier (K-M) curves reported in the EXTENTORCH trial was based on the visual inspection and Akaike information criterion (AIC), AIC values and best fitted models were performed in Supplementary Table 1. The estimated survival parameters were shown in Table 1. After the disease progressed, patients would receive the standard second-line treatment of topotecan, and the proportion of patients received second-line therapy in the three strategies were gathered from the EXTENTORCH trial.
Table 1: Survival model parameters fitting to the PFS and OS data from the EXTENTORCH trial.
Cost and utility values
Only direct medical costs were considered in the current analysis because the evaluate perspective was the Chinese health-care system, costs values included the cost of anti-cancer regimens, routine follow-up, best supportive care, end-of-life care, and management of treatment-related serious adverse events (SAEs, grade≥3), typical patient with weight of 65 kg and height of 1.64m, resulting in the body surface area (BSA) of 1.72m^2^ [21], was used to calculate the dosage of the chemotherapy, all cost values were obtained from the local bid-winning price or previously literatures.
The health utility values which reflecting health state preference that affected by race, region, and religious beliefs were obtained from the related studies and the utility values were usually on the scale of 0–1, the utility values of the PFS, PD, and Death health state in the current study were set to be 0.673, 0.473 and 0 [22], respectively, the disutility values caused by the SAEs were also considered in our model. All model parameters were shown in Table 2.
Table 2: Model inputs: base-line values and ranges for sensitivity analyses.
Sensitivity analyses
Sensitivity analyses included one-way and probabilistic sensitivity analyses (PSA) were conducted to evaluate the robustness of the model results when model parameters were changed. In one-way sensitivity analyses, parameters were changed one-by-one based on their lower and upper bound to identify which was the most influence parameter of the model results, the range of the parameter was set as 95% confidence interval or ±25% of the base-line value (when the 95% confidence interval was not available). The results of the one-way sensitivity analyses were presented by the Tornado diagram. For PSA, Monte Carlo simulation of 1,000 iterations was developed by repeatedly sampling the model parameters from the statistical distributions, where Gamma distribution was used for cost values, Beta distribution was used for utility and disutility values, incidence rates proportions and probabilities [29], the results of PSA were presented by the cost-effectiveness acceptability curves (CEACs).
Results
Base-case results
From Chinese health-care system perspective, in 20-year time horizon, ITH testing directed treatment could bring additional 0.14 QALYs and 0.29 QALYs with the acceptable marginal costs of 7778.18 compared with toripalimab plus chemotherapy and chemotherapy alone, resulting in the ICER of 26,461.46/QALY, respectively, which were lower than the Chinese WTP threshold of $40,761.60 per additional QALY gained, the base-case results were shown in Table 3.
Table 3: Base-case results.
Sensitivity analyses results
In one-way sensitivity analyses, for ITH-testing directed treatment versus toripalimab plus chemotherapy, the utility of PD was the main driver of the model outcomes (Fig 2A), for ITH-testing directed treatment versus chemotherapy alone, the utility of PFS had the substantial influence of the model results (Fig 2B). For the two comparisons, the ICERs were always lower than the WTP threshold of $40,761/QALY whatever each parameter changed in the threshold range, the results of one-way sensitivity analyses were robustness.
Tornado diagram of one-way sensitivity analyses of (A) ITH-testing directed treatment versus toripalimab plus chemotherapy and (B) ITH-testing directed treatment versus chemotherapy.PFS, progression-free survival; PD, progressed disease; ITH, intratumor heterogeneity; BSC, best supportive care; ICER, incremental cost-effectiveness ratio; QALY, quality-adjusted life-year.
For PSA, the probability of ITH-testing directed treatment, toripalimab plus chemotherapy, and chemotherapy alone could be considered cost-effective at the Chinese WTP threshold of 40,761/QALY (Supplementary Fig 1 and Supplementary Fig 2).
Cost-effectiveness acceptability curves of three competing first-line therapy.ITH, intratumor heterogeneity; WTP, willingness-to-pay; QALY, quality-adjusted life-year.
Discussion
Both oncologists and health-care decision makers were interested by the results of the clinical benefit of adding toripalimab to first-line chemotherapy for patients with previously untreated ES-SCLC in EXTENTORCH trial, simultaneously, ITH-testing results layered treatment option of toripalimab plus chemotherapy demonstrated superior clinical benefit compared to it in the intention-to-treat population. Although the price of toripalimab has been significant decline compared with initial launch, its price was still relatively expensive compared to chemotherapy, and its cost-effective was need to be clarified. The current analysis aimed to evaluate the cost-effectiveness of biomarker-directed toripalimab plus chemotherapy as first-line treatment for patients with ES-SCLC, the study has three competing therapies among all patients with toripalimab plus chemotherapy, all patients with chemotherapy, and patients with ITH-testing results directed treatment. In base-case analysis, ITH-testing directed treatment could bring additional health benefit compared with toripalimab plus chemotherapy and chemotherapy alone with the acceptable marginal cost, resulting in the ICER of 26,461.46/QALY, respectively, which lower than the WTP threshold of $40,761 per additional QALY gained, one-way sensitivity analyses suggested that the utility value of the health state was the main driver of the model results, PSA showed that the probability of ITH-testing directed treatment could be considered cost-effective was 61%, and to explore additional contexts, we conducted the price analysis, we found that when the price of toripalimab reduced 30% and 50%, the cost-effective probability of ITH-testing directed treatment was stabled at around 60%, these findings revealed that the ITH-testing directed treatment was likely to be the most cost-effective first-line treatment but sensitive to utility assumptions for patients with previously untreated ES-SCLC.
Notably, in the current analysis, the ITH testing method was Mutant-Allele Tumor Heterogeneity (MATH) method, which is a computational tool designed to quantify intratumor heterogeneity by analyzing the dispersion of variant allele frequencies (VAFs) across somatic mutation loci within tumor samples using high-throughput sequencing data, and the score of 29 was used as the boundary between high and low heterogeneity. In China, biomarker-informed precision decision-making was received growing emphasis in the management of malignant neoplastic diseases, and with widespread application in the clinical practice, it was critical for enhancing rational drug utilization and optimizing healthcare resource allocation efficiency. Our analysis conducted the economic evaluation based on potential clinical pathways, wherein the cost of ITH testing was gathered from the local charge, and the ITH testing method of MATH was feasibility for the clinical practice, the results of our analysis demonstrated the economic value of refined clinical pathway, which was valuable for health-care decision makers.
Several studies evaluated the cost-effectiveness of adding ICIs to first-line chemotherapy compared chemotherapy alone from the Chinese context, the analyses demonstrated that adding atezolizumab, durvalumab, or adebrelimab was unlikely to be the cost-effective first-line treatment due to the unfavorable ICERs with limited health benefit and unacceptable marginal cost [30–32], these finds were in line with the understanding with the lower economic conversion rate of the high-price innovative anti-cancer drug. The above issues were still the direction of health-care decision makers need to pay more attention to. Although the development of Chinese economy and decreased of the drug price, the cost-effective of the high-value treatment may be improved, the future potential market imbalance need to be monitored. As the innovation point of the current study, we also involved the ITH-testing directed treatment in our analysis, and we found that it was more cost-effective than the competing strategies which were not considered biomarkers for using toripalimab plus chemotherapy or chemotherapy alone, our findings were valuable for treatment decision based on the precise economic evaluation results for both oncologists and health-care decision makers.
Several limitations must be illustrated when the health-care decision making was based on our study results. First, long-time survival data beyond the follow-up period in the clinical trial which used to calculate the health benefit were extrapolated by fitting the parametric survival model, despite the potential bias may be caused between the model results and real-world data, this method was an inevitable limitation of the cost-effectiveness analysis for anti-cancer treatment. Second, some cost values such as the cost of routine follow-up, the cost of best supportive care were gathered from the published studies rather than real-world data, however, sensitivity analyses demonstrated the robustness of the model outputs when parameters were changed. Only direct medical costs were considered in the model due to the health-care system perspective was conducted in the current analysis, however, as the chronic disease management model for malignant tumor diseases continues to deepen and refine, with more rational measurement methods become widespread, indirect costs such as productivity loss expenses caused by the disease should be increasingly considered for inclusion in such research. Third, as the key parameter for evaluating the health benefit, health state utility values, which may be affected by ethnicity and religious were obtained from a foreign study, although the utility values were the main driver of the model results, one-way sensitivity revealed that the ICERs were always lower than the WTP threshold, the model results were robustness. Fourth, to ensure the simplicity of the model structure, the cost of management of grade 1/2 adverse events were excluded from the model, only the cost of management SAEs (Grade≥3) was considered in the model, however, only minimal influence of the model outcomes for these parameters in our analysis. Finally, other potential competing first-line ICIs plus chemotherapy treatment for patients with ES-SCLC were not included in the current analysis due to the absence of the head-to-head clinical study. Despite the above limitations, we believe our analysis findings reflected the clinical and economic outcomes of the three first-line treatments for patients with previously untreated ES-SCLC in Chinese context.
Conclusion
In conclusion, ITH-testing directed therapy could be considered the most cost-effective first-line option compared with toripalimab plus chemotherapy and chemotherapy alone for patients with previously untreated ES-SCLC from the Chinese health-care system perspective due to the acceptable ICER.
Supporting Information
S1 TableSummary of statistical goodness-of-fit of Kaplan-Meier curves in EXTENTORCH trial.(PDF)
S1 FigCost-effectiveness acceptability curves of three competing first-line therapy when the price of toripalimab reduced 30%.ITH, intratumor heterogeneity; WTP, willingness-to-pay; QALY, quality-adjusted life-year.(TIF)
S2 FigCost-effectiveness acceptability curves of three competing first-line therapy when the price of toripalimab reduced 50%.ITH, intratumor heterogeneity; WTP, willingness-to-pay; QALY, quality-adjusted life-year.(TIF)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Howlader N, Forjaz G, Mooradian MJ. The Effect of Advances in Lung-Cancer Treatment on Population Mortality. N Engl J Med. 2020;383:640–9.32786189 10.1056/NEJ Moa 1916623 PMC 8577315 · doi ↗ · pubmed ↗
- 2Thatcher N, Faivre-Finn C, Lorigan P. Management of small-cell lung cancer. Ann Oncol. 2005;16:ii 235–9.10.1093/annonc/mdi 70015958464 · doi ↗ · pubmed ↗
- 3Rudin CM, Brambilla E, Faivre-Finn C, Sage J. Small-cell lung cancer. Nat Rev Dis Primers. 2021;7(1):3. doi: 10.1038/s 41572-020-00235-0 33446664 PMC 8177722 · doi ↗ · pubmed ↗
- 4Megyesfalvi Z, Gay CM, Popper H, Pirker R, Ostoros G, Heeke S, et al. Clinical insights into small cell lung cancer: Tumor heterogeneity, diagnosis, therapy, and future directions. CA Cancer J Clin. 2023;73(6):620–52. doi: 10.3322/caac.21785 37329269 · doi ↗ · pubmed ↗
- 5Früh M, De Ruysscher D, Popat S. Small-cell lung cancer (SCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2013;24(6):vi 99–105.10.1093/annonc/mdt 17823813929 · doi ↗ · pubmed ↗
- 6Rudin CM, Giaccone G, Ismaila N. Treatment of Small-Cell Lung Cancer: American Society of Clinical Oncology Endorsement of the American College of Chest Physicians Guideline. J Oncol Pract. 2016;12(1):83–6. doi: 10.1200/JOP.2015.008201 29424581 · doi ↗ · pubmed ↗
- 7Rossi A, Di Maio M, Chiodini P, Rudd RM, Okamoto H, Skarlos DV, et al. Carboplatin- or cisplatin-based chemotherapy in first-line treatment of small-cell lung cancer: the COCIS meta-analysis of individual patient data. J Clin Oncol. 2012;30(14):1692–8. doi: 10.1200/JCO.2011.40.4905 22473169 · doi ↗ · pubmed ↗
- 8Ribas A, Wolchok JD. Cancer immunotherapy using checkpoint blockade. Science. 2018;359(6382):1350–5. doi: 10.1126/science.aar 4060 29567705 PMC 7391259 · doi ↗ · pubmed ↗