Utility of ABI and API Versus CTA to Identify Surgically Significant Arterial Injury After Lower Extremity Trauma in a LMIC
Rubinette Robbertze, Megan Lubout, Daniel Nicholas Prince, Isabella Margaretha Joubert, Maeyane S. Moeng

TL;DR
This study shows that ABI and API can reliably screen for arterial injuries in trauma patients, reducing the need for unnecessary CT scans in South Africa.
Contribution
The study provides evidence supporting the use of ABI and API as reliable screening tools to avoid overuse of CTA in trauma patients with suspected lower extremity vascular injury.
Findings
ABI and API had 100% sensitivity and 100% NPV for detecting surgically significant arterial injuries.
CTA showed higher PPV (69.2%) compared to ABI/API (28.1%–35.9%).
Neither ABI nor API missed any surgically significant arterial injuries in the study cohort.
Abstract
South Africa faces a high burden of trauma‐related vascular injury. Prompt diagnosis and management are crucial to limit morbidity and mortality. Literature recommends a thorough vascular examination of at‐risk patients. Ankle brachial index (ABI) and arterial pressure index (API) are considered reliable screening tools for lower extremity vascular injury (LEVI) in the correct clinical scenario. Patients with an abnormal ABI/API warrant diagnostic imaging with computed tomography angiography (CTA). However, recent international literature demonstrates a trend toward potential CTA overuse in the work up for LEVI, when the internationally recommended vascular injury work‐up guidelines are not followed correctly. To assess the reliability of ABI/API in trauma patients with suspected LEVI as a screening tool to safely avoid unnecessary CTA. A retrospective cohort study of all lower…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
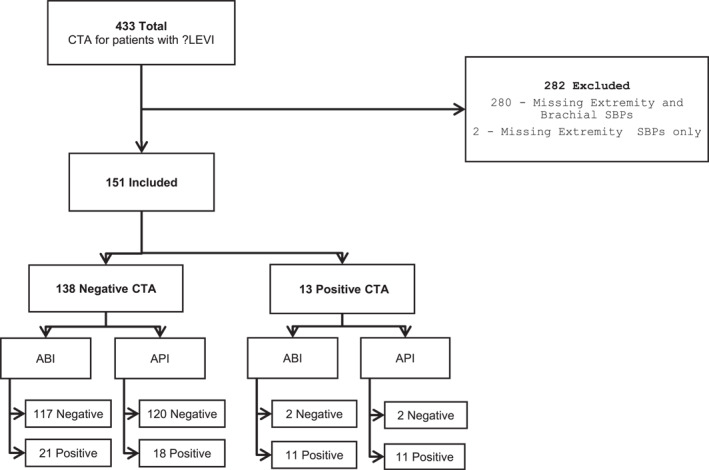 FIGURE 1
FIGURE 1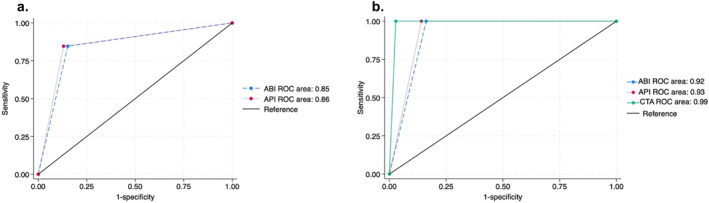 FIGURE 2
FIGURE 2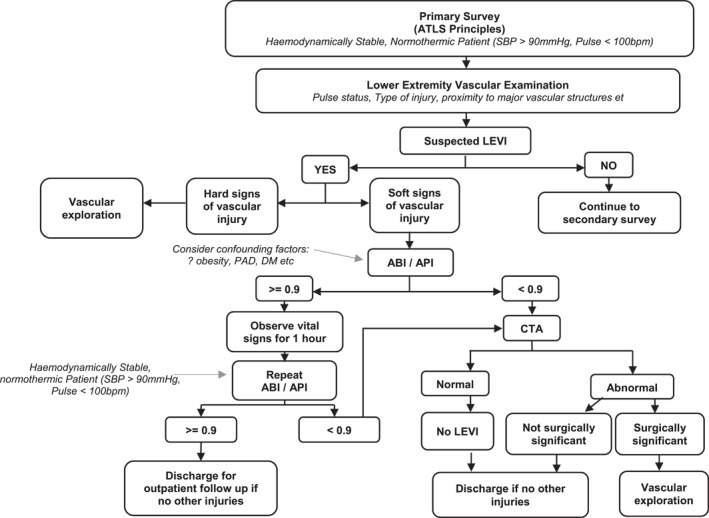 FIGURE 3
FIGURE 3| Hard signs | Soft signs |
|---|---|
| External bleeding | History of arterial bleeding on scene or during transfer |
| Rapidly expanding hematoma | Injury in proximity to a major or named artery |
| Palpable thrill or audible bruit | Small nonpulsatile hematoma over a major or named artery |
| Classical signs of arterial occlusion (pulselessness, pallor, paresthesia, pain, and paralysis) | Neurological deficit in the distribution of a peripheral nerve adjacent to a major or named artery [ |
| Frequency | Percentage | |
|---|---|---|
| Sex | ||
| Female | 8 | 5.3 |
| Male | 143 | 94.7 |
| Total | 151 | 100 |
| Age | ||
| 18–24 | 35 | 23.2 |
| 25–44 | 100 | 66.2 |
| 45–64 | 13 | 8.6 |
| ≥ 65 | 2 | 1.3 |
| Unknown | 1 | 0.7 |
| Total | 151 | 100 |
| Mechanism of injury | ||
| Blunt | 10 | 6.6 |
| Penetrating | 141 | 93.4 |
| Total | 151 | 100 |
| Type of injury | ||
| MVC | 1 | 0.7 |
| PVC | 4 | 2.6 |
| Fall | 6 | 4.0 |
| GSW | 131 | 86.8 |
| Stab | 9 | 6.0 |
| Total | 151 | 100 |
| CTA findings | Surgical management | ||
|---|---|---|---|
| Required surgery | 1 | SFA and profunda femoris injury with thrombosis and long segment SFA cutoff | Fasciotomy, SFA exploration, and PTFE graft |
| 2 | Distal popliteal artery cutoff | Popliteal artery exploration, distal popliteal repair with PTFE graft, and fasciotomy | |
| 3 | Distal SFA injury and thrombosis | SFA exploration and primary repair | |
| 4 | SFA injury and pseudoaneurysm | SFA exploration and PTFE graft | |
| 5 | SFA cutoff | SFA repair with RSVG | |
| 6 | Tibialis posterior artery cutoff | Fasciotomy for compartment syndrome, no vascular intervention | |
| 7 | SFA cutoff | SFA primary repair | |
| 8 | Mid SFA cutoff | SFA exploration and primary repair | |
| 9 | Mid SFA cutoff | SFA exploration and RSVG | |
| Did not require surgery | 1 | Superficial femoral vein early venous filling | None |
| 2 | Tibialis anterior artery cutoff | None | |
| 3 | Tibialis anterior and tibialis posterior cutoff | None | |
| 4 | Popliteal artery early venous filling | None |
| Sensitivity (95% CI) | Specificity (95% CI) | NPV (95% CI) | PPV (95% CI) | Level of agreement | Area under the ROC | |||
|---|---|---|---|---|---|---|---|---|
| Kappa (95% CI) |
| Area (95% CI) | Asymptotic significance | |||||
| Compared to CTA | ||||||||
| ABI | 84.6% (54.6%–98.1%) | 84.8% (77.7%–90.3%) | 98.3% (94.1%–99.8%) | 34.4% (18.6%–53.2%) | 0.41 (0.35–0.49) | < 0.001 | 0.85 (0.73–0.97) | < 0.001 |
| API | 84.6% (54.6%–98.1%) | 87% (80.2%–92.1%) | 98.4% (94.2%–99.8%) | 37.9% (20.7%–57.7%) | 0.46 (0.39–0.53) | < 0.001 | 0.86 (0.74–0.98) | < 0.001 |
| Compared to injuries found at operation | ||||||||
| ABI | 100% (66.4%–100%) | 83.8% (76.7%–89.4%) | 100% (96.9%–100%) | 28.1% (13.7%–46.7%) | 0.38 (0.32–0.45) | < 0.001 | 0.92 (0.87–0.97) | < 0.001 |
| API | 100% (66.4%–100%) | 85.9% (79.1%–91.2%) | 100% (97.0%–100%) | 31% (15.3%–50.8%) | 0.42 (0.26–0.49) | < 0.001 | 0.93 (0.89–0.97) | < 0.001 |
| CTA | 100% (66.4%–100%) | 97.2% (92.9%–99.2%) | 100% (97.4%–100%) | 69.2% (38.6%–90.9%) | 0.80 (0.73–0.86) | < 0.001 | 0.99 (0.97–1.00) | < 0.001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Procedures and Complications · Venous Thromboembolism Diagnosis and Management · Trauma and Emergency Care Studies
Introduction
1
Injury and trauma‐related ailments form part of the quadruple burden of disease in South Africa, a lower middle‐income country (LMIC) [1]. A recent article from 2024 demonstrated that trauma accounted for the majority (36%) of emergency department (ED) visits to a district hospital in North–West province, South Africa, mirroring presentation nationally [2, 3, 4]. This trauma burden results in significant morbidity and mortality annually, resulting in overburdened and understaffed ED and healthcare facilities [4, 5, 6, 7].
Trauma‐related vascular injuries are a leading cause of morbidity and mortality globally [8]. Although there is limited data regarding the incidence of extremity vascular trauma in South Africa, these types of injuries are a known and common cause of ED presentation. Generally, lower extremity vascular injury (LEVI) is more prevalent (50%–60%) than upper limb vascular injury [9, 10].
To limit morbidity and mortality related to these injuries in a low‐middle income country (LMIC) with a high burden of trauma‐related injury, prompt diagnosis and timely management are crucial. International literature recommends that a thorough physical examination (extremity pulse status and assessment for soft and hard signs of vascular injury) should be performed on all at‐risk patients. Those with hard signs of vascular injury (summarized in Table 1) necessitate operative intervention. In those with soft signs, comprehensive physical examination should be followed by screening vascular tests, such as ankle‐brachial index (ABI) and arterial pressure index (API), to determine the need for further imaging and management [9, 10].
ABI and API are the two most widely recognized screening vascular tests utilized in patients with potential traumatic LEVI [9, 10]. ABI is defined as the ratio of the systolic blood pressure (SBP) in the extremity distal to the level of injury to the SBP in the brachial artery of an uninjured upper extremity. API is defined as the ratio of the Doppler arterial pressure of the injured extremity distal to the level of injury to the Doppler arterial pressure in the uninjured extremity.
Internationally, an ABI/API threshold value of ≥ 0.9 has the highest combined specificity (> 90%) and negative predictive value (98%) when evaluating the likelihood of LEVI requiring intervention in patients with soft signs of vascular injury [9, 10, 11]. In the absence of other life‐threatening injuries, current international guidelines advise that patients with soft signs of vascular injury require diagnostic imaging only if the ABI or API is abnormal (< 0.9). In contrast, those with a normal ABI or API can be safely discharged for outpatient follow‐up. Mandatory outpatient follow‐up of these patients is recommended using both EAST and WTA guidelines, to identify potential initially undetected vascular injuries (1%–4%) or complications, most commonly soft tissue infections (5.5%) [9, 10].
However, there are recognized clinical scenarios where the applicability of API or ABI are limited, including hemodynamically unstable patients, hypothermia, obesity, and patients with preexisting peripheral arterial disease (PAD) [9, 10]. It is recommended that patients with hemodynamic instability be resuscitated before vascular examination is performed or relied upon. In obese patients, the literature recommends using an appropriately sized blood pressure (BP) cuff when performing vascular screening tests. In patients with known PAD, a higher threshold ABI or API value (≥ 1.0) has been suggested [9, 10]. Care should also be taken in patients with multilimb trauma.
If diagnostic vascular imaging is indicated, peripheral computed tomography angiography (CTA) has surpassed conventional digital subtraction angiography (DSA) as the international gold standard. Advantages of CTA over DSA include widespread availability, reduced costs, high interobserver agreement, intravenous only contrast injection negating the need for arterial puncture, and related complications [9, 10, 12].
However, recent international literature has demonstrated a trend toward overutilization of CTA in the workup of suspected LEVI, since it is increasingly used as the initial screening tool for identification of vascular injury prior to dedicated vascular examination and screening tools such as ABI/API [13, 14, 15]. This is contrary to international guidelines recommending the use of CTA as an adjunct to vascular screening tools. This trend may be associated with unnecessary costs incurred by the facility and patients, increased ED waiting times, increased radiation dose, contrast‐related complications, and increased workload and costs for the already overburdened radiology departments [4, 13, 14].
Furthermore, access to CT imaging in South Africa is limited, since there are only approximately 5 CT machines available per 1 million population compared to the USA, which has approximately 43 CT machines per million population [16]. Evidently, CT imaging is a scarce resource in this LMIC setting and strategies to optimize its utilization are necessary.
In this LMIC setting, where public healthcare systems are overburdened and understaffed, utilization of international vascular injury work‐up guidelines could safely eliminate unnecessary CTA imaging, thereby decreasing costs, emergency room patient overcrowding, and the workload of ED and radiology departments alike.
Aim of the Study
2
To assess the reliability of ABI and API in trauma patients with soft signs of LEVI as screening tools to safely avoid unnecessary CTA.
Method
3
Study Design
3.1
A retrospective cohort study of all lower extremity (groin to knee) trauma patients who presented with soft signs of vascular injury to Charlotte Maxeke Johannesburg Academic Hospital (CMJAH) trauma department from February 1, 2018 to January 31, 2020 was undertaken.
Ethics approval from the University of Witwatersrand Health Research Ethical Committee (HREC) (ref. no M220825) and institutional approval from the facility Chief Executive Officer were obtained.
Patients 18 years and older who had recorded vascular examination findings (bilateral lower limb and brachial artery BPs) and subsequently received lower extremity CTA were included. Those who presented with hemodynamic instability, hard signs of vascular injury, had injuries above the level of the common femoral artery or below the popliteal trifurcation, patients with bilateral lower extremity injury, and those who did not have recorded vascular examination findings (bilateral lower limb and/or brachial BPs) were excluded.
Data were retrospectively collected from the ED records, resuscitation forms, hospital files, surgical notes, and the institution's picture archiving and communication system (PACS). Data collected was anonymized and documented on a password‐protected Microsoft Excel spreadsheet for further analysis. The data collected included patient demographics; mechanism of injury (MOI); type of injury (i.e., gunshot wound [GSW] or motor vehicle collision [MVC]); brachial artery SBP; SBP of the injured and uninjured limbs; timing of CTA post trauma, CTA findings; and timing of surgery post injury, details of vascular surgical intervention if any.
The ABI and API were calculated retrospectively by the authors, using the admission brachial artery and bilateral lower limb SBPs as recorded in the patient resuscitation forms. It is unclear from patient records who measured the SBPs; however, in the study Center, these examinations are generally performed by a trauma nurse under the supervision of a medical doctor. For this study, an ABI/API threshold value equal to 0.9 or higher was considered normal, corresponding to current international standards.
For the purposes of this study, “surgically significant arterial injury” was defined as arterial injury, which required surgical intervention.
Statistical Analysis
3.2
Data were analyzed using IBM SPSS version 28. Descriptive statistics were used to demonstrate patients' demographic profiles and clinical characteristics. Categorical variables were reported using frequencies and percentages, and continuous scale data were reported in means with standard deviation or median with interquartile range. The sensitivity, specificity, NPV, and PPV of ABI and API to detect arterial injury were computed in crosstabulations in which CTA was treated as the gold standard. The sensitivity, specificity, NPV, and PPV of ABI, API, and CTA to detect significant injury were computed in crosstabulations in which injuries requiring surgical intervention was treated as the gold standard were also calculated. The receiver operating curves (ROC) and area under the curve (AUC) for ABI, API, and CTA were calculated. The Cohen's kappa statistic was used to measure the level of agreement between the alternative methods. Statistical significance testing was set at the 95% confidence level, and therefore, p < 0.05 indicated statistical significance.
Results
4
There was a total of 433 peripheral CTA performed for suspected traumatic LEVI at our facility during the study period. Of these, 282 patients (65%) had to be excluded as they were referred for CTA without documentation of brachial and/or bilateral lower extremity BP, which precluded retrospective calculation of ABI and API (see Figure 1). Similar to the included population where 91.4% had a negative CTA, a substantial majority (91.8%) of the excluded patients had a negative CTA where no vascular injury was demonstrated.
Flow diagram demonstrating total, included, and excluded CTAs with corresponding ABI/API results where applicable.
Of the 151 included patients (34.9%), most were men (94.7%, n = 143) and penetrating trauma (93.4%, n = 141) accounted for the most frequent MOI, of which gunshot wound injuries (86.8%) were the most prevalent (see Table 2). The mean age of presentation was 31.8 years, with an interquartile range of 18.8–44.8 years.
CTA Versus Surgically Significant Injury
4.1
Most of the included CTA studies (n = 138, 91%) were normal with no arterial injury. There were 13 (8.6%) positive CTA studies, which demonstrated arterial injury (see Figure 1). Of these, nine patients (69.2%) required surgical intervention and were considered surgically significant, whereas four patients (31.8%) did not require surgical intervention per trauma and vascular surgical decision and were discharged home (summarized in Table 3).
For detection of arterial injury requiring surgical intervention, CTA had a sensitivity of 100%, specificity of 97.2%, NPV of 100%, PPV of 69.2% (summarized in Table 4), and an AUC of 0.99 (plotted in Figure 2b). In this study, CTA did not miss any surgically significant arterial injuries.
ROC for predicting traumatic lower extremity arterial injury using various tests. (a) ROC for predicting traumatic lower extremity arterial injury by ABI and API compared to CTA. Blue dashed line represents ABI with an AUC of 0.85. Red dotted line represents API with an AUC of 0.86. (b) ROC for predicting surgically significant arterial injury after lower extremity trauma by ABI, API, and CTA compared to injuries found and repaired at operation. Blue dashed line represents ABI with an AUC of 0.92. Red dotted line represents API with an AUC of 0.93. Green solid line represents CTA with AUC of 0.99.
ABI Versus CTA
4.2
Of the 138 patients with negative CTA results, 117 had a normal ABI (true negative) and 21 had an abnormal ABI (false positive). Of the 13 patients with positive CTA, 11 had an abnormal ABI (true positive).
There were two patients with a false negative ABI. The first patient had early venous filling on CTA; however upon imaging and clinical review, an arteriovenous fistula (AVF) was ruled out and the patient was discharged home. The second patient had an isolated tibialis anterior artery cutoff and did not require surgical intervention. Therefore, screening ABI identified all patients requiring surgical intervention (surgically significant injury).
When compared to CTA, ABI had a specificity of 84.8%, sensitivity of 84.6%, NPV of 98.3%, PPV of 34.4% (refer to Table 4), and AUC of 0.85 in the detection of post‐traumatic LEVI (refer to Figure 2a).
API Versus CTA
4.3
Of the 138 patients with negative CTA results, 120 had a normal ABI (true negative) and 18 had an abnormal ABI (false positive). Of the 13 patients with positive CTA, 11 had an abnormal ABI (true positive) and the same 2 patients detailed under ABI versus CTA were found to have a false negative API, which were not considered surgically significant.
When compared to CTA, API had a specificity of 87%, sensitivity of 84.6%, NPV of 98.4%, PPV of 37.9% (refer to Table 4), and AUC of 0.86 in the detection of post traumatic LEVI (refer to Figure 2a).
ABI/API Versus Surgically Significant Injury
4.4
ABI had a sensitivity of 100%, specificity of 83.8%, NPV of 100%, PPV 28.1%, and AUC of 0.92 to detect surgically significant post‐traumatic LEVI, whereas API had a sensitivity of 100%, specificity of 85.9%, NPV of 100%, PPV of 31% (refer to Table 4), and AUC of 0.93 (refer Figure 2b for detail).
Indicated Versus Nonindicated CTA According to International Guidelines
4.5
Of the 151 patients who underwent peripheral CTA for soft signs of LEVI after lower extremity trauma, only 32 (21.2%) and 29 (19.2%) had a positive ABI and API, respectively, thus warranting further imaging according to international guidelines. Conversely, 119 (78.8%) and 122 (80.8%) had a negative ABI and API, respectively, which should have negated the need for further imaging according to international guidelines.
Discussion
5
Our study population size (n = 151) is comparable to similar international studies (Kelly et al., n = 157) but is presently the largest sample size locally, which specifically assesses the reliability of ABI and API to detect surgically significant LEVI [17]. Akin to other international and local studies, most of our study patients were male (94.7%), with penetrating trauma, the most common etiology for lower extremity injury [9, 10].
Although one of our study objectives were to evaluate the reliability of ABI and API in both penetrating and blunt trauma, only 10 patients (6.6%) sustained blunt lower limb trauma with none having vascular injuries requiring revascularization. As such, we were unable to accurately assess the reliability of these screening tests in blunt lower extremity trauma.
This study confirms excellent sensitivity (100%), specificity (100%), and NPV (100%) of peripheral CTA for detecting surgically significant arterial injury post lower extremity trauma, in keeping with international data [9, 10]. Furthermore, it demonstrated a low PPV (69.2%) for CTA in detection of arterial injury requiring vascular intervention, which is consistent with results from a recent retrospective review at a Level 1 trauma center by Kelly et al. [17].
When applying the standard international threshold value of 0.9, ABI and API demonstrated high specificity (ABI 83.8% and API 85.9%) and excellent sensitivity (100%) and NPV (100%) in predicting arterial injury requiring surgical intervention. In this cohort, neither ABI nor API missed any surgically significant arterial injuries requiring intervention. These findings support the use of both ABI and API as screening tools to effectively identify patients requiring further imaging to confirm or rule out surgically significant injury, and those who do not require further imaging who can therefore be discharged home for outpatient follow‐up, consistent with international data [9, 10].
Approximately two‐thirds of the 433 patients referred for CTA for suspected LEVI over the 2‐year study period had to be excluded due to a lack of documentation of vascular examination findings. Most excluded patients (91.8%) had a negative CTA. This begs the question whether most of these CTA's could safely have been avoided.
Based on the results obtained from patients who met inclusion criteria (n = 151), by doing a simple physical vascular examination with API or ABI and applying internationally recognized cutoff values, 79.5% of these studies were unnecessary. Considering that each peripheral CTA performed at our institution currently costs approximately R4700 and takes at least 15 min to perform, approximately R564,000 of (± USD 31,996) unnecessary expenditure and at least 30 h of imaging time could have been saved by utilizing recognized international guidelines. This represents a significant potential saving for an institution in a low‐middle income country where resources are already very limited. Our results additionally support recent international data, which has demonstrated an overutilization of peripheral CTA after lower extremity trauma [13, 17].
Limitations
6
As this study is a retrospective review, it is inherently limited by the quality and accuracy of recorded data, including incompletely documented vascular examination findings. Given the absence of recorded vascular examination findings in up to two‐thirds of the total patients who received CTA for suspected LEVI, many patients had to be excluded from the sample, which may impact the accuracy of the results. This could be overcome by designing a prospective study with clearly defined data fields for collection and thus eliminating this source of bias.
Due to the low number of patients with blunt LEVI present in this cohort of patients, no inferences could be made about the reliability of ABI/API to detect significant vascular injuries in this population.
Care should be taken in those recognized clinical scenarios where the applicability of API/ABI is limited (hemodynamically instability, hypothermia, obesity, PAD, and bilateral lower extremity injury) [9, 10]. The mean age of presentation in this cohort was 31.8 years (interquartile range of 18.8–44.8 years), as such, PAD was not prevalent and the reliability of ABI/API in this scenario could not be assessed.
However, despite the identified limitations, we believe that the congruence between the results from this study and similar international studies affirms the utility and reliability of physical examination and screening vascular examination tests in the workup of suspected lower extremity trauma.
Conclusions
7
Our study affirms the reliability of ABI and API as a screening vascular examination tool in South African patients presenting with soft signs of vascular injury after unilateral lower extremity penetrating trauma. It further supports international data demonstrating CTA overuse in this subset of trauma patients. If applied correctly, we suggest ABI and API may be useful screening tests to limit unnecessary peripheral CTA after lower extremity trauma (refer to Figure 3 for the proposed protocol).
Flow diagram demonstrating proposed utilization of ABI/API in patients with suspected traumatic lower extremity vascular injury.
Future Perspectives
8
This study demonstrates the need for clear emergency department trauma protocols and selective referral for peripheral CTA after trauma.
Unfortunately, there is an absence of clear local or international guidelines regarding the timing of outpatient follow‐up in patients discharged from ED after lower extremity trauma to screen for missed vascular injury. We suggest that this is an important future avenue of study.
Author Contributions
Rubinette Robbertze: conceptualization, investigation, writing – original draft, methodology, validation, visualization, writing – review and editing, formal analysis, data curation. Megan Lubout: conceptualization, methodology, validation, writing – review and editing, project administration, supervision, investigation, formal analysis. Daniel Nicholas Prince: investigation, methodology, validation, writing – review and editing, supervision, formal analysis. Isabella Margaretha Joubert: writing – review and editing, supervision, formal analysis. Maeyane S. Moeng: methodology, validation, writing – review and editing, project administration, supervision, formal analysis.
Ethics Statement
Ethics approval was obtained from the University of Witwatersrand Health Research Ethical Committee (HREC) (ref. no M220825).
Conflicts of Interest
The authors declare no conflicts of interest.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of any affiliated agency of the authors.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization , Country Cooperation Strategy: South Africa (WHO [Internet], 2018), 1–2, https://www.who.int/publications/i/item/WHO‐CCU‐18.02‐South‐Africa.
- 2J. A. Adewole , J. M. Tumbo , and H. I. Okonta , “Emergency Care Visits at a South African Hospital: Implications for Healthcare Services and Policy,” South African Family Practice 66, no. 1 (2024): 1–6, 10.4102/safp.v 66i 1.5816.PMC 1101903238572872 · doi ↗ · pubmed ↗
- 3T. C. Hardcastle , G. Oosthuizen , D. Clarke , and E. Lutge , “Trauma a Preventable Burden of Disease in South Africa: Review of the Evidence, With a Focus on Kwa Zulu‐Natal,” South African Health Review [Internet] 2016, no. 1 (2016): 179–189, https://journals.co.za/content/healthr/2016/1/EJC 189309?TRACK=RSS.
- 4A. A. Bashir , V. Y. Kong , R. D. Weale , et al., “Quantifying the Burden of Trauma Imaging on the CT Scan Service at a Major Trauma Centre in South Africa,” South African Journal of Surgery 57, no. 2 (2019): 48–53, 10.17159/2078-5151/2019/v 57n 2a 2836.31342684 · doi ↗ · pubmed ↗
- 5M. Prinsloo , S. Mhlongo , B. Dekel , et al., “The 2nd Injury Mortality Survey: A National Study of Injury Mortality Levels and Causes in South Africa in 2017,” in In Collaboration With Gender and Health Research Unit and Biostatistics South African Medical Research Council South Africa in 2017 (2021), 1–61.
- 6Stats S. A. Mortality and Causes of Death in South Africa, 2018: Findings From Death Notification (Statistical Release P 03093 [Internet], 2021), 1–142, www.statssa.gov.za.
- 7J. Goosen , F. Plani , and M. Moeng , Overview of Trauma in South Africa (Occupational Health Southern Africa, 2007).
- 8Z. B. Perkins , H. D. De’Ath , C. Aylwin , K. Brohi , M. Walsh , and N. R. M. Tai , “Epidemiology and Outcome of Vascular Trauma at a British Major Trauma Centre,” European Journal of Vascular and Endovascular Surgery 44, no. 2 (2012): 203–209, 10.1016/j.ejvs.2012.05.013.22658774 · doi ↗ · pubmed ↗