Factors Associated With Mortality in Leukemia and Lymphoma With COVID-19: A National Inpatient Sample Analysis (2020–2021)
Saketh Palasamudram Shekar, Barath Prashanth Sivasubramanian, Diviya Bharathi Ravikumar, Husna Qadeer, Ibthisam Ismail Sharieff, Rhea Prasad, Sindhu Chandra Pokhriyal, Amulya Bellamkonda, Mamtha Balla, Rutul Dalal

TL;DR
This study finds that leukemia and lymphoma patients with COVID-19 face high mortality risks, especially during certain pandemic periods, and identifies factors like organ dysfunction that increase the risk.
Contribution
The study provides new insights into mortality trends and risk factors for leukemia and lymphoma patients with COVID-19 using U.S. national inpatient data.
Findings
Leukemia and lymphoma patients with COVID-19 had mortality rates of 14.7% and 19.7%, respectively.
Mortality was strongly associated with pulmonary, renal, and cardiac dysfunction, as well as bone marrow dysfunction.
Mortality surges occurred during specific pandemic periods, such as October-December 2020 and January-March 2021.
Abstract
Background Patients with hematological malignancies face a substantially increased mortality from COVID-19. Although the peak of the COVID-19 pandemic has passed, the virus remains common, and understanding its impact on vulnerable groups such as those with hematologic malignancies remains crucial. Limited research exists on mortality patterns in leukemia and lymphoma patients during the pandemic. Studying these outcomes provides important insights into how different waves of COVID-19 affected immunocompromised individuals and supports the development of strategies for prevention, patient care, and risk reduction, which are essential both for managing emerging variants and preventing future pandemics. We aimed to identify the mortality risk of COVID-19 in leukemia (LekCov-19) and lymphoma (LymCov-19) in the United States and the mortality trends between each quartile from 2020 to 2021.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
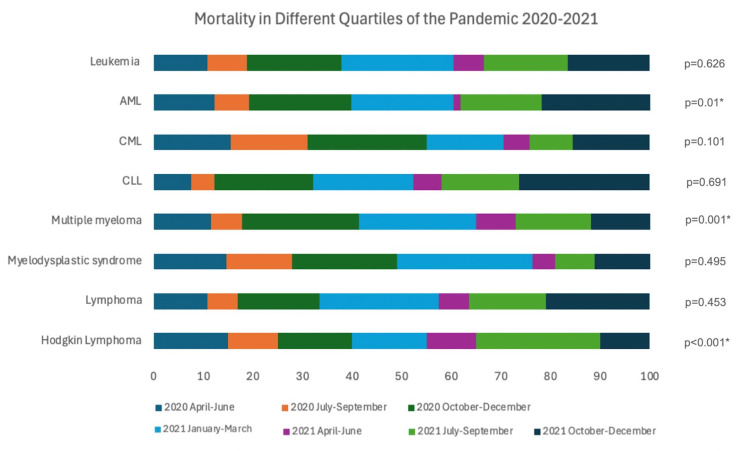 Figure 1
Figure 1| Leukemia patients with COVID-19 | Lymphoma patients with COVID-19 | |||||
| Survival percentage (%) (n = 6991) | Mortality percentage (%) (n = 1200) | p-value | Survival percentage (%) (n = 2071) | Mortality percentage (%) (n = 507) | p-value | |
| Age over 65 years | 55.9 | 78.0 | <0.0001 | 62.5 | 74.6 | <0.0001 |
| Gender | 0.0741 | 0.3307 | ||||
| Male | 56.7 | 59.5 | 58.4 | 60.8 | ||
| Female | 43.3 | 40.5 | 41.6 | 39.3 | ||
| Race | 0.0021 | 0.654 | ||||
| White | 60.7 | 66.9 | 76.1 | 78.8 | ||
| Black | 16.2 | 14.8 | 8.0 | 7.1 | ||
| Hispanic | 16.7 | 13.1 | 11.1 | 8.9 | ||
| Asian or Pacific Islander | 2.4 | 1.6 | 2.1 | 2.0 | ||
| Native American | <1 | <1 | <1 | <1 | ||
| Other | 3.4 | 3.1 | 2.5 | 2.8 | ||
| Median household | 0.3384 | 0.5524 | ||||
| $1 - $49,999 | 29.0 | 31.0 | 24.4 | 25.5 | ||
| $50,000 - $64,999 | 27.5 | 25.4 | 28.3 | 29.1 | ||
| $65,000 - $85,999 | 24.5 | 23.8 | 26.0 | 27.1 | ||
| $86,000 or more | 19.0 | 19.8 | 21.3 | 18.4 | ||
| Primary expected payer | <0.0001 | 0.0258 | ||||
| Medicare | 54.0 | 71.4 | 60.8 | 67.3 | ||
| Medicaid | 11.7 | 6.5 | 7.6 | 4.8 | ||
| Private, including HMO | 26.9 | 17.5 | 27.1 | 22.6 | ||
| Self-pay | 3.1 | 1.3 | 1.4 | 2.0 | ||
| No charge | <1 | <1 | <1 | <1 | ||
| Other | 4.1 | 3.1 | 2.8 | 2.8 | ||
| Census division of the hospital | 0.065 | 0.7451 | ||||
| New England | 4.0 | 4.0 | 5.7 | 5.1 | ||
| Mid-Atlantic | 15.2 | 16.5 | 16.0 | 16.2 | ||
| East North Central | 17.3 | 16.3 | 19.2 | 16.2 | ||
| West North Central | 7.7 | 7.3 | 8.2 | 7.5 | ||
| South Atlantic | 21.2 | 18.5 | 18.2 | 18.3 | ||
| East South Central | 5.8 | 7.4 | 6.1 | 7.1 | ||
| West South Central | 10.0 | 11.8 | 10.0 | 10.9 | ||
| Mountain | 7.0 | 6.0 | 6.8 | 8.5 | ||
| Pacific | 11.7 | 12.0 | 9.9 | 10.3 | ||
| Relative bed size category of the hospital | 0.0842 | 0.629 | ||||
| Small | 25.6 | 22.8 | 22.9 | 20.9 | ||
| Medium | 26.3 | 26.1 | 27.1 | 28.0 | ||
| Large | 48.2 | 51.1 | 50.0 | 51.1 | ||
| Location/teaching status of the hospital | 0.0981 | 0.0637 | ||||
| Rural | 11.0 | 9.3 | 11.5 | 8.3 | ||
| Urban non-teaching | 18.0 | 17.0 | 16.9 | 15.6 | ||
| Urban teaching | 71.0 | 73.8 | 71.6 | 76.1 | ||
| Palliative care services | 4.3 | 47.1 | <0.0001 | 4.9 | 54.2 | <0.0001 |
| Charlson comorbidities | <0.0001 | <0.0001 | ||||
| 0 comorbidities | 15.3 | 4.6 | <1 | <1 | ||
| 1 comorbidity | 11.6 | 5.8 | <1 | <1 | ||
| 2 comorbidities | 23.8 | 18.8 | 31.9 | 20.3 | ||
| ≥3 comorbidities | 49.7 | 71.0 | 67.7 | 79.1 | ||
| Leukemic patients with COVID-19 | Lymphoma patients with COVID-19 | |||||
| Pulmonary Variables | Survival percentage (%) (n = 6991) | Mortality percentage (%) (n = 1200) | p-value | Survival percentage (%) (n = 2071) | Mortality percentage (%) (n = 507) | p-value |
| Acute respiratory failure | 61.5 | 64.8 | 0.0296 | 55.2 | 66.3 | <0.0001 |
| ARDS | 4.6 | 30.2 | <0.0001 | 3.0 | 30.4 | <0.0001 |
| Acute pulmonary embolism | <1 | <1 | 0.1877 | <1 | <1 | 0.0613 |
| Renal and metabolic variables | ||||||
| Acute kidney injury | 22.4 | 57.5 | <0.0001 | 21.3 | 53.5 | <0.0001 |
| Acidosis | 8.6 | 29.1 | <0.0001 | 6.5 | 26.0 | <0.0001 |
| Hemodialysis | 3.2 | 12.1 | <0.0001 | 1.8 | 9.7 | <0.0001 |
| Hepatic dysfunction | 0.3 | 4.6 | <0.0001 | <1 | 3.4 | <0.0001 |
| Metabolic encephalopathy | 4.9 | 12.8 | <0.0001 | 4.2 | 11.8 | <0.0001 |
| Diabetes | 33.0 | 37.3 | 0.003 | 30.0 | 30.6 | 0.8129 |
| Cardiovascular variables | ||||||
| Arrhythmia | 9.0 | 18.2 | <0.0001 | 9.0 | 18.2 | <0.0001 |
| Acute heart failure | 8.2 | 16.0 | <0.0001 | 8.2 | 16.0 | <0.0001 |
| Stroke | 0.3 | 1.4 | 0.0019 | <1 | 1.4 | 0.0019 |
| Hypotension | 7.3 | 12.6 | 0.0001 | 7.3 | 12.6 | 0.0001 |
| Myocardial infarction | 4.6 | 3.6 | <0.0001 | 4.6 | 3.4 | <0.0001 |
| Cardiogenic shock | 0.2 | 1.6 | 0.0001 | <1 | 1.6 | 0.0001 |
| Sudden cardiac arrest | 0.1 | 11.8 | <0.0001 | <1 | 11.8 | <0.0001 |
| Hemato-oncological variables | ||||||
| Anemia | 36.2 | 45.2 | <0.0001 | 34.7 | 45.2 | <0.0001 |
| Thrombocytopenia | 11.5 | 21.9 | <0.0001 | 13.0 | 24.7 | <0.0001 |
| Neutropenia | 3.0 | 3.0 | 0.9942 | 8.2 | 6.1 | 0.1227 |
| Pancytopenia | 7.5 | 14.5 | <0.0001 | 11.9 | 18.2 | 0.0002 |
| HSCT | 4.2 | 3.7 | 0.423 | 4.6 | 3.4 | 0.2218 |
| Infections and others | ||||||
| HIV | 0.0 | 0.0 | 0.4729 | <1 | 0.0 | 0.3912 |
| Fungal infections | 0.6 | 1.8 | <0.0001 | 1.3 | 5.5 | <0.0001 |
| Severe sepsis | 2.0 | 25.0 | <0.0001 | 1.6 | 22.7 | <0.0001 |
| ICU-related variables | ||||||
| Tracheostomy | 1.1 | 2.9 | 0.0086 | 0.8 | 2.2 | 0.0086 |
| CPR | 0.2 | 11.8 | <0.0001 | <1 | 9.5 | <0.0001 |
| Invasive ventilation | 0.7 | 9.4 | <0.0001 | <1 | 8.9 | <0.0001 |
| Ventilator-associated pneumonia | 0.2 | 2.0 | <0.0001 | <1 | 2.0 | <0.0001 |
| Vasopressor usage | 0.5 | 2.6 | <0.0001 | <1 | 15.0 | <0.0001 |
| Leukemia | Adjusted odds ratio (aOR) | 95% CI | p-value |
| COVID-19 | 2.3 | 2.0 - 2.7 | <0.001 |
| Leukemia patients with COVID-19 | Adjusted odds ratio (aOR) | 95% CI | p-value |
| Pancytopenia | 1.8 | 1.4 - 2.3 | <0.001 |
| Neutropenia | 1.6 | 0.95 - 2.8 | 0.08 |
| Thrombocytopenia | 1.3 | 1.1 - 1.6 | 0.006 |
| Anemia | 1.1 | 0.9 - 1.2 | 0.59 |
| HSCT | 0.75 | 1.4 - 2.3 | 0.174 |
| Lymphoma | Adjusted odds ratio (aOR) | 95% CI | p-value |
| COVID-19 | 2.8 | 2.2 - 3.6 | <0.001 |
| Lymphoma patients with COVID-19 | Adjusted odds ratio (aOR) | 95% CI | p-value |
| Pancytopenia | 1.6 | 1.1 - 2.3 | 0.024 |
| Neutropenia | 0.8 | 0.5 - 1.5 | 0.529 |
| Thrombocytopenia | 1.7 | 1.2 - 2.4 | 0.004 |
| Anemia | 1.14 | 0.9 - 1.5 | 0.331 |
| HSCT | 0.43 | 0.2 - 1.1 | 0.086 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 and healthcare impacts · COVID-19 Clinical Research Studies · Healthcare cost, quality, practices
Introduction
Cancer patients are more vulnerable to acquiring SARS-CoV-2 infection compared to the general population (p = 0.01) [1]. They also face a higher risk of developing severe illness due to a profoundly compromised immune system induced by both chemotherapy and the malignancy itself [1]. Notably, in a study by Lunski et al., patients with active cancer, when infected with COVID-19, had a higher mortality rate (21.2%) when compared with non-cancer patients (8.7%) (p < 0.001) [2]. It is essential to recognize that the immune status of patients can be a crucial factor contributing to the severity of complications and subsequent mortality [3]. COVID-19 infection triggers the release of excess cytokines or proinflammatory proteins (IL-1, IL-6, tumor necrosis factor-alpha (TNF-ɑ), interferon (IFN)-gamma, etc.) by the immune system. This cytokine storm and inflammation are responsible for severe consequences in multiple organs, leading to multi-organ dysfunction [4,5].
The overall mortality associated with COVID-19 was notably high in patients with hematological malignancies, ranging between 34% and 36.5%, which is significantly higher than the 23.8% mortality rate observed in patients with solid tumors [6]. Of note, a recent study in Europe observed the highest COVID-19-related mortality with myelodysplastic syndrome (42.3%), acute myeloid leukemia (40%), and hairy cell leukemia (34.8%) [7]. Factors contributing to this increased mortality risk include significant humoral and cellular immunosuppression [8], aggravated by chemotherapy [9]. Disease-related factors such as prolonged shedding and persistent immune dysregulation can lead to the exhaustion of T cells and decreased viral clearance, which play a significant role in disease progression [10]. In a recent study of patients with acute myeloid leukemia (AML), it was found that older age (p = 0.012), active disease (p < 0.001), and treatment discontinuation (p < 0.001) were associated with increased mortality [11]. Similarly, factors associated with higher mortality risk in lymphoma were age over 70 years, heart disease, and chronic kidney disease (p < 0.05) [12].
There has been a limited number of case series documenting the COVID-19 infection in individuals with hematologic malignancies, and these reports only offer limited information concerning the disease status or histological classification [13]. Most studies are limited by their narrow inclusion criteria, small sample sizes, and case duplications [14]. Many cohort studies during the early stages of the pandemic overestimated the risk of COVID-19 by including asymptomatic patients and those with a secondary diagnosis of COVID-19 [15]. Data on COVID-19’s impact on leukemia patients remain limited [16], with lymphoma patients even more underrepresented [17].
This retrospective cross-sectional study aims to assess risk factors for in-hospital mortality in leukemia and lymphoma patients primarily admitted for COVID-19 in the United States. We also aimed to examine trends in mortality from COVID-19 in leukemia and lymphoma patients from April 2020 to December 2021.
Materials and methods
Design and data source
We performed a retrospective observational study using the 2020-2021 National Inpatient Sample (NIS) database. The NIS database is developed by the Healthcare Cost and Utilization Project (HCUP) and sponsored by the Agency for Healthcare Research and Quality (AHRQ). The NIS generates regional and national estimates of inpatient admissions and records of discharge outcomes [18]. The document encompasses various components like patient demographics (such as age, sex, race, and median income based on location), diagnosis, and procedure codes derived from the International Classification of Diseases, Tenth Revision, Clinical Modification/Procedure Coding System (ICD-10-CM/PCS). The ICD-10-CM/PCS measures severity and comorbidity, hospital characteristics, discharge status, and length of stay (LOS).
Ethical consideration, sample size, and study population
The NIS is a de-identified, publicly accessible database, and this investigation did not require institutional review board approval. This study did not involve the estimation of a predetermined sample size. The research did not employ any sampling methodology. Individuals aged 18 years or above admitted with an ICD-10-CM code of leukemia and lymphoma were included. We used a previously established method to identify patients admitted for COVID-19 infection with a history of hematological malignancies (leukemia and lymphoma) [19-22]. We compared the COVID-19 cohort with all other admissions. ICD-10-CM/PCS codes were used to identify patients and their comorbidities (acute respiratory failure, sepsis, acute kidney injury, myocardial infarction) are provided in Supplementary Table A1. Before accessing the NIS database, we ensured compliance with the data user agreement outlined by the AHRQ. Furthermore, the databases utilized comply with the Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule’s definition of limited datasets and exclude explicit patient identifiers.
Outcomes
Our primary objective was to assess mortality risk in adults with leukemia or lymphoma admitted for COVID-19. The secondary objective was to evaluate the risk of mortality in the subset of this population treated with hematopoietic stem cell transplantation (HSCT).
Statistical methods
We conducted our analysis by examining continuous variables through means and t-tests, and qualitative variables were assessed using the chi-square test. We set a significance level of p ≤ 0.05. Stata v18 (StataCorp LLC, College Station, TX) was used to conduct the analysis. We used two methods to adjust for confounders: propensity matching and multivariate regression analysis. A non-parsimonious multivariate logistic regression model was developed to estimate the propensity score for COVID-19 and mortality using acute respiratory failure and invasive ventilation. The double robust method was then used to generate treatment weights, and the inverse probability of treatment weighting was used to match cases with controls using generalized linear models [23]. Multivariable regression models were built by including all the confounders that were significantly associated with the outcome on univariable analysis with a cutoff p = 0.3. Variables found to be important based on the literature were also forced into the models. Mortality trends in the patients were analyzed using univariate analysis and categorized into quartiles.
Results
Leukemia with COVID-19
Of 8,191 Leukemia patients with COVID-19, 1,200 (14.7%) had mortality. Mortality was common in patients over 65 years of age compared to survivors (p < 0.0001). There was no difference in mortality according to gender (p > 0.05). Race was significantly associated with mortality (p < 0.01). Table 1 presents the sociodemographic characteristics of leukemia patients with COVID-19.
Comorbidities in leukemic patients with COVID-19
COVID-19 patients with more than three comorbidities had higher mortality rates (p < 0.0001). Several comorbidities were significantly associated with increased mortality. Pulmonary dysfunctions, including acute respiratory distress syndrome (ARDS), acute respiratory failure, acute pulmonary embolism, and ventilator-associated pneumonia, showed higher mortality (p ≤ 0.0001). Renal and metabolic factors, such as acute kidney injury, acidosis, hepatic dysfunction, and acute metabolic encephalopathy, also showed higher mortality (p ≤ 0.0001). Cardiac factors, including arrhythmia, acute heart failure, hypotension, myocardial infarction, cardiogenic shock, and sudden cardiac arrest, were significantly associated with increased mortality (p ≤ 0.0001). Similarly, bone marrow dysfunctions, such as anemia, thrombocytopenia, and pancytopenia, were associated with higher mortality (p ≤ 0.0001). HSCT was not significantly associated with mortality (p > 0.05). Interventions such as hemodialysis, cardiopulmonary resuscitation, invasive ventilation, tracheostomy, and vasopressor usage were common (p < 0.05). Table 2 shows the comorbidities and complications leading to mortality in leukemia patients with COVID-19.
Multivariate regression analysis was performed to determine whether COVID-19 is associated with increased mortality. The results showed that COVID-19 was associated with a two-fold increase in the odds of mortality (p < 0.001). Among leukemia patients with COVID-19, pancytopenia had 80% increased odds (p < 0.001) and thrombocytopenia had 30% increased odds (p < 0.01) of mortality, while neutropenia and anemia (p > 0.05) did not alter mortality. Additionally, there was no difference in mortality in patients who were treated with HSCT (p > 0.05). Table 3 shows multivariate logistic regression for leukemia and lymphoma patients with COVID-19.
Lymphoma with COVID-19
Of 2,578 lymphoma patients with COVID-19, 507 had mortality (19.7%). In patients aged 65 years and older, the proportion of non-survivors was significantly higher than that of survivors (p < 0.0001). There was no significant difference in mortality by race and gender (p > 0.05). Table 1 presents the sociodemographic characteristics of lymphoma patients with COVID-19.
Comorbidities in lymphoma patients with COVID-19
COVID-19 patients with more than three comorbidities had higher mortality rates compared to those who survived (p < 0.0001). Several comorbidities were significantly associated with increased mortality. Pulmonary dysfunctions, including ARDS, acute respiratory failure, and ventilator-associated pneumonia, were linked to higher mortality (p ≤ 0.0001). Renal and metabolic factors, such as acute kidney injury, acidosis, hepatic dysfunction, and metabolic encephalopathy, also showed higher mortality (p ≤ 0.0001). Cardiac factors, including arrhythmia, acute heart failure, hypotension, myocardial infarction, and cardiogenic shock, were associated with increased mortality (p ≤ 0.0001). Bone marrow dysfunctions, such as anemia (p ≤ 0.0001), thrombocytopenia (p ≤ 0.0001), and pancytopenia (p < 0.001), were also associated with higher mortality. HSCT was not associated with mortality (p > 0.05). Interventions such as hemodialysis, invasive ventilation, cardiopulmonary resuscitation, tracheostomy, and vasopressor use were required more in those who faced mortality (p < 0.05). Table 2 shows the comorbidities and complications leading to mortality in lymphoma patients with COVID-19.
Multivariate regression analysis was performed to determine whether COVID-19 is associated with increased mortality. The results showed that COVID-19 was associated with a two-fold increase in the odds of mortality (p < 0.001). Of lymphoma patients with COVID-19, pancytopenia had 60% increased odds (p < 0.05) and thrombocytopenia had 70% increased odds (p < 0.01) of mortality, while neutropenia and anemia (p > 0.05) did not alter mortality. Additionally, HSCT did not alter mortality (p > 0.05). Table 3 shows multivariate logistic regression for leukemia and lymphoma patients with COVID-19.
Our study showed that AML showed the highest mortality rate (21.7%), followed by myelodysplastic syndrome (18.6%), chronic myeloid leukemia (CML, 18.5%), multiple myeloma (18.4%), Hodgkin lymphoma (13.5%), leukemia (10.7%), and lymphoma (10.2%). Our analysis of COVID-19 in hematological malignancies from April 2020 to December 2021 revealed significant trends in mortality rates in different quartiles. Leukemia showed more than 15% proportional mortality in the discharge quartile from October to December 2020 (19.1%) and January to March (22.6%), July to September (16.9%), and October to December (16.5%) in 2021 (p < 0.001). Chronic lymphocytic leukemia (CLL) had a significant increase in proportional mortality during October to December (19.9%) in 2020 and January to March (20.1%), July to September (15.6%), and October to December (26.3%) in 2021 (p = 0.001). In AML, CML, multiple myeloma, and myelodysplastic syndrome, proportional mortality did not vary between the different quartiles (p > 0.05).
Lymphoma patients had significant proportional mortality during October to December (16.4%) in 2020 and January to March (24%), July to September (15.5%), and October to December (16.4%) in 2021 (p = 0.01). Hodgkin lymphoma showed no significant proportional mortality increase during these periods (p > 0.05).
These findings emphasize that the October to December 2020 and January to March 2021 quartiles were particularly critical, with all hematological malignancies exhibiting proportional mortality rates exceeding 15%.Supplementary Table A2 shows quarterly trends in COVID-19-related mortality in patients with hematological malignancies (April 2020 - December 2021). Figure 1 shows mortality in different quartiles of the pandemic (2020-2021).
Mortality in different quartiles of the pandemic (2020-2021). * Significant value.AML: acute myeloid leukemia; CML: chronic myeloid leukemia; CLL: chronic lymphocytic leukemia.
Discussion
Using a retrospective study design, we identified the mortality risk in hospitalized COVID-19 patients with pre-existing leukemia and lymphoma. In patients with malignancies, COVID-19 has been shown to have a severe presentation due to immune dysfunction leading to low secretion of IFN-1. COVID-19 further compromises immunity by disrupting regulatory pathways such as the adrenergic and immune checkpoint pathways. These mechanisms are also affected in those with malignancies, amplifying immune suppression and increasing the risk of severe outcomes and mortality [24]. Our analysis showed that COVID-19 was associated with a two-fold increase in the odds of mortality in leukemia and lymphoma patients (p < 0.001). In our study, thrombocytopenia and pancytopenia were associated with increased odds of mortality in both cohorts (p < 0.01). Studies indicate that COVID-19 significantly impacts the hematopoietic system, causing cytopenias (lymphopenia, thrombocytopenia, leukopenia) and hypercoagulopathy [25]. Thrombocytopenia may result from decreased platelet production, increased destruction, sequestration, or consumption [25]. Pancytopenia in COVID-19 may result from molecular mimicry, cytokine-mediated suppression of hematopoiesis, and viral bone marrow infiltration [25,26]. HSCT recipients had lower odds of mortality in both cohorts (p > 0.05), although this difference did not reach statistical significance. This may be attributable to the inability to account for the timing of HSCT and the immune status of the patients. This finding is consistent with the study by Karatas et al., which suggested that mortality rates among HSCT recipients are lower in patients whose primary disease is in remission, compared to those whose disease is not in remission [27].
We found that COVID-19 mainly affects the elderly, and Sharafeldin et al. reported age ≥ 65 years (HR: 1.9, 95% CI: 1.3- 3.1) as one of the risk factors for death in cancer patients [19,28,29]. Immunosenescence, deteriorating immunity with progressing age, makes older individuals susceptible to adverse outcomes [30]. Sepsis and fungal infections are significant factors associated with mortality (p < 0.001). Secondary infections and multiorgan failure are known outcomes of COVID-19 [31-33]. COVID-19 is associated with high mortality in patients with hematological malignancies who develop ARDS [13,34]. The pathogenesis is a consequence of increased neutrophilic and eosinophilic activity and high cytokine release (IL-6, TNF-ɑ) [35]. Invasive ventilation is commonly associated with increased mortality (p < 0.001). Studies have shown that mechanical ventilation was associated with a four-fold rise in mortality (p = 0.02) [15,36]. Ventilated patients are also at risk of secondary infections, pneumothorax, and asphyxia due to ventilator-associated complications [37], which may explain the higher mortality associated with ventilator-associated pneumonia observed in our study (p < 0.001). Acute kidney injury from COVID-19 is due to direct invasion of podocytes and proximal tubular cells, leading to acute tubular injury, tubulointerstitial injury, and glomerular injury. Other factors contributing to renal damage include severe volume depletion, cytokine storm, collapsing glomerulopathy, and secondary hypoxia of renal vascular endothelium due to elevated IL-6 [38,39]. COVID-19 has high cardiac complications such as arrhythmia, acute heart failure, myocardial infarction, and cardiogenic shock (p < 0.001), as shown in our study. COVID-19 can increase the risk of thrombosis and directly damage myocardial cells, leading to cardiomyopathy and acute heart failure [40-42].
Our study examined COVID-19 mortality from April 2020 to December 2021 in patients with hematological malignancies and noted trends aligning with shifts in SARS-CoV-2. Mortality rates rose during the April-June 2020 quartile, coinciding with the spread of the wild-type strain [26,43,44]. Before April, COVID-19 testing was not widely used. After June, a slowing of cases was seen in July-September 2020, likely attributable to mask mandates and additional restrictions implemented across various states that helped control transmission. However, as winter approached, the October-December 2020 and January-March 2021 quartiles became particularly critical, with all hematological malignancies exhibiting high mortality rates [26,43-45]. During the April-June 2021 quartile, a drop in mortality rates was seen, likely due to increased vaccination coverage that began in December 2020. However, mortality rates rose starting in July 2021, coinciding with the spread of the more transmissible and severe Delta variant [46]. The emergence of Omicron BA.1 in December 2021 and reduced vaccine effectiveness in cancer patients and their greater risk of severe COVID-19 further contributed to the surge in cases [26,47,48]. Wood et al. reported that the mortality of CLL patients with COVID-19 was 28%, compared to 17.9% in our study [49]. The differences could be due to the different sample sizes in both studies. CLL patients may not consistently generate anti-SARS-CoV-2 antibodies [50], leading to vaccine inefficiency and poorer outcomes. In our study, CLL patients were also noted to have high mortality in the last quartile of 2021, when all other malignancies had lower rates.
This study was limited by the absence of follow-up and information regarding the staging of the malignancies, treatment, treatment responses, and vaccine status. Consequently, we are unable to determine the total effect of vaccines and their side effects. Additionally, as our sample included individuals admitted for COVID-19, we could not estimate the overall impact of COVID-19, at-home mortality rates, or post-discharge outcomes. The underrepresentation of racial minorities leads to inconclusive evidence when it comes to racial disparities. Duplication of patient data and coding errors from the use of ICD-10 were not addressed. The database only includes information from the United States, so its findings may not apply to other countries. The database does not include the exact lab values, which also limits our understanding of the comorbidities in greater detail.
Conclusions
This study highlights the increased mortality associated with COVID-19 among leukemia and lymphoma patients, with pancytopenia and thrombocytopenia linked to higher mortality in these cohorts. Mortality was highest between October 2020 and March 2021. Understanding these mortality trends from the COVID-19 pandemic is crucial for forecasting future mortality risks in cancer patients. As vaccination and antiviral therapies have evolved, it is important to examine how these interventions have influenced outcomes in patients with hematologic malignancies. Research should also prioritize refining treatment regimens, strengthening preventive strategies, advancing novel therapies, and ensuring long-term follow-up care for this vulnerable population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Patients with cancer appear more vulnerable to SARS-Co V-2: a multicenter study during the COVID-19 outbreak Cancer Discov Dai M Liu D Liu M 7837911020203234559410.1158/2159-8290.CD-20-0422 PMC 7309152 · doi ↗ · pubmed ↗
- 2Multivariate mortality analyses in COVID-19: comparing patients with cancer and patients without cancer in Louisiana Cancer Lunski MJ Burton J Tawagi K 26627412720213311241110.1002/cncr.33243 · doi ↗ · pubmed ↗
- 3CD 8+ T cells in SARS-Co V-2 induced disease and cancer—clinical perspectives Front Immunol Mortezaee K Majidpoor J 8642981320223543234010.3389/fimmu.2022.864298 PMC 9010719 · doi ↗ · pubmed ↗
- 4CD 8+ T cell senescence: lights and shadows in viral infections, autoimmune disorders and cancer Int J Mol Sci Tedeschi V Paldino G Kunkl M Paroli M Sorrentino R Tuosto L Fiorillo MT 33742320223532879510.3390/ijms 23063374 PMC 8955595 · doi ↗ · pubmed ↗
- 5Marked T cell activation, senescence, exhaustion and skewing towards TH 17 in patients with COVID-19 pneumonia Nat Commun De Biasi S Meschiari M Gibellini L 34341120203263208510.1038/s 41467-020-17292-4PMC 7338513 · doi ↗ · pubmed ↗
- 6Mortality of COVID-19 in patients with hematological malignancies versus solid tumors: a systematic literature review and meta-analysis Clin Exp Med Hardy N Vegivinti CT Mehta M 194519592320233679523910.1007/s 10238-023-01004-5PMC 9933827 · doi ↗ · pubmed ↗
- 7COVID-19 infection in adult patients with hematological malignancies: a European Hematology Association Survey (EPICOVIDEHA)J Hematol Oncol Pagano L Salmanton-García J Marchesi F 1681420213464956310.1186/s 13045-021-01177-0PMC 8515781 · doi ↗ · pubmed ↗
- 8Haematological malignancies implications during the times of the COVID-19 pandemic Oncol Lett Papakonstantinou E Dragoumani K Efthimiadou A 8562220213477759010.3892/ol.2021.13117 PMC 8581473 · doi ↗ · pubmed ↗