A Case of Choriocarcinoma Undergoing Laparoscopic Surgery Due to Suspected Peritoneal Pregnancy
Takuto Maekawa, Senn Wakahashi, Kenta Obata, Koki Moriuchi, Yutoku Shi, Yuki Sasagawa, Satoshi Nagamata, Masashi Nishimoto, Motoyoshi Maruo, Yoshito Terai

TL;DR
A rare case of choriocarcinoma was diagnosed and successfully treated with chemotherapy after being mistaken for an ectopic pregnancy.
Contribution
Highlights the importance of histopathological examination in suspected ectopic pregnancies to enable timely chemotherapy for choriocarcinoma.
Findings
Primary peritoneal choriocarcinoma was confirmed through histology and immunohistochemistry.
The patient achieved sustained hCG normalization and no recurrence after MEA chemotherapy.
Prompt chemotherapy is critical for choriocarcinoma due to its chemosensitivity.
Abstract
Extrauterine choriocarcinoma is uncommon and may be mistaken for a ruptured ectopic pregnancy. Rapid diagnosis is essential, as massive intraperitoneal bleeding can be fatal. Once histologically diagnosed, choriocarcinoma is highly chemosensitive. This case describes a 38-year-old woman who presented with sudden lower abdominal pain. Six weeks after her last menstrual period, serum human chorionic gonadotropin (hCG) was 28,834 mIU/mL. No intra-uterine gestational sac was found, and intraperitoneal bleeding was observed, suggesting an ectopic pregnancy. An emergency laparoscopic surgery revealed a blood clot and active bleeding on the peritoneal surface near the ileocecal region, which was resected. Histology revealed sheets of syncytiotrophoblasts and intermediate trophoblast cells without villi, and immunohistochemistry was diffusely positive for Ki-67 and hCG, confirming primary…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
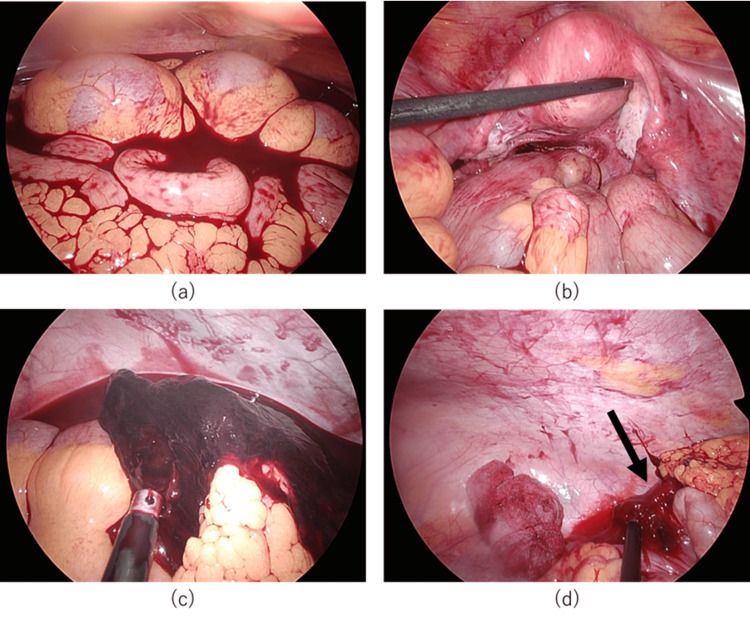 Figure 1
Figure 1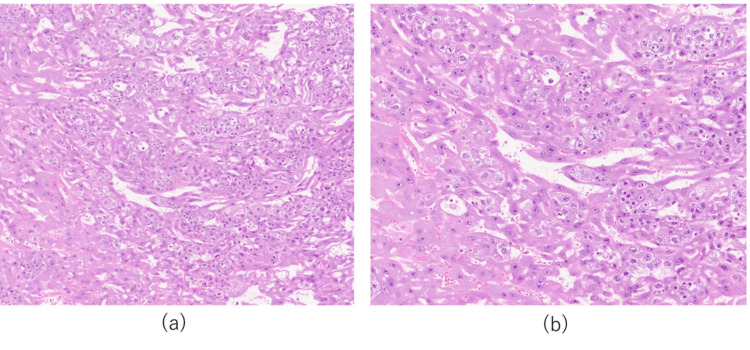 Figure 2
Figure 2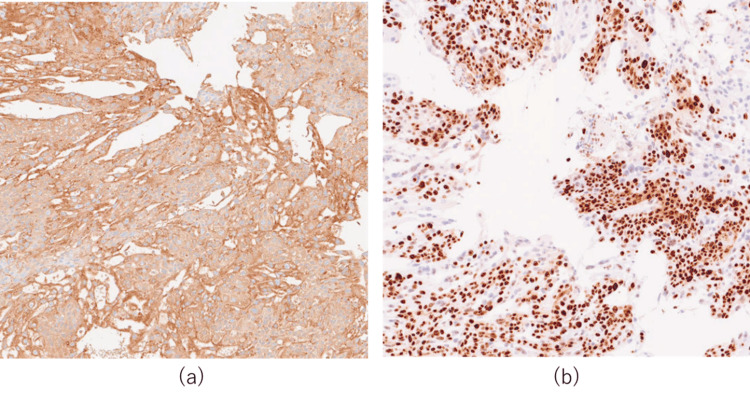 Figure 3
Figure 3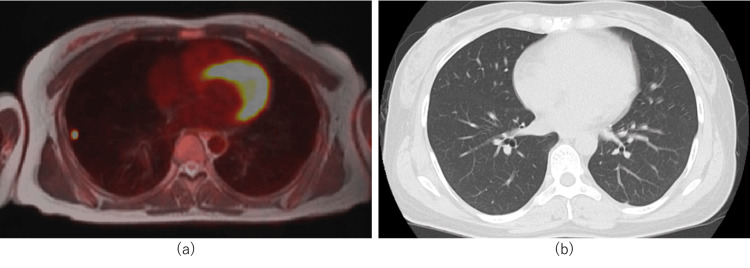 Figure 4
Figure 4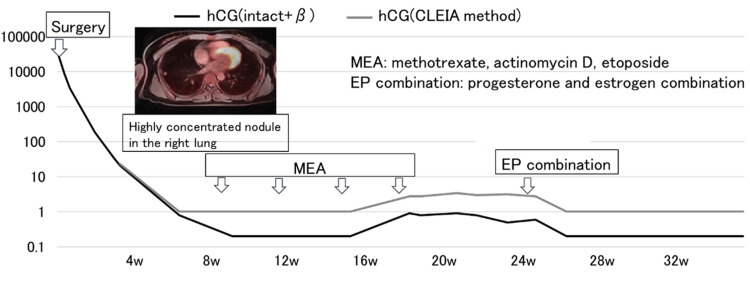 Figure 5
Figure 5| Parameter | Value | Reference range |
| WBC | 8,360 | 3,300-8,600 /μL |
| RBC | 4.73×106 | 3.86-4.92×106 /μL |
| Hb | 11.9 | 11.6-14.8 g/dL |
| PLT | 21.7×104 | 15.8-34.8×104/μL |
| AST | 11 | 13-30 U/L |
| ALT | 9 | 7-30 U/L |
| LD | 142 | 124-222 U/L |
| ALP | 35 | 38-113 U/L |
| BUN | 8.4 | 8-20 mg/dL |
| CRE | 0.75 | 0.46-0.70 mg/dL |
| hCG | 28,834 | mIU/ml |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGestational Trophoblastic Disease Studies · Ectopic Pregnancy Diagnosis and Management · Prenatal Screening and Diagnostics
Introduction
Choriocarcinoma can occur after any event during pregnancy: 50% after molar pregnancy, 25% after miscarriage or tubal pregnancy, and 25% after full-term or premature birth. The incidence of choriocarcinoma is approximately 3 cases per 100,000 births in Europe and North America but approximately 23 cases per 100,000 births in Southeast Asia. The risk increases with maternal age [1,2]. The definitive diagnosis of choriocarcinoma was based on the histological examination. However, in extrauterine choriocarcinoma, no lesions are found in the uterus, and there are no symptoms, such as abnormal uterine bleeding, making it difficult to suspect choriocarcinoma. It is often discovered because of symptoms or bleeding of metastatic lesions, such as pulmonary hemorrhage, gastrointestinal hemorrhage, intraperitoneal hemorrhage, and cerebral hemorrhage, and histological diagnosis is not easy. The clinical presentation is similar to ectopic pregnancy, so some rare pelvic lesions may be misdiagnosed as ectopic pregnancy [3]. Therefore, even in cases of suspected ectopic pregnancy, pathological diagnosis is important, and the possibility of choriocarcinoma must be considered and treated [3]. Here, we report a case in which laparoscopic surgery was performed for a suspected peritoneal pregnancy, and the pathological diagnosis was choriocarcinoma.
Case presentation
The patient was a 38-year-old woman, gravida 3, para 2 (2 full-term births, 1 induced abortion). Her previous pregnancy was a full-term birth at 29 years old. There was nothing to note in her medical or family history.
She visited our hospital complaining of lower abdominal pain. She tested positive for pregnancy and was thought to be at six weeks since her last menstrual period. Ultrasound findings showed no gestational sac in the uterus, but fluid retention suggestive of blood clots was observed in the Douglas and vesicouterine pouches. Laboratory findings are shown in Table 1.
An ectopic pregnancy was suspected, and emergency laparoscopic surgery was performed. Observation of the abdominal cavity revealed significant bloody ascitic fluid. No abnormal findings were observed in the uterus or adnexa. A 20 mm blood clot was found near the ileocecal area. After the clot was removed, active bleeding was observed from outside the ascending colon near the ileocecal area. This area was considered to be the site of peritoneal pregnancy; the ileocecal area was mobilized, and the affected area was excised and removed from the body. The operative time was 4 h and 13 min, respectively. Intraoperative blood loss was 1450 ml (Figure 1).
Intra-abdominal findings at laparoscopic surgery(a) Significant bloody ascites. (b) No abnormal findings were found in the uterus or bilateral adnexa. (c) A 20 mm blood clot was found near the ileocecal area. (d) Active bleeding was observed from outside the ascending colon near the ileocecal area.
The pathological findings of the excised tissue showed a large amount of blood clots, proliferation of acidophilic multinucleated syncytiotrophoblast cells, and proliferation of intermediate-type trophoblast cells with round nuclei and clear cytoplasm. In addition, no villous structures were observed, and based on these findings, the diagnosis was choriocarcinoma (Figure 2) [4].
Histopathological examination of the resected tissue (H&E staining) (a) 200×magnification; (b) 400×magnification; (a–b) Histology of the excised tissue showing the proliferation of syncytiotrophoblast cells and intermediate trophoblast cells
HCG and Ki67 staining was diffusely positive in syncytiotrophoblast cells, which supports the diagnosis of choriocarcinoma (Figure 3) [4,5].
Immunohistochemical staining for hCG and Ki-67(a-b) 200×magnification; (a-b) Histology of the excised tissue showing positivity for (a) HCG and (b) Ki67 in syncytiotrophoblast cellshCG: human chorionic gonadotropin
The pathological diagnosis was choriocarcinoma. A positron emission tomography (PET)-CT scan revealed a nodule with high uptake in the right lung; however, a subsequent contrast CT scan revealed no obvious nodule in the right lung (Figure 4).
PET-CT and contrast CT of the lung(a) A positron emission tomography (PET)-CT scan revealed a nodule with a high uptake in the right lung; (b) a contrast CT scan revealed no obvious nodule in the right lung
In addition, no findings suggestive of distant or lymph node metastasis were found. MEA therapy (methotrexate 450 mg/body on day 1, etoposide 100 mg/body on days 1-5, and actinomycin D 0.5 mg/body on days 1-5) was initiated. Four courses of MEA therapy were administered every three weeks. hCG levels remained negative; however, after the third course of MEA, low-unit hCG levels persisted. Considering the possibility of pituitary hCG based on estradiol (E2), follicle-stimulating hormone (FSH), and luteinizing hormone (LH) levels, a combination of luteinizing and estrogen hormones (EP combination) was administered, and the hCG level was negative (Figure 5).
Treatment progress and serum hCG levelsSerum hCG levels during MEA therapy and subsequent EP therapy. Low-level hCG elevation after the third MEA cycle suggested a pituitary origin, which resolved following EP therapy.hCG: human chorionic gonadotropin; MEA: methotrexate, etoposide, actinomycin D; EP: luteinizing and estrogen hormones
Thereafter, follow-up observation was continued, and no recurrence was observed.
In some cases, low levels of hCG persist without increasing after treatment for gestational trophoblastic neoplasia, which may be due to pituitary hCG levels. In this case, it was thought that there was a high possibility of pituitary hCG; therefore, a combination of progesterone and estrogen was administered, and the hCG level became negative. If low levels of hCG persist, invasive mole or choriocarcinoma may be suspected, and chemotherapy may be considered, but the possibility of pituitary hCG must be considered [1,4,6].
Discussion
The peritoneum is a rare site for primary choriocarcinoma development. Only nine reported cases of primary peritoneal choriocarcinoma have been reported [7].
Choriocarcinoma is primarily diagnosed by histological examination, but extrauterine choriocarcinoma is difficult to detect because there are no lesions in the uterus, and symptoms are unlikely to appear [8]. Uterine choriocarcinoma has lesions in the uterus, symptoms such as abnormal uterine bleeding are present, and histological diagnosis is possible; however, extrauterine choriocarcinoma has lesions in areas where ectopic pregnancy can occur; no lesions are found in the uterus, and there is no abnormal uterine bleeding, making it difficult to suspect the onset of choriocarcinoma. It is often discovered because of symptoms or bleeding from metastatic lesions, and a histological diagnosis is difficult [8]. When a diagnosis cannot be made by tissue testing, it is made using scoring such as the FIGO (International Federation of Gynecology and Obstetrics) risk score. However, there is a risk that the FIGO risk score will not result in a diagnosis of clinical choriocarcinoma [9]. Without a tissue diagnosis, there was a high possibility that the hCG levels would have continued to be monitored; therefore, obtaining a tissue diagnosis made it possible to intervene early. Choriocarcinoma is treated well with chemotherapy, and with MEA therapy, the initial remission rate is 75-88%, with a recurrence rate of 4-10%.
Peritoneal pregnancy can cause heavy bleeding, and in this case, it was difficult to confirm the location of the pregnancy and stop bleeding [10]. Extrauterine choriocarcinoma of primary peritoneal origin is rare, but in cases where ectopic pregnancy is suspected, accompanied by intraperitoneal bleeding, careful observation of the abdominal cavity and pathological diagnosis are considered important.
In cases in which ectopic pregnancy is suspected, pathological diagnosis is important, and the possibility of choriocarcinoma should be considered. It is also important to keep in mind that choriocarcinoma can occur secondary to pregnancy.
Conclusions
Choriocarcinoma occurs in a small percentage of cases of hydatidiform mole, but it can occur after any pregnancy, including normal delivery and miscarriage. In this study, we observed cases in which laparoscopic surgery was performed for suspected ectopic pregnancy, and intraoperative findings suggested a peritoneal pregnancy, but postoperative pathological diagnosis revealed choriocarcinoma.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Epidemiology, diagnosis, and treatment of gestational trophoblastic disease: A Society of Gynecologic Oncology evidence-based review and recommendation Gynecol Oncol Horowitz NS Eskander RN Adelman MR Burke W 60561316320213468635410.1016/j.ygyno.2021.10.003 · doi ↗ · pubmed ↗
- 2Advances in the diagnosis and early management of gestational trophoblastic disease BMJ Med Joyce CM Fitzgerald B Mc Carthy TV Coulter J O'Donoghue K 01202210.1136/bmjmed-2022-000321 PMC 997873036936581 · doi ↗ · pubmed ↗
- 3Misdiagnosis of gestational trophoblastic neoplasia as ectopic pregnancy: a 15-year retrospective study Front Med (Lausanne) Xiao P Guo T Yin R 1018573920223640557910.3389/fmed.2022.1018573 PMC 9667102 · doi ↗ · pubmed ↗
- 4Guidelines for treatment of uterine body neoplasm Endometrial Cancer Treatment Guidelines 2023 Edition (In Japanese) Japan Society of Gynecologic Oncology Tokyo Japan Society of Gynecologic Oncology (JSGO)Tokyo 2023 https://jsgo.or.jp/guideline/taiganguide 2023.html
- 5Ki-67 labeling index in the differential diagnosis of exaggerated placental site, placental site trophoblastic tumor, and choriocarcinoma: a double immunohistochemical staining technique using Ki-67 and Mel-CAM antibodies Hum Pathol Ming Shih IE Kurman RJ 2733291998944513010.1016/s 0046-8177(98)90386-0 · doi ↗ · pubmed ↗
- 6Gestational trophoblastic diseases: 4. Presentation with persistent low positive human chorionic gonadotropin test results Gynecol Oncol Cole LA Khanlian SA Giddings A Butler SA Muller CY Hammond C Kohorn E 16517210220061663124310.1016/j.ygyno.2005.12.048 · doi ↗ · pubmed ↗
- 7Short tandem repeat polymorphism analysis for primary peritoneal choriocarcinoma: a case report and literature review J Obstet Gynaecol Res Yamauchi K Sato Y Usui H Sakurai A Harada R Goto M 264026464820223577531710.1111/jog.15347 · doi ↗ · pubmed ↗
- 8The General Rules for Clinical and Pathological Management of Trophoblastic Diseases (The 3rd edition) (In Japanese)The General Rules for Clinical and Pathological Management of Trophoblastic Diseases (The 3rd edition) Japan Society of Obstetrics and Gynecology Tokyo The Japanese Pathological Society 2011 https://www.kanehara-shuppan.co.jp/books/detail.html?isbn=978430730108423156334 · pubmed ↗