Use of the International Classification of Diseases to Perinatal Mortality (ICD-PM) with verbal autopsy to determine the causes of stillbirths and neonatal deaths in rural Cambodia: a population-based, prospective, cohort study
Kaajal Patel, Sopheakneary Say, Daly Leng, Sophanou Khut, Sothearith Duong, Chou Ly, Arthur Riedel, Koung Lo, Verena Carrara, Claudia Turner

TL;DR
This study uses verbal autopsy and a new classification system to identify causes of stillbirths and neonatal deaths in rural Cambodia, highlighting major causes like hypoxia and infection.
Contribution
The study adapts the ICD-PM classification system for use with verbal autopsy data to better understand perinatal mortality in low-resource settings.
Findings
Hypoxia was the leading cause of intrapartum stillbirths (78.3%).
Infection was the main cause of late neonatal deaths (51.4%).
ICD-PM adaptations were needed to address unknown timing of death in stillbirths.
Abstract
Perinatal mortality remains a significant global health challenge, particularly in low- and middle-income countries (LMICs). Accurate cause-of-death data are essential to inform effective interventions but are often scarce. This study aimed to identify causes of stillbirths and neonatal deaths in rural Cambodia using verbal autopsy (VA) and the WHO International Classification of Diseases to Perinatal Mortality (ICD-PM). A four-year prospective study (2018–2022) in Preah Vihear province, Cambodia, established a community health worker-based pregnancy surveillance system. Verbal autopsy was conducted on stillbirths and neonatal deaths, with dual physician analysis to interpret VA data. To classify causes of death, ICD-PM was applied with adaptations made for stillbirths with unknown timing of death. A total of 522 deaths (229 stillbirths, 293 neonatal deaths) were recorded, and 79.1%…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
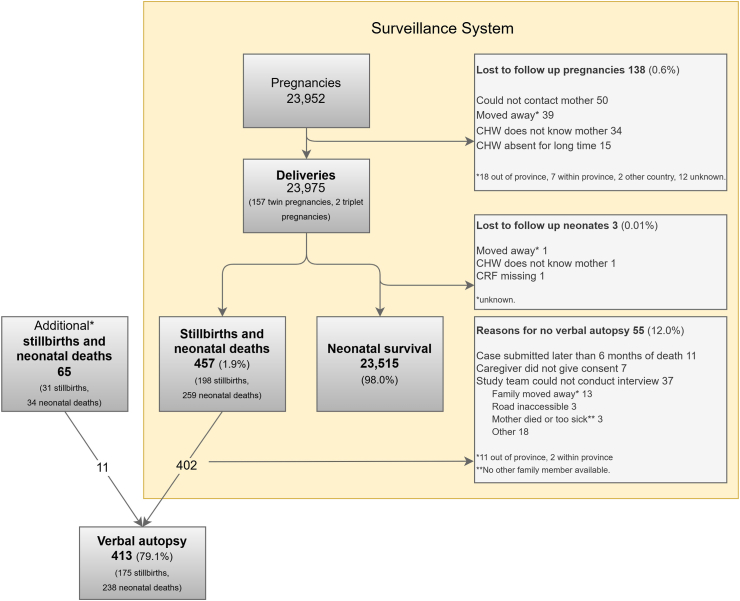 Figure 1
Figure 1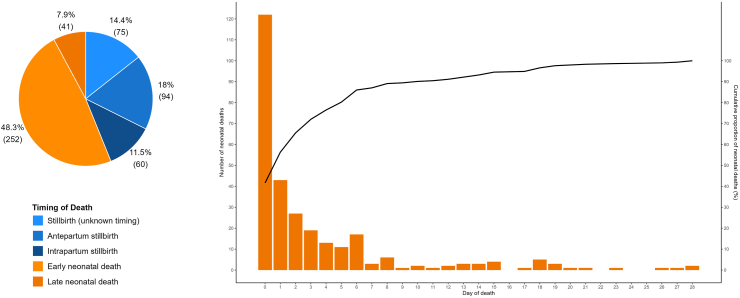 Figure 2
Figure 2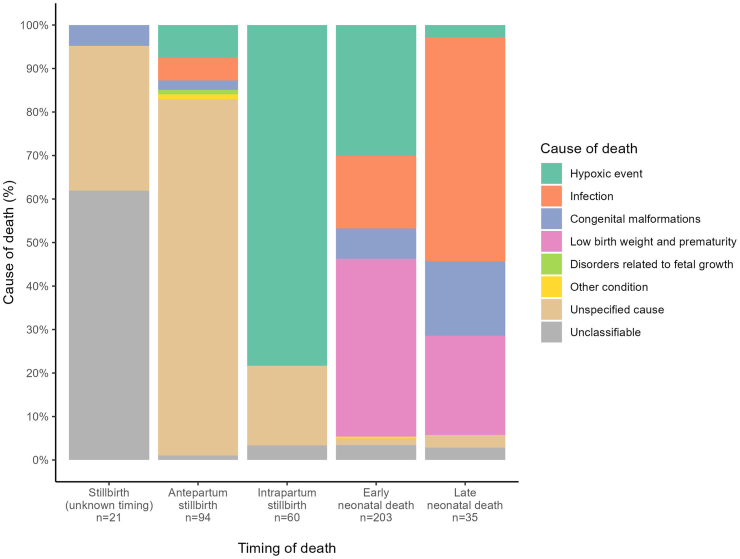 Figure 3
Figure 3- —Angkor Hospital for Children
- —Civil Society in Development
- —Fu Tak Iam Foundation
- —Manan Trust
- —T&J Meyer Family Foundation
- —Vitol Foundation
- —IF Foundation
- —10.13039/100010269Wellcome Trust
- —10.13039/100010269Wellcome Trust
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Maternal and Child Health · Global Health and Epidemiology · Child Nutrition and Water Access
Research in contextEvidence before this studyIn low- and middle-income countries, accurate and comprehensive causes of perinatal death data are scarce, making it difficult to identify and monitor effective interventions. In Cambodia, there is a paucity of good quality, large-scale perinatal data, especially for causes of death.The WHO's International Classification of Diseases to Perinatal Mortality (ICD-PM) was developed to improve the uniform reporting of causes of perinatal deaths. A recent systematic review on the global use of ICD-PM found that only 6% of deaths were from low-income settings and all applied ICD-PM to facility-derived data. Thus, in low-income settings where the vast majority of perinatal deaths occur, the relative representation of reported experience describing causes of deaths with ICD-PM is severely lacking.Added value of this studyTo the best of our knowledge, this is the first study to report the use of ICD-PM with verbal autopsy (VA) to classify perinatal deaths. We found that it is not only feasible, but also very useful, to use the ICD-PM tool to classify deaths on VA-derived data, but only with adaptations. The multilayered approach facilitated cause of death classification, even when data were less detailed, and was also useful with dual physician analysis when timing of death was agreed upon but the primary cause of death was unclear.Implications of all the available evidenceOur study provides the most comprehensive report of perinatal epidemiology in Cambodia, providing essential data for programme development and policy-makers. Our study shows that ICD-PM in it's current form requires adaptation to fulfil its potential to be globally applicable. In particular, ICD-PM needs the capacity to include cases where timing of death is unknown, as is common with VA-derived data. We recommend revision of ICD-PM to make it more applicable for low-resource settings. Until such revisions are made, we encourage users in similar contexts to adapt ICD-PM to their local context and methodologies. Our findings suggest that an adapted version of ICD-PM applied to VA data could significantly contribute to global efforts to report standardised perinatal mortality data and reduce perinatal mortality.
Introduction
Despite increased global focus and investment, perinatal mortality remains unacceptably high, amounting to 2.3 million neonatal deaths a year globally, with low- and middle-income countries (LMICs) carrying the vast burden.1 To address this urgent global health challenge, population-level perinatal mortality data are needed to inform programmes and policy, particularly given limited resources. Knowledge of how many, who, where, and why deaths are occurring allows for targeted interventions, especially important for perinatal deaths, which are mostly preventable with available, inexpensive interventions.2
Perinatal mortality data comprise mortality rates, as well as timing and causes of deaths. To be meaningful, cause of death data need to be accurate, reliable, feasible, relevant, and comparable across different settings. However, in areas with the highest perinatal mortality, the quality of data is poorest: less than 3% of perinatal deaths in LMICs achieve complete recording and certification3 compared to more than 90% in high-income countries.4
A civil registration and vital statistics (CRVS) system is the international gold standard for generating reliable, comprehensive, and timely statistics on all births and deaths in a population. Well-functioning CRVS systems are associated with better health outcomes.5 Despite its importance, emphasised by a Sustainable Development Goal focussing on improving CRVS,6 CRVS systems remain weak in many LMICs, resulting in poor quality perinatal mortality rate and cause of death data. This is for two main reasons. Firstly, many births and especially deaths occur without contact with the health system, resulting in millions of births and deaths never being officially recorded, and referred to as a ‘scandal of invisibility’.7^,^8 Secondly, weak health systems can mean facility-based births and deaths remain unrecorded, records are lost, and/or causes of deaths are inaccurate.
While CRVS systems in Cambodia are still developing, perinatal mortality rate estimates are available from demographic health surveys (DHS).9^,^10 However, the Cambodian DHS lacks data on timing of stillbirths (antepartum or intrapartum) and causes of perinatal deaths. Data on perinatal causes of death in Cambodia are scarce, derived mainly from small studies and estimates.11, 12, 13, 14 The limited availability and quality of these data necessitate reliance on estimates in perinatal epidemiology.15^,^16 However, there is increasing recognition that direct measurement, not estimation, is essential for accurate mortality data.17
In low-resource settings, robust yet feasible interim solutions are needed to provide mortality data until CRVS systems are strengthened. Surveillance and verbal autopsy (VA) are prominent strategies to find births and deaths and determine causes of deaths respectively.18 Population-based pregnancy surveillance systems aim to prospectively identify all relevant cases and follow them up for a defined time period to establish pregnancy outcomes and collect relevant data. Verbal autopsy involves data collection on the events preceding death, collected via interviews with families of the deceased, and then data analysis to determine the cause of death for each case.
Perhaps surprisingly given the necessity of consistent and comparable data to tackle perinatal mortality, a standardised global classification system to define perinatal causes of deaths was only introduced in 2016: the WHO application of ICD-10 to perinatal deaths: the ICD-perinatal mortality classification system (ICD-PM).19 ICD-PM uses a three-step approach to first determine the timing of death (antepartum, intrapartum, or postpartum/neonatal), second determine the primary medical cause of death, and third determine the contributing maternal condition.19^,^20
A recent systematic review found that ICD-PM had been applied in low-income settings to only 6% (2556/45,735) of perinatal death cases, which exclusively comprised hospital data.21 To the best of our knowledge, ICD-PM has never been applied to population-based data collected via VA. This is an important gap due to the significant proportion of home deliveries and deaths, as well as unreliable health records, where the burden of perinatal deaths is greatest. For ICD-PM to be truly globally comparable, relevant, and useful to perinatal death reduction efforts, reporting on experiences of its application to population-based, VA-derived data is essential.
The primary objective of this study was to determine the underlying causes of stillbirths and neonatal deaths in rural Cambodia, using a population-based pregnancy surveillance system combined with VA and the WHO's ICD-PM classification system. We also aimed to describe the feasibility, strengths, and limitations of ICD-PM when used with VA-derived data, which has not been previously rigorously examined in population-based, low-resource contexts.
Methods
This was a prospective observational study covering the whole of Preah Vihear province, in North-Eastern Cambodia, over four years (1st September 2018–31st August 2022). This study was nested within the Saving Babies' Lives (SBL) implementation research programme.22 SBL is a cluster-randomised trial to evaluate a package of interventions aiming to reduce perinatal mortality in Preah Vihear province. Population-based pregnancy surveillance identified all births and deaths before 28 days of life. Verbal autopsy was conducted with ICD-PM to classify causes of stillbirths and neonatal deaths. A social autopsy component was later added, the results of which are published separately.23
Study setting
Preah Vihear is a large, rural province comprising 1.6% of Cambodia's population (254,827 in 2019).24 Before this study, birth registration amongst children under five was 66.5% in the province, below the national average of 73.3%.9 No data were available on birth registration by the end of the neonatal period or on death registration.
Primary healthcare in Cambodia is supported by a network of community health workers (CHWs), typically two per village. As trained laypeople, CHWs cover all 289 villages in Preah Vihear province, each serving approximately 441 people. Although they often track pregnant women in their village informally, CHWs have no formal role in reporting births or deaths, and do not usually attend deliveries.
Surveillance
A neonatal surveillance system harnessing the existing CHW network was set up to cover all deliveries and deaths before the first four weeks of life. CHWs were trained to identify, take verbal consent, and collect data on all pregnancies ≥28 weeks gestation from their respective village, and then follow up the pregnancies until 28 days of life. All deliveries ≥28 weeks gestation (determined from last menstrual period, otherwise birth weight ≥1000 g was used) of women living in and/or delivering in the study area during the study date range were included.
CHWs used a paper-based case record form (CRF) to collect data on estimated delivery date, birth details (date, place, sex, gestation, birth weight, multiple birth), and pregnancy outcome. Outcomes were defined as stillbirth (baby born with no signs of life), neonatal death (death during the first 28 completed days of life) or neonatal survival. Training and familiarisation with the CRF was provided prior to study start. On a monthly basis, the study team met with CHWs and entered the CRF data into a tablet-based electronic form developed using KoboToolbox.25 Overdue outcomes were monitored and the relevant CHW prompted accordingly. Missing and unfeasible data checks were done to allow timely clarification with the relevant CHW. CHWs received $2USD per completed CRF to compensate for time and expenses incurred.
Additional deaths
Due to resource constraints, we focused on finding deaths missed by the surveillance system. In Cambodia, families are legally required to register births and deaths with their local authority (commune council), but we found few births and no stillbirths or neonatal deaths recorded and so did not pursue this data source further. Instead, we reviewed all facility records in the study area annually for stillbirths and neonatal deaths, and cross-checked these with surveillance data to identify additional deaths. Any newly found cases were followed up by the designated CHW. If the family could not be located, the available facility data were used to record the death.
Verbal autopsy
A VA was performed by the study team within six months of all stillbirths and neonatal deaths, and physician analysis used to assign cause of death using the ICD-PM classification system.
To collect data, we adapted the 2016 WHO VA questionnaire for stillbirths and neonatal deaths to our context and purpose (Appendix 1).26^,^27 A tablet-based, electronic version of the questionnaire was developed in both English and Khmer (the national language) using KoboToolbox.25 CHWs helped organise the interviews, which were held in privacy (mostly in the family home) with at least one parent and/or close family member who was present during the time preceding death. Following informed consent, interviews were conducted by the trained Cambodian study team in Khmer, which is the usual spoken language in the study area except for near the Laos border. Completed VAs were checked weekly for completion and logic to allow for timely clarification as needed.
To determine cause of death from VA data collected, we used dual physician analysis. This is the accepted best method for VA analysis, especially for research studies and settings where many deliveries and deaths occur outside of the formal health system.28^,^29 The trained, consistent coding team comprised three paediatricians: a Cambodian-trained and a UK-trained senior registrar who independently assigned cause of death to all VA cases, and a UK-trained consultant with expertise in tropical medicine and obstetrics who independently assigned cause of death only in cases of discrepancy. All three coders were based in Cambodia prior to and throughout the study, and familiar with the local context. A diagnosis of ‘unclassifiable’ was used when agreement between all three physician coders was not achieved.
ICD-PM
To classify the causes of stillbirths and neonatal deaths we used the WHO ICD-PM classification system.19 We adapted the coding system to our context and purpose (Table 1, Appendix 2). The main adaptation was the addition of a fourth major category for the timing of death: ‘U’ for unknown timing of stillbirth in relation to the onset of labour. Subsequent U sub-categories (U1–U6) followed the existing ICD-PM codes for antepartum stillbirths and those used in previous studies to ensure they were relevant and comparable.21^,^30 We also developed rules for assigning codes that were difficult to differentiate due to a lack of diagnostics and clinical information, such as birth asphyxia (N4) and hypoxic ischaemic encephalopathy (N5) (Appendix 2).Table 1ICD-PM codes and descriptions adapted and used to classify causes of stillbirths and neonatal deaths in our study.ICD-PM codeDescriptionStep 1Timing of deathUUnknown timing of death in relation to labour onset, died before deliveryADead before/at the onset of labour, died before deliveryIAlive at onset of labour, died before deliveryNAlive at delivery, died before 28 days of lifeTiming of deathICD-PM codeDescriptionStep 2UStillbirth of unknown timingU1Congenital malformations, deformations, and chromosomal abnormalitiesU2In utero hypoxiaU3InfectionU4Other specified in utero disorderU5Disorders related to foetal growthU6In utero death of unspecified causeAAntepartum stillbirthA1Congenital malformations, deformations, and chromosomal abnormalitiesA2InfectionA3Antepartum hypoxiaA4Other specified antepartum disorderA5Disorders related to foetal growthA6Antepartum death of unspecified causeIIntrapartum stillbirthI1Congenital malformations, deformations, and chromosomal abnormalitiesI2Birth traumaI3Acute intrapartum eventI4InfectionI5Other specified intrapartum disorderI6Disorders related to foetal growthI7Intrapartum death of unspecified causeNNeonatal deathN1Congenital malformations, deformations, and chromosomal abnormalitiesN2Disorders related to foetal growthN3Birth traumaN4Complications of intrapartum eventsN5Convulsions and disorders of cerebral statusN6InfectionN7Respiratory and cardiovascular disordersN8Other neonatal conditionsN9Low birth weight and prematurityN10MiscellaneousN11Neonatal death of unspecified causeICD-PM code****DescriptionStep 3Maternal contributing conditionM1Complications of placenta, cord, and membranesM2Maternal complications of pregnancyM3Other complications of labour and deliveryM4Maternal medical and surgical conditionsM5No maternal condition
For each case we applied the ICD-PM in three steps (Table 1, Appendix 2):
- 1.Time of death major category: exact timing of death was classified as antepartum stillbirth (A), intrapartum stillbirth (I), unknown timing of stillbirth (U), or neonatal death (N).
- 2.Primary cause of death sub-category: for each timing category (A, I, U, N) medical cause of foetal or neonatal death was coded as A1–A5, I1–I7, U1–U6, N1–N11.
- 3.Contributing maternal condition category: main maternal condition or disease considered to have contributed to death was coded as M1–M5.
Only one primary cause of death and one maternal condition was permitted: this was considered to be the earliest condition in the chain of events ending in death. When physician coders did not agree on the primary cause of death, but did agree on the time of death code, only the major timing of death code (U, A, I, N) was reported and the primary cause described as ‘unclassifiable’. When the coders did not agree on the maternal contributing condition, this was also reported as ‘unclassifiable’.
The ICD-PM system is designed to be used for deaths in the perinatal period: all stillbirths and early (within the first seven days) neonatal deaths. However, ICD-PM can also be used for late neonatal deaths as these may also occur as a consequence of perinatal events.19 Thus, for deaths assigned a neonatal (N) code, we report their ICD-PM codes split by timing of death, defined as before and after the first seven completed days of life (early and late neonatal deaths respectively).
Data analysis
All data were entered on KoboCollect25 and analysis was performed using the R software package.31 Additional deaths discovered from facility records and not from the surveillance system were excluded both from mortality rate calculations due to their unknown denominator, and from comparison of characteristics of deliveries that survived with those that died. Due to few missing data (3.6% for the multivariable analysis), complete case analysis was performed. Causes of deaths were described as cause-specific mortality fractions (CSMFs), the accepted metric in the field.32 For physician analysis, acceptable inter-rater variability was predefined as equal to or more than 60% and assessed using Cohen's Kappa statistic. Descriptive analyses included frequencies, percentages, and rates. Relative risks with 95% confidence intervals were calculated to assess associations between perinatal risk factors and death. Potential selection bias was assessed by comparing characteristics of VA enrolled and non-enrolled cases.
Ethics approval
The sensitive nature of VA required careful ethical consideration. Verbal autopsy was conducted after allowing for a mourning period, and confidentiality of cases and of participant views was maintained at all times. The study was approved by the Cambodian National Ethics Committee for Health Research (NECHR, 283) and the Oxford Tropical Research Ethics Committee (OxTREC, 547–17). Verbal autopsy interviews were done after obtaining informed verbal consent from caregivers of the deceased. Verbal consent was witnessed by another study team member and documented via the VA digital tool. The tool ensured that the interviewer could not progress with the interview until verbal consent was obtained.
Role of the funding source
Angkor Hospital for Children participated in the design of the study, data collection, analysis and interpretation, and in the writing of this manuscript; the other funding bodies did not.
Results
There were 23,975 deliveries and 457 deaths (198 stillbirths and 259 neonatal deaths) recorded by the surveillance system during the study (Fig. 1). The overall stillbirth rate, neonatal mortality rate, and perinatal mortality rate were 8.3 per 1000 deliveries, 10.9 per 1000 live births, and 17.4 per 1000 deliveries respectively.Fig. 1. Flowchart of stillbirths and perinatal deaths. Community health worker (CHW); case record form (CRF). ∗additional death cases found from health facility records.
Baseline characteristics of all deliveries found via surveillance are shown in Table 2. Most deliveries occurred in primary (63.2%) and secondary (21.6%) government-run facilities in the province and 5.5% of deliveries occurred in the community. Death (both stillbirths and neonatal deaths) was associated with male sex, preterm (<37 weeks gestation) delivery, low birth weight, and being born in the community (Appendix 3).Table 2. Characteristics of deliveries ≥28 weeks gestation, stratified by outcome: Deceased (stillbirths and neonatal deaths) or neonatal survival.CharacteristicDeceased N = 457Neonatal survival N = 23,515Overall N = 23,972Male sex, n (%)278 (61.2%)12,175 (51.8%)12,453 (52.0%) Missing303Preterma, n (%)232 (50.9%)717 (3.1%)949 (4.0%) Missing13435Birth weight (kg), median (IQR)2.30 (1.50, 3.00)3.00 (2.80, 3.30)3.00 (2.80, 3.30) Missing88758846Multiple births, n (%)28 (6.1%)283 (1.2%)311 (1.3%) Missing000Birth location, n (%) Home54 (11.8%)1266 (5.4%)1320 (5.5%) Enroute22 (4.8%)0 (0.0%)22 (0.1%) Primary170 (37.2%)14,973 (63.7%)15,143 (63.2%) Secondary150 (32.8%)5029 (21.4%)5179 (21.6%) Private6 (1.3%)384 (1.6%)390 (1.6%) Other2 (0.4%)67 (0.3%)69 (0.3%) Other province primary6 (1.3%)437 (1.9%)443 (1.8%) Other province secondary7 (1.5%)342 (1.5%)349 (1.5%) Other province tertiary (NGO)38 (8.3%)1012 (4.3%)1050 (4.4%) Other province private2 (0.4%)0 (0.0%)2 (0.0%) Missing055Birth location definitions: Enroute: deliveries that occurred whilst travelling to a facility; Primary: primary-level government healthcare facility; Secondary: government hospital; Private: privately-run health facility; Tertiary: tertiary-level non-governmental organisation (NGO)-run hospital. Birth locations were all in the study area (Preah Vihear province) unless stated as other province.aPreterm defined as <37 weeks gestational age.
Deaths
Overall, 522 deaths (229 stillbirths and 293 neonatal deaths) were found. Checking health facility records found 155 (29.7%, 155/522) stillbirths and neonatal deaths, of which 65 had not yet been identified by the surveillance system. Of these 65 additional deaths, data could be collected by CHWs for 30 cases, and 11 had a VA. Some differences were found in baseline characteristics between the 457 cases found by the CHW surveillance system and the additional 65 cases found from facility records (Appendix 4).
For stillbirth cases with a known timing of death, 61.0% (94/154) of stillbirths occurred antepartum (Fig. 2). The proportion of neonatal deaths occurring on the first day of life was 41.6% (122/293) and in the first week of life was 86.0% (252/293) (Fig. 2).Fig. 2. Death cohort (n = 522): timing of deaths.
Baseline characteristics of all deaths, stratified by the timing of their death, are shown in Appendix 5. Amongst the 522 deaths, 15.3% occurred in the community.
Verbal autopsy
Verbal autopsy was conducted on 413 of the 522 deaths (79.1%). Reasons for non-enrolment included deaths being reported too late (> six months), lack of consent, and logistical issues including road access issues and the family moving away (Fig. 1). We found no difference between the baseline characteristics of the VA enrolled and unenrolled population, except for in birth and death locations (Appendix 6). The median time from the date of death to VA interview was 54.0 days (IQR 30.0–91.0 days). By the time of VA interview, five mothers had died (two intrapartum and three postpartum). Excluding these five maternal death cases, the mother was the main respondent for 98.5% (402/408) of cases.
For 67 of the 413 (16.2%) VA cases no agreement on cause of death could be reached between the initial two physician analysers and so the case went to a third physician. Of these 67 cases, an agreement could be reached between two out of the three physicians for 44 cases. For all 23 cases for which physician agreement was not reached on the primary cause of death (unclassifiable), an agreement was reached on the timing of death and so the major code is reported (Table 3). Inter-rater reliability between the two primary physicians conducting physician analysis was 0.811, calculated using Cohen's Kappa statistic.Table 3ICD-PM coding of stillbirths and neonatal deaths.Maternal contributing conditionTotalM1M2M3M4M5MComplications of placenta, cord and membranesMaternal complications of pregnancyOther complications of labour and deliveryMaternal medical and surgical conditionsNo maternal conditionUnclassifiableUnknown timing of stillbirth U1-Congenital malformations0 (0.0%)0 (0.0%)0 (0.0%)0 (0.0%)1 (4.8%)0 (0.0%)1 (4.8%) U6-Unspecified cause0 (0.0%)0 (0.0%)0 (0.0%)1 (4.8%)6 (28.6%)0 (0.0%)7 (33.3%) U-Unclassifiable2 (9.5%)0 (0.0%)0 (0.0%)5 (23.8%)6 (28.6%)0 (0.0%)13 (61.9%) **Subtotal****2 (9.5%)****0 (0.0%)****0 (0.0%)****6 (28.6%)****13 (61.9%)****0 (0.0%)21 (100.0%)**Antepartum stillbirth A1-Congenital malformations0 (0.0%)0 (0.0%)0 (0.0%)0 (0.0%)2 (2.1%)0 (0.0%)2 (2.1%) A2-Infection1 (1.1%)0 (0.0%)0 (0.0%)4 (4.3%)0 (0.0%)0 (0.0%)5 (5.3%) A3-Antepartum hypoxia5 (5.3%)0 (0.0%)0 (0.0%)1 (1.1%)1 (1.1%)0 (0.0%)7 (7.4%) A4-Other condition0 (0.0%)0 (0.0%)0 (0.0%)1 (1.1%)0 (0.0%)0 (0.0%)1 (1.1%) A5-Disorders related to foetal growth0 (0.0%)0 (0.0%)0 (0.0%)1 (1.1%)0 (0.0%)0 (0.0%)1 (1.1%) A6-Unspecified cause2 (2.1%)3 (3.2%)0 (0.0%)5 (5.3%)66 (70.2%)1 (1.1%)77 (81.9%) A-Unclassifiable0 (0.0%)0 (0.0%)0 (0.0%)1 (1.1%)0 (0.0%)0 (0.0%)1 (1.1%) **Subtotal8 (8.5%)****3 (3.2%)****0 (0.0%)****13 (13.8%)****69 (73.4%)****1 (1.1%)94 (100.0%)**Intrapartum stillbirth I3-Intrapartum hypoxia4 (6.7%)4 (6.7%)37 (61.7%)1 (1.7%)0 (0.0%)1 (1.7%)47 (78.3%) I7-Unspecified cause0 (0.0%)0 (0.0%)1 (1.7%)1 (1.7%)9 (15.0%)0 (0.0%)11 (18.3%) I-Unclassifiable0 (0.0%)0 (0.0%)0 (0.0%)1 (1.7%)1 (1.7%)0 (0.0%)2 (3.3%) **Subtotal4 (6.7%)****4 (6.7%)****38 (63.3%)****3 (5.0%)****10 (16.7%)****1 (1.7%)****60 (100.0%)Stillbirth subtotal14 (8.0%)****7 (4.0%)****38 (21.7%)****22 (12.6%)****92 (52.6%)****2 (1.1%)175 (100.0%)**Early neonatal death N1-Congenital malformations0 (0.0%)1 (0.5%)0 (0.0%)1 (0.5%)11 (5.4%)1 (0.5%)14 (6.9%) N4-Intrapartum hypoxia10 (4.9%)3 (1.5%)32 (15.8%)0 (0.0%)13 (6.4%)3 (1.5%)61 (30.0%) N6-Infection0 (0.0%)0 (0.0%)3 (1.5%)4 (2.0%)24 (11.8%)3 (1.5%)34 (16.7%) N8-Other condition0 (0.0%)0 (0.0%)0 (0.0%)0 (0.0%)1 (0.5%)0 (0.0%)1 (0.5%) N9-Low birth weight and prematurity9 (4.4%)4 (2.0%)59 (29.1%)4 (2.0%)3 (1.5%)4 (2.0%)83 (40.9%) N11-Unspecified cause0 (0.0%)0 (0.0%)0 (0.0%)0 (0.0%)3 (1.5%)0 (0.0%)3 (1.5%) N-Unclassifiable0 (0.0%)0 (0.0%)1 (0.5%)1 (0.5%)4 (2.0%)1 (0.5%)7 (3.4%) **Subtotal19 (9.4%)****8 (3.9%)****95 (46.8%)****10 (4.9%)****59 (29.1%)****12 (5.9%)203 (100.0%)**Late neonatal death N1-Congenital malformations0 (0.0%)0 (0.0%)0 (0.0%)0 (0.0%)6 (17.1%)0 (0.0%)6 (17.1%) N4-Intrapartum hypoxia0 (0.0%)0 (0.0%)0 (0.0%)0 (0.0%)1 (2.9%)0 (0.0%)1 (2.9%) N6-Infection0 (0.0%)0 (0.0%)2 (5.7%)1 (2.9%)15 (42.9%)0 (0.0%)18 (51.4%) N9-Low birth weight and prematurity0 (0.0%)3 (8.6%)4 (11.4%)0 (0.0%)0 (0.0%)1 (2.9%)8 (22.9%) N11-Unspecified cause0 (0.0%)0 (0.0%)0 (0.0%)0 (0.0%)1 (2.9%)0 (0.0%)1 (2.9%) N-Unclassifiable0 (0.0%)0 (0.0%)0 (0.0%)0 (0.0%)1 (2.9%)0 (0.0%)1 (2.9%) **Subtotal0 (0.0%)****3 (8.6%)****6 (17.1%)****1 (2.9%)****24 (68.6%)****1 (2.9%)****35 (100.0%)Neonatal subtotal19 (8.0%)****11 (4.6%)****101 (42.4%)****11 (4.6%)****83 (34.9%)****13 (5.5%)****238 (100.0%)Total33 (8.0%)****18 (4.4%)****139 (33.7%)****33 (8.0%)****175 (42.4%)****15 (3.6%)**413 (100.0%)
Causes of deaths
Final CSMFs classified by ICD-PM codes are shown in Table 3 and Fig. 3. For 12.0% (21/175) of stillbirths the timing of the death in relation to the onset of labour could not be determined (U). No cause of death could be identified for 95.2% (20/21) of stillbirths of unknown timing, 83.0% (78/94) of antepartum stillbirths, but only 21.7% (13/60) of intrapartum stillbirths. For intrapartum stillbirths, hypoxia (78.3%, 47/60) was the leading (and only) cause identified.Fig. 3. Cause-specific mortality fractions by timing of death.
Most deaths occurred intrapartum and within the first seven days of life (63.7% (263/413)). During this critical time period the leading cause of death and associated maternal condition were hypoxia (41.1%, 108/263), and complications of labour and delivery (50.6%, 133/263) respectively (Appendix 7).
Four causes (low birth weight and prematurity, intrapartum hypoxia, infection, and congenital malformations) accounted for nearly all (94.5%, 225/238) neonatal deaths. Most early neonatal deaths were attributed to low birth weight and prematurity (40.9%, 83/203) and intrapartum hypoxia (30.0%, 61/203), and complications of labour and delivery (46.8%, 95/203) was the commonest maternal contributing condition. Most late neonatal deaths were attributed to infection (51.4%, 18/35), and only one case was attributed to hypoxia (2.9%); maternal contributing cause was largely unattributed (68.6%, 24/35). The CSMFs for neonatal deaths changed with progressing age, such that after 19 days of life, the only causes were infection and congenital abnormalities (Appendix 8).
Discussion
Our study provides the most comprehensive description of perinatal epidemiology in Cambodia. To the best of our knowledge, it is also the first reported study combining VA with ICD-PM for both stillbirths and neonatal deaths in both community and facility (all) settings.
Our stillbirth and neonatal mortality rates are lower than recently reported in Cambodia,14 although the perinatal mortality is the same as that reported in Preah Vihear province in the most recent Cambodian DHS.24
In keeping with global data, preterm and low birth weight complications were the leading cause of neonatal deaths in our setting.33 The only previous neonatal VA study in Cambodia found sepsis to be the leading cause, followed by asphyxia, but this study was based on only 12 neonatal deaths.13 Our findings confirm the emphasis on preterm labour as a global target to reduce perinatal mortality.34^,^35
Primary cause of death could not be ascertained for the majority of antepartum stillbirths and stillbirths of unknown timing, similar to experiences applying ICD-PM in other LMICs.30 Identifying causes of antepartum deaths in low-resource settings remains a global challenge as without this information, interventions cannot be targeted.36
Strengths & limitations: surveillance system
Community health worker surveillance of pregnancies was far superior to routinely-collected facility data at discovering deaths. Of all deaths, 84.7% occurred in a facility. However, had we relied solely on facility records, we would only have found 29.7% of deaths, suggesting that facilities were not recording these deaths. This is an important consideration for programmes in similar settings that use routinely-collected mortality data. However, the CHW surveillance system was not perfect: if we had only used surveillance, we would only have found 87.5% (457/522) of all deaths because it missed 65 deaths. Of the 522 deaths, 35 (6.7%) were never found by CHWs and only facility record data were used. Reasons for CHWs missing death cases include the movement of domestic economic migrants in and out of the province, families living in very remote farms for work, and concealment of pregnancy by unmarried women. Future programmes should consider triangulation of data if resources allow, and ideally should also include facility births to provide calculation of more comprehensive mortality rates.
Many VA unenrolled cases involved additional deaths found from facility records and initially missed by CHWs. Actively including health facility staff in our surveillance system might have resulted in reporting of these deaths sooner and improved our VA enrolment rate.
A strength of our surveillance system was harnessing the existing CHW network. Community health workers live amongst the communities they serve, making them accessible and trusted members of the health system.37 This might help to explain our high follow-up rate, high proportion of VA enrolment, and high reported home birth rate of 5.5% compared to 3.6% reported in Preah Vihear province.10 Our study highlights the importance of CHWs as an important resource in LMICs, particularly in rural and remote settings, to achieve inclusion of the most marginalised communities.
However, the challenge was the limited capacity for data collection as CHWs are busy people with work, family life, and other CHW responsibilities. For the surveillance system, therefore, we prioritised data quality and completeness of a few, core variables, which limited comparison between deceased and surviving babies. Also, lack of sociodemographic data limited our ability to assess the generalisability of results from the enrolled to the unenrolled population.
Another limitation was the lack of early, accurate, dating ultrasound scan results, which meant gestational age (≥28 weeks gestation) for study inclusion could not be verified.
The other major challenge of the pregnancy surveillance system was its resource-intensity, making it difficult to be sustained without significant funding, technical, and logistical support. Considerable resources are required to report truthful, accurate data in low-resource settings until routine data collection systems improve.
Strengths & limitations: verbal autopsy
Verbal autopsy is a resource-intensive epidemiological tool, especially combined with dual physician analysis. Another limitation of VA is its reliance solely on observation, perspective, and recall of family members present at the time of terminal illness. Potential for bias towards visible, untreated, and memorable pathology (such as visible congenital abnormalities and prematurity), especially when diagnostics and reliable medical records are lacking, might explain our limited variety of causes of death: we used only 18 out of 30 possible ICD-PM codes.
Antepartum stillbirths are particularly challenging, since diagnostics are needed for usually covert pathology, which might explain the high proportion (70.2%) of antepartum stillbirths with neither primary cause of death, nor maternal condition identified in our setting. Also, without diagnostics (antenatally and/or postnatally), the clinical manifestation of ‘invisible’ pathology might have led to misclassification. For example, a congenital cardiac defect in a term neonate manifesting as respiratory distress might have been misdiagnosed as infection. However, our findings are consistent with those from other LMICs.30
Additionally, 98.5% of respondents were mothers and with most deaths occurring around the time of delivery, their own condition might have affected their observation of events. Furthermore, perspectives can be context-specific; for example, neonatal jaundice is a poorly recognised medical problem in rural Cambodia.38
Lack of a ‘true’ gold standard to assess accuracy and validate our VA results is another limitation. Triangulation of data with healthcare worker perspectives, antenatal scans, or medical records was not feasible given that reports were often missing or of poor quality. However, VA as a tool has been validated, although there is less reported experience with stillbirths.18 Our findings are comparable to other studies in rural areas, including a multi-country VA study for stillbirths and early neonatal deaths.39
Strengths & limitations: ICD-PM
The ICD-PM system comprises the capacity to account for the unique set of circumstances that occur perinatally: firstly, the transition from the in utero foetal period to the ex utero neonatal period, and secondly the inextricable link between mother and baby. It summarises the complexity of perinatal causes of deaths into a concise four-character code (e.g., N9–M3).
We found the multilayered nature of the ICD-PM system to be a great strength because it allowed for classification from a broad to a more detailed level, according to the data available. This meant we could assign ICD-PM to all deaths, even when information from VA was limited or when physicians agreed on the major timing of death code (U/A/I/N) but disagreed on the primary cause of death code (unclassifiable). This maximised the number of cases contributing to perinatal death data, even if this was only timing of death.
We found linking deaths to maternal conditions to be a strength of ICD-PM, particularly in cases when the primary cause of death was unknown but a maternal contributing condition was identified. Thus, the code could still provide useful data to guide public health interventions.
For this study, given the limited availability of detailed information via VA, we accept the results of fewer and broader cause of death categories with relatively high proportions of unknowns. We do not consider a high proportion of unknowns for each of the three steps of the ICD-PM, and especially for antepartum stillbirths, to be a failure of the classification system, but rather a reflection of the context.
ICD-PM adaptation for use with verbal autopsy
The ICD-PM was developed to be applicable globally but wasn't piloted in a low-income setting, despite most deaths occurring here.40 Subsequent application globally has been mostly on facility data, mostly retrospective, and predominantly in high- and middle-income countries.21 We agree with the limited studies from low-resource settings that to be applicable globally, revisions to ICD-PM are both necessary and useful.21^,^30 Based on our experience of using ICD-PM with VA data to identify cause of death, our suggested amendments to the classification system are summarised below.
Most importantly, ICD-PM needs to have the capacity to account for an indeterminate timing of death. The step-wise application of ICD-PM means that without a major timing code, the subsequent cause of death code, even if known, cannot be assigned. As a result these cases would otherwise be excluded from global perinatal death reporting. In our study, 12.0% (21/175) of stillbirth cases were assigned a U code for unknown timing of stillbirth. Even when using hospital records, which might, for example, have documentation on intrapartum heart rate, a multi-country LMIC study assigned a U code to 7.3% (92 cases) of stillbirths.30 Since with VA methodology we relied solely on recall from family members, a higher U proportion is to be expected, and emphasises the need for addition of this code to the ICD-PM to make it applicable to VA-derived data. Of note, it can also be very challenging to differentiate between an intrapartum stillbirth and neonatal death within a few minutes of life, especially based on VA data and/or for home deaths.41 The ICD-PM also does not account for this unknown time period. Although we did not encounter the need for such a code in our study, it is worth considering for future ICD-PM revisions.
Finally, simplification of ICD-PM codes is a worthwhile consideration for future application to VA-derived data. We developed internal coding rules (Appendix 2) to reduce ambiguity and ensure consistency.
Implications for practice, policy, and research
Our findings indicate key intervention areas to reduce preventable perinatal deaths. These include promoting facility-based deliveries and strengthening healthcare delivery, particularly obstetric care at delivery, neonatal resuscitation, and care of small and preterm neonates.
The resource-intensity of our pregnancy surveillance system highlights the challenges of generating high-quality, community-level data to capture all births and deaths in low-resource settings. Whilst CRVS systems are strengthened in low-resource settings, leveraging existing community-based networks, especially those trusted by the community, can be invaluable in capturing information that would otherwise go unrecorded.
Adaptation of ICD-PM for use with VA and to our context was crucial for meaningful and consistent cause-of-death assignment. Quality improvement of ICD-PM with our VA tool was inbuilt during implementation (Appendix 2). Future application of ICD-PM to population-based, VA data should similarly consider and report context-specific adaptations to refine the tool.
Conclusion
The ICD-PM classification system can be applied to VA-derived data but only with adaptation. In particular, the capacity to account for unknown timing of stillbirth was crucial. With adaptation to our context, we found ICD-PM user-friendly, optimised inclusion of cases, and provided a comprehensive description of causes of deaths. Thus, our findings provide globally-comparable, relevant, and practical data for programme design and policy makers. To improve the standardisation of perinatal cause of death reporting in regions with the highest mortality rates, important ICD-PM revisions to make it better applicable in LMICs and with VA-derived data are needed.
Contributors
KP and CT conceptualised and designed the study. KP and CT developed the methodology. KP and AR developed the software. KP, DL, SK, SD, CL, and KL conducted data collection. KP, AR, and DL conducted data curation. KP, SS, and CT conducted physician analysis. KP conducted data analysis and data visualisation. KP drafted the initial manuscript. KP, CT, and VC reviewed the results, interpreted findings, and edited the manuscript. SS translated the abstract. CT and the Angkor Hospital for Children fundraising team acquired funding. KP and DL managed and coordinated the project. CT and VC provided supervision. All authors reviewed and approved the final version of the manuscript. All authors had full access to the data and had final responsibility for the decision to submit the manuscript for publication.
Data sharing statement
The datasets generated and/or analysed during the current study are not publicly available due to ethical and legal reasons, including participant anonymity and privacy, but may be available from the corresponding author on reasonable request. A data access agreement will be put in place prior to data transfer. Instructions and the data application form are available here: https://www.tropmedres.ac/units/moru-bangkok/bioethics-engagement/data-sharing.
Declaration of interests
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1United Nations Inter-agency Group for Child Mortality Estimation (UN IGME)Levels & Trends in Child Mortality: Estimates: Report 2022 [Internet]. New York 2022 Available from:https://childmortality.org/wp-content/uploads/2023/01/UN-IGME-Child-Mortality-Report-2022.pdf
- 2Bhutta Z.A.Das J.K.Bahl R.Can available interventions end preventable deaths in mothers, newborn babies, and stillbirths, and at what cost?Lancet 3849940201434737010.1016/S 0140-6736(14)60792-324853604 · doi ↗ · pubmed ↗
- 3Lawn J.Shibuya K.Stein C.No cry at birth: global estimates of intrapartum stillbirths and intrapartum-related neonatal deaths Bull World Health Organ 836200540941715976891 PMC 2626256 · pubmed ↗
- 4Mathers C.D.Fat D.M.Inoue M.Rao C.Lopez A.D.Counting the dead and what they died from: an assessment of the global status of cause of death data Bull World Health Organ 833200517117715798840 PMC 2624200 · pubmed ↗
- 5Phillips D.E.Abou Zahr C.Lopez A.D.Are well functioning civil registration and vital statistics systems associated with better health outcomes?Lancet 386100012015138613942597122210.1016/S 0140-6736(15)60172-6 · doi ↗ · pubmed ↗
- 6The 17 Goals Sustainable development goals [Internet]Available from:https://sdgs.un.org/goals
- 7Mikkelsen L.Phillips D.E.Abouzahr C.A global assessment of civil registration and vital statistics systems: monitoring data quality and progress Lancet 386100012015139514062597121810.1016/S 0140-6736(15)60171-4 · doi ↗ · pubmed ↗
- 8Setel P.W.Macfarlane S.B.Szreter S.A scandal of invisibility: making everyone count by counting everyone Lancet 37095982007156915771799272710.1016/S 0140-6736(07)61307-5 · doi ↗ · pubmed ↗