Utility of microbial cell-free DNA sequencing in the diagnosis of mycobacterial infections in a quaternary care center
Fernando H. Centeno, Todd Lasco, Ahmed M. Hamdi, Mayar Al Mohajer

TL;DR
This study shows that sequencing microbial cell-free DNA can help diagnose mycobacterial infections and guide treatment in a hospital setting.
Contribution
The study demonstrates the clinical utility of mcfDNA NGS for diagnosing mycobacterial infections in a real-world hospital setting.
Findings
mcfDNA NGS had 75.0% sensitivity and 97.8% specificity for mycobacterial infections.
Positive mcfDNA NGS results led to changes in antimicrobial therapy for most patients.
Abstract
We examine the performance of microbial cell-free DNA (mcfDNA) next-generation sequencing (NGS) testing on patients admitted to a quaternary care hospital in Houston, Texas. The test was 75.0% sensitive and 97.8% specific for all mycobacterial infections. mcfDNA NGS results led to adjustments in antimicrobial therapy for seven of nine patients with positive results.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
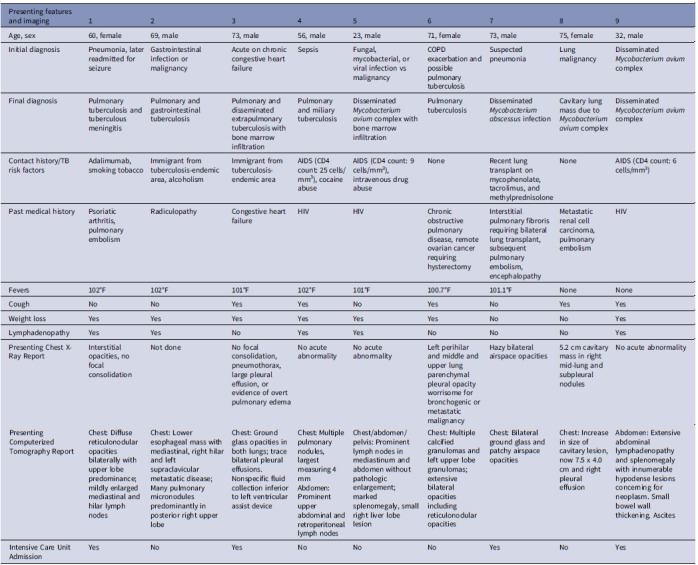 Figure 1
Figure 1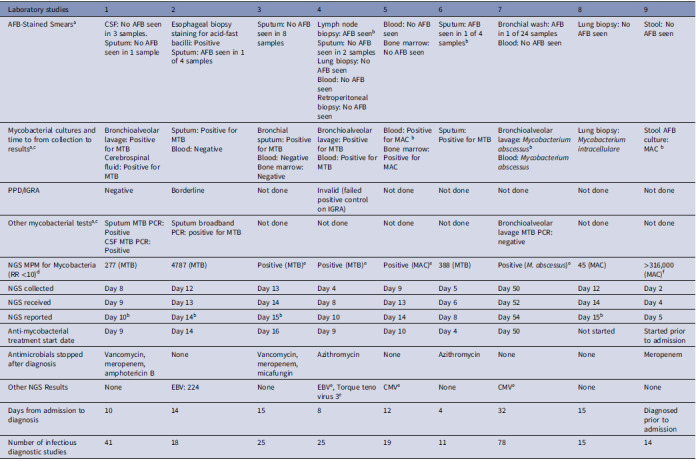 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMycobacterium research and diagnosis · Tuberculosis Research and Epidemiology · Cancer Genomics and Diagnostics
Introduction
Mycobacterial diseases remain a substantial cause of morbidity and mortality in the United States, where the prevalence of tuberculosis (TB) is 4.4–4.8%.^ 1 ^ The prevalence of non-tuberculous mycobacteria remains more infrequent but persists at 11.70 per 100,000.^ 2 ^ Establishing the diagnosis in these cases promptly is challenging and often requires the evaluation of multiple, time-consuming, quality-dependent tests that may not definitively rule out the infection.^ 3 ^
Next-generation sequencing (NGS) of microbial cell-free DNA (mcfDNA) has become increasingly common as an open-ended method for testing against a broad range of pathogens through non-invasive plasma sampling.^ 4 ^ Previous studies of mcfDNA assays have characterized the sensitivity and specificity of the test in TB cases.^ 5 ^ Less clear is the role mcfDNA NGS plays compared to other diagnostic modalities, its performance, and its impact on management. In this retrospective case series, we characterize the mcfDNA role in mycobacterial diagnosis and management in one quaternary medical center.
Methods
The performance of mcfDNA NGS was compared to mycobacterial cultures among patients who had both tests performed between 2017 and 2024. The electronic medical records for patients with positive mcfDNA NGS for mycobacteria were examined for clinical symptoms, radiology, diagnostic tests, and clinical management.
mcfDNA NGS tests were sent to Karius, Inc. (Redwood City, CA), the sputum acid-fast bacilli (AFB) PCR was sent to Quest Diagnostics ® (Secaucus, NJ), while the mycobacterial cultures were performed in-house.
The primary outcome was the sensitivity of the mcfDNA NGS tests compared with mycobacterial cultures. The secondary outcomes included the turnaround time (TAT) and whether mcfDNA NGS led to a change in antimicrobial management. The clinical TAT was defined as the time from physician order and collection to reporting results (days). In contrast, the laboratory TAT was defined as the time from specimen receipt by the laboratory to reporting results. This study was approved by the Baylor College of Medicine Institutional Review Board.
Results
149 patients had both mcfDNA NGS and mycobacterial cultures performed, of which 135 were positive for neither, and 15 were positive for at least one. Five patients with Mycobacterium tuberculosis (MTB) on mcfDNA NGS had confirmatory cultures. Four had non-tuberculous mycobacteria (NTM) on both methods, and three had positive cultures but negative NGS. Three others had positive NGS for NTM but negative AFB cultures, with two deemed false positives and one with a prior history of Mycobacterium avium complex (MAC). Sensitivity and specificity for mcfDNA NGS were 75.0% and 97.8%; for MTB, both were 100%, while NTM sensitivity was 57.1% and specificity 97.8%.
Nine patients with positive mcfDNA NGS and microbiologic data were reviewed: five for MTB and four for NTM. The median age was 69 years, with six males and three females. Seven had risk factors for mycobacterial infection, including two from endemic regions, one on adalimumab, a lung transplant recipient, and three with AIDS (CD4 < 50). Chronic fever and weight loss were common, with lymphadenopathy seen in three MTB and two MAC cases.
On average, each patient received 27 diagnostic studies for infectious diseases (range 14–78) before diagnosis (Table 2). All patients except one had pending tests for mycobacterial disease at the time mcfDNA NGS was sent, one already had a positive culture for Mycobacterium abscessus, and one had a previously diagnosed MAC infection.
Table 2.Imaging and laboratory studies for study patientsLaboratory studies123456789AFB-Stained Smears^ a ^ CSF: No AFB seen in 3 samples.Sputum: No AFB seen in 1 sampleEsophageal biopsy staining for acid-fast bacilli: PositiveSputum: AFB seen in 1 of 4 samplesSputum: No AFB seen in 8 samplesLymph node biopsy: AFB seen^ b ^ Sputum: No AFB seen in 2 samplesLung biopsy: No AFB seenBlood: No AFB seenRetroperitoneal biopsy: No AFB seenBlood: No AFB seenBone marrow: No AFB seenSputum: AFB seen in 1 of 4 samples^ b ^ Bronchial wash: AFB in 1 of 24 samplesBlood: No AFB seenLung biopsy: No AFB seenStool: No AFB seenMycobacterial cultures and time to from collection to results^a,c^ Bronchioalveolar lavage: Positive for MTBCerebrospinal fluid: Positive for MTBSputum: Positive for MTBBlood: NegativeBronchial sputum: Positive for MTBBlood: NegativeBone marrow: NegativeBronchioalveolar lavage: Positive for MTBBlood: Positive for MTBBlood: Positive for MAC ^ b ^ Bone marrow: Positive for MACSputum: Positive for MTBBronchioalveolar lavage: Mycobacterium abscessus ^ b ^ Blood: Mycobacterium abscessus Lung biopsy: Mycobacterium intracellulare Stool AFB culture: MAC ^ b ^ PPD/IGRANegativeBorderlineNot doneInvalid (failed positive control on IGRA)Not doneNot doneNot doneNot doneNot doneOther mycobacterial tests^a,c^ Sputum MTB PCR: PositiveCSF MTB PCR: PositiveSputum broadband PCR: positive for MTBNot doneNot doneNot doneNot doneBronchioalveolar lavage MTB PCR: negativeNot doneNot doneNGS MPM for Mycobacteria (RR <10)^ d ^ 277 (MTB)4787 (MTB)Positive (MTB)^ e ^ Positive (MTB)^ e ^ Positive (MAC)^ e ^ 388 (MTB)Positive (M. abscessus)^ e ^ 45 (MAC)>316,000 (MAC)^ f ^ NGS collectedDay 8Day 12Day 13Day 4Day 9Day 5Day 50Day 12Day 2NGS receivedDay 9Day 13Day 14Day 8Day 13Day 6Day 52Day 14Day 4NGS reportedDay 10^ b ^ Day 14^ b ^ Day 15^ b ^ Day 10Day 14Day 8Day 54Day 15^ b ^ Day 5Anti-mycobacterial treatment start dateDay 9Day 14Day 16Day 9Day 10Day 4Day 50Not startedStarted prior to admissionAntimicrobials stopped after diagnosisVancomycin, meropenem, amphotericin BNoneVancomycin, meropenem, micafunginAzithromycinNoneAzithromycinNoneNoneMeropenemOther NGS ResultsNoneEBV: 224NoneEBV^ e ^, Torque teno virus 3^ e ^ CMV^ e ^ NoneCMV^ e ^ NoneNoneDays from admission to diagnosis10141581243215Diagnosed prior to admissionNumber of infectious diagnostic studies411825251911781514Abbreviations: CSF, Cerebrospinal fluid; AFB, Acid-fast bacilli; MTB, Mycobacterium tuberculosis; MAC, Mycobacterium avium complex; PPD, Purified Protein Derivative; IGRA, Interferon Gamma Release Assay; NGS, Next-generation sequencing; MPM, Molecules per microliter; RR, Reference range; EBV, Epstein-Barr virus; CMV, Cytomegalovirus. a Dates are reported from day of hospital admission. Dates in which tests were received are reported for send-out studies. b First positive mycobacterial diagnostic result received for a patient. c Patients received multiple cultures and repeat PCR tests after the ones included in the table, as reflected in the counts of laboratory studies. For conciseness, only the first set are shown in this table. d In a 684 healthy subject cohort used in the Karius test validation process, the 97^th^ percentile of both Mycobacterium tuberculosis and Mycobacterium avium complex mcfDNA concentration was 10 MPM (Blauwkamp et al., 2019) e Some patients seen in 2017 received an earlier version of mcfDNA NGS studies that did not quantify the MPM of mcfDNA. Instead, the samples were tested with a negative buffer control. f Concentration above quantifiable range for the assay.
The median clinical TAT for mcfDNA NGS was 3.3 days (range 2–6), while the median laboratory TAT was one day (range 1–2). Mycobacterial cultures had a median clinical and laboratory TAT of 27 days (range 9–46). Three acid-fast stains were positive: a lymph node biopsy and two sputum specimens with a median clinical and laboratory TAT of one day. Two patients had a positive sputum MTB PCR with a clinical TAT of nine days for both and a median laboratory TAT of 4.5 days (range 2–7).
The median time from admission to diagnosis was 11 days (range 4–15). In four patients, NGS results were the first to be positive. In three, alternative testing resulted in positive for MAC and TB before NGS results were received. The diagnosis was already established in two when mcfDNA NGS testing was sent.
Anti-mycobacterial therapy was started empirically in three patients: two with tuberculosis and one with NTM. One was already receiving therapy for a prior MAC diagnosis. In two, anti-mycobacterial therapy was started once positive NGS had resulted. In two, treatment was started after positive mycobacterial cultures. One was discharged and lost to follow-up before the start of treatment. Additionally, five patients discontinued empiric antibiotics (vancomycin, meropenem, amphotericin B, micafungin, and azithromycin) once positive NGS results were received. Four of nine patients required intensive care unit admissions and intubation. One patient expired, one was discharged to hospice care, and another to a skilled nursing facility, while the rest were discharged home.
Discussion
Our results showed that when clinical suspicion is high, mcfDNA NGS testing can be an additional and valuable tool to achieve an accurate and timely diagnosis. Despite being a send-out test collected after other mycobacterial studies, mcfDNA NGS testing established the diagnosis before other laboratory studies in four out of nine patients. It also led to changing clinical management in patients due to earlier initiation of antimycobacterial treatment and discontinuation of other antimicrobials.
There were significant issues encountered by clinicians when using traditional tests, including the time required for laboratory diagnosis using conventional mycobacterial culture and send-out TB PCRs and the limited sensitivity of acid-fast smears. NGS of mcfDNA allowed clinicians to discontinue unnecessary antibiotics in some patients and start anti-mycobacterial therapy in others. The observed performance of the test was greater for MTB than seen in a prior study, ^ 5 ^ but it was markedly less for NTM than MTB. Notably, the delay in ordering the mcfDNA NGS compared to traditional tests could have negatively impacted its performance.
The test results must be carefully correlated with clinical presentation, as it can detect low concentrations of organisms like MAC that may colonize airways without causing disease. Additionally, mcfDNA NGS remains costly at 231 for MTB PCR and $4,325 for daily ICU charges. Until costs decrease, this test should be reserved for cases where diagnostic delays may lead to clinical deterioration and increased spending.
The greatest benefit of mcfDNA NGS was observed when traditional tests were done alongside NGS to maximize microbial identification and expedite results or when the disease presentation was nonspecific and broad antimicrobial therapies were used. Patients where mcfDNA NGS did not change outcomes were often immunocompromised, with the disseminated disease diagnosed by sampling sputum, blood, or stool. A prior study showed no clinical benefit in over nine of ten tests. Clinicians should carefully assess available diagnostics and their potential impact on outcomes.^ 7 ^
While this series does not definitively answer how diagnostic approaches for such complex presentations should be adjusted, it does illustrate the necessity for further investigation to best utilize this open-ended diagnostic tool in such challenging encounters. Our study is limited by the small number of patients included. Also, the TAT of different laboratory tests varies by the institution and microbiology laboratory capacity, affecting the generalizability of our findings.
Table 1.Clinical characteristics of study patientsPresenting features and imaging123456789Age, sex60, female69, male73, male56, male23, male71, female73, male75, female32, maleInitial diagnosisPneumonia, later readmitted for seizureGastrointestinal infection or malignancyAcute on chronic congestive heart failureSepsisFungal, mycobacterial, or viral infection vs malignancyCOPD exacerbation and possible pulmonary tuberculosisSuspected pneumoniaLung malignancyDisseminated Mycobacterium avium complexFinal diagnosisPulmonary tuberculosis and tuberculous meningitisPulmonary and gastrointestinal tuberculosisPulmonary and disseminated extrapulmonary tuberculosis with bone marrow infiltrationPulmonary and miliary tuberculosisDisseminated Mycobacterium avium complex with bone marrow infiltrationPulmonary tuberculosisDisseminated Mycobacterium abscessus infectionCavitary lung mass due to Mycobacterium avium complexDisseminated Mycobacterium avium complexContact history/TB risk factorsAdalimumab, smoking tobaccoImmigrant from tuberculosis-endemic area, alcoholismImmigrant from tuberculosis-endemic areaAIDS (CD4 count: 25 cells/mm^3^), cocaine abuseAIDS (CD4 count: 9 cells/mm^3^), intravenous drug abuseNoneRecent lung transplant on mycophenolate, tacrolimus, and methylprednisoloneNoneAIDS (CD4 count: 6 cells/mm^3^)Past medical historyPsoriatic arthritis, pulmonary embolismRadiculopathyCongestive heart failureHIVHIVChronic obstructive pulmonary disease, remote ovarian cancer requiring hysterectomyInterstitial pulmonary fibroris requiring bilateral lung transplant, subsequent pulmonary embolism, encephalopathyMetastatic renal cell carcinoma, pulmonary embolismHIVFevers102°F102°F101°F102°F101°F100.7°F101.1°FNoneNoneCoughNoNoYesYesNoYesNoYesYesWeight lossYesYesYesYesYesYesNoNoYesLymphadenopathyYesYesNoYesYesNoNoNoYesPresenting Chest X-Ray ReportInterstitial opacities, no focal consolidationNot doneNo focal consolidation, pneumothorax, large pleural effusion, or evidence of overt pulmonary edemaNo acute abnormalityNo acute abnormalityLeft perihilar and middle and upper lung parenchymal pleural opacity worrisome for bronchogenic or metastatic malignancyHazy bilateral airspace opacities5.2 cm cavitary mass in right mid-lung and subpleural nodulesNo acute abnormalityPresenting Computerized Tomography ReportChest: Diffuse reticulonodular opacities bilaterally with upper lobe predominance; mildly enlarged mediastinal and hilar lymph nodesChest: Lower esophageal mass with mediastinal, right hilar and left supraclavicular metastatic disease; Many pulmonary micronodules predominantly in posterior right upper lobeChest: Ground glass opacities in both lungs; trace bilateral pleural effusions. Nonspecific fluid collection inferior to left ventricular assist deviceChest: Multiple pulmonary nodules, largest measuring 4 mmAbdomen: Prominent upper abdominal and retroperitoneal lymph nodesChest/abdomen/pelvis: Prominent lymph nodes in mediastinum and abdomen without pathologic enlargement; marked splenomegaly, small right liver lobe lesionChest: Multiple calcified granulomas and left upper lobe granulomas; extensive bilateral opacities including reticulonodular opacitiesChest: Bilateral ground glass and patchy airspace opacitiesChest: Increase in size of cavitary lesion, now 7.5 x 4.0 cm and right pleural effusionAbdomen: Extensive abdominal lymphadenopathy and splenomegaly with innumerable hypodense lesions concerning for neoplasm. Small bowel wall thickening. AscitesIntensive Care Unit AdmissionYesNoYesNoNoNoYesNoYes Abbreviations: TB, Tuberculosis; AIDS, Acquired immunodeficiency syndrome; CD4, Cluster of differentiation 4; HIV, Human immunodeficiency virus.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mancuso J. D , Diffenderfer J. M , Ghassemieh B. J , Horne D. J , Kao T. C . The prevalence of latent tuberculosis infection in the United States. Am J Respir Crit Care Med 2016; 194(4):501–509. 10.1164/rccm.201508-1683 OC.26866439 PMC 12057332 · doi ↗ · pubmed ↗
- 2Winthrop K. L , Marras T. K , Adjemian J , Zhang H , Wang P , Zhang Q. Incidence and prevalence of nontuberculous mycobacterial lung disease in a large U.S. Managed care health plan, 2008–2015. Ann Am Thorac Soc 2020;17:178–185. 10.1513/Annals ATS.201804-236OC.31830805 PMC 6993793 · doi ↗ · pubmed ↗
- 3Datta S , Shah L , Gilman R. H , Evans C. A. Comparison of sputum collection methods for tuberculosis diagnosis: a systematic review and pairwise and network meta-analysis. Lancet Glob Health 2017;5):e 760–e 771. 10.1016/S 2214-109X(17)30201-2.28625793 PMC 5567202 · doi ↗ · pubmed ↗
- 4Blauwkamp T. A , Thair S , Rosen M. J et al. Analytical and clinical validation of a microbial cell-free DNA sequencing test for infectious disease. Nat Microbiol 2019;4:663 -674. 10.1038/s 41564-018-0349-6.30742071 · doi ↗ · pubmed ↗
- 5Yu G , Shen Y , Ye B , Shi Y. Diagnostic accuracy of Mycobacterium tuberculosis cell-free DNA for tuberculosis: a systematic review and meta-analysis. PLOS ONE 2021;16:e 0253658. 10.1371/journal.pone.0253658.34161399 PMC 8221493 · doi ↗ · pubmed ↗
- 6Zhou Y , Hemmige V , Dalai S. C , Hong D. K , Muldrew K , Mohajer M. A. Utility of whole-genome next-generation sequencing of plasma in identifying opportunistic infections in HIV/AIDS. Open AIDS J 2019;13:7–11. 10.2174/1874613601913010007. · doi ↗
- 7Hogan C.A , Yang S , Garner O.B et al. Clinical impact of metagenomic next-generation sequencing of plasma cell-free DNA for the diagnosis of infectious diseases: a multicenter retrospective cohort study. Clin Infect Dis 2021; 72:239–245. 10.1093/cid/ciaa 035.31942944 · doi ↗ · pubmed ↗