A Hidden Danger Behind the Self-Reported Intrauterine Pregnancy
Kenichiro Iga, Tomoyuki Shirahige, Shinji Yamada, Sunao Yamauchi

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1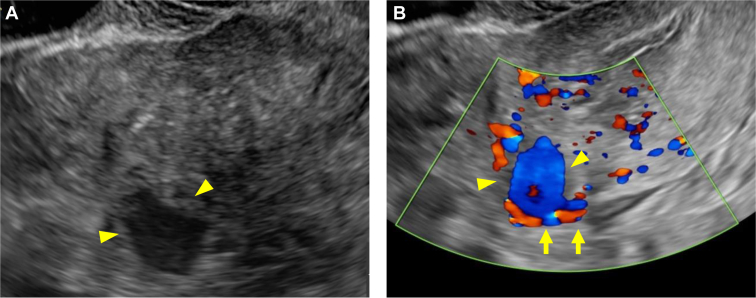 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEctopic Pregnancy Diagnosis and Management · Gestational Trophoblastic Disease Studies · Reproductive Health and Contraception
Patient Presentation
1
A 32-year-old woman, gravida 3 para 0, at 5 weeks of gestation, presented to the emergency department with sudden onset of abdominal pain. She reported that she had an intrauterine pregnancy confirmed by her obstetrician. For this pregnancy, she had undergone in vitro fertilization and frozen embryo transfer with 2 embryos. She had a history of ectopic pregnancy and a left salpingectomy. On arrival, her vital signs were as follows: blood pressure, 89/61 mm Hg; heart rate, 102 beats per minute; and oxygen saturation, 100% without oxygen supplementation. Physical examination revealed pallor and right lower abdominal tenderness. Blood tests revealed a hemoglobin level of 8.3 g/dL. The serum β human chorionic gonadotropin level was 18,068.7 mIU/mL. Transabdominal ultrasonography showed significant free fluid extending from the liver surface to the pouch of Douglas. Transvaginal ultrasonography revealed a 12.1-mm gestational sac in the uterus and an 18.6-mm cystic mass in the left uterine cornu with internal blood flow suggestive of hemorrhage (Figs 1 and 2). She was considered to be in hypovolemic shock due to hemorrhage, and 4 units of red blood cells and 4 units of fresh frozen plasma were urgently transfused.Figure 1. Transvaginal ultrasonography: a 12.1-mm gestational sac in the uterus.Figure 2. Transvaginal ultrasonography: (A) An 18.6-mm cystic mass (arrowheads) in the left uterine cornu; (B) A mass (arrowheads) with internal blood flow suggestive of hemorrhage (arrows) in the left uterine cornu.
Diagnosis: Heterotopic Pregnancy
2
Heterotopic pregnancy has been reported to occur with a frequency of 1 in 30,000 pregnancies.1 However, in pregnancies resulting from assisted reproductive technology, the incidence is estimated to increase significantly, occurring in 0.7% to 1% of cases.2^,^3 Furthermore, in cases of multiple embryo transfer, the frequency increases in proportion to the number of embryos transferred.4 The presence of an intrauterine pregnancy does not exclude the possibility of a concurrent ectopic pregnancy, which can lead to misdiagnosis as a threatened miscarriage. One study found that approximately 6% of heterotopic pregnancies are missed during the initial ultrasound examination.5 A study reported that 15.4% of heterotopic pregnancies developed hypovolemic (hemorrhagic) shock.6 Thus, heterotopic pregnancy is a condition that can be missed and could be life-threatening, emphasizing the critical importance of timely diagnosis and intervention.
In our case, emergency laparoscopic surgery was performed and examination revealed swelling in the left uterine cornu, indicative of a possible interstitial pregnancy. Subsequently, a left cornual resection was performed. This case highlights the importance of considering heterotopic pregnancies in at-risk patients presenting with abdominal pain in early pregnancy, even when an intrauterine pregnancy is confirmed, as delayed diagnosis can lead to life-threatening complications such as hypovolemic (hemorrhagic) shock.
Funding and Support
By JACEP Open policy, all authors are required to disclose any and all commercial, financial, and other relationships in any way related to the subject of this article as per ICMJE conflict of interest guidelines (see www.icmje.org). The authors have stated that no such relationships exist.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tal J.Haddad S.Gordon N.Heterotopic pregnancy after ovulation induction and assisted reproductive technologies: a literature review from 1971 to 1993 Fertil Steril 6611996112875260210.1016/s 0015-0282(16)58378-2 · doi ↗ · pubmed ↗
- 2Clayton H.B.Schieve L.A.Peterson H.B.Ectopic pregnancy risk with assisted reproductive technology procedures Obstet Gynecol 107320065956041650793010.1097/01.AOG.0000196503.78126.62 · doi ↗ · pubmed ↗
- 3American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins—Gynecology ACOG Practice Bulletin No. 193: tubal ectopic pregnancy Obstet Gynecol 13132018 e 91e 1032947034310.1097/AOG.0000000000002560 · doi ↗ · pubmed ↗
- 4Kirk E.Bottomley C.Bouene T.Diagnosing ectopic pregnancy and current concepts in the management of pregnancy of unknown location Hum Reprod Update 20220142502612410160410.1093/humupd/dmt 047 · doi ↗ · pubmed ↗
- 5Xiao J.Zhou X.Wang S.Ultrasound manifestations and clinical analysis of 50 cases of heterotopic pregnancy J Clin Ultrasound 525202449149810.1002/jcu.2366038437597 · doi ↗ · pubmed ↗
- 6Ge F.Ding W.Zhao K.Qu P.Management of heterotopic pregnancy: clinical analysis of sixty-five cases from a single institution Front Med (Lausanne)102023116644610.3389/fmed.2023.1166446 PMC 1020622037234242 · doi ↗ · pubmed ↗