Anterolateral Thigh Flap Repair of Ruptured Incisional Hernia with Intractable Ascites after Laparoscopic Liver Resection: A Case Report
Tomohiro Yoshimura, Shinya Hayami, Atsushi Miyamoto, Kensuke Nakamura, Satsuki Tachibana, Atsushi Shimizu, Yuji Kitahata, Masatoshi Sato, Kyohei Matsumoto, Shinichi Asamura, Manabu Kawai

TL;DR
A 78-year-old man with intractable ascites after liver surgery developed a ruptured hernia, which was successfully repaired using an anterolateral thigh flap without artificial materials.
Contribution
The paper presents a novel hernia repair method using an ALT flap in patients with intractable ascites.
Findings
ALT flap repair was effective for ruptured incisional hernia caused by intractable ascites.
The procedure avoided the risk of peritonitis from using artificial prostheses.
The patient experienced significant symptom improvement and no postoperative complications.
Abstract
Incisional hernia is one of the postoperative complications after abdominal surgery including laparoscopic liver resection. There is often intractable ascites after liver resection, especially for patients with severe cirrhosis. In the present study, we report the case of ruptured incisional hernia due to the pressure from massive ascites, which was successfully repaired using an anterolateral thigh (ALT) flap. A 78-year-old man had hepatocellular carcinoma and underwent laparoscopic left lateral sectionectomy. There was no short-term postoperative complication during hospital stay and at discharge, but approximately 5 months postoperatively, massive ascites gradually accumulated that was intractable, and resistant to diuretic drugs. There was eventually rupture of incisional hernia at the umbilical port scar, caused by strong compression from this ascites. One year postoperatively,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
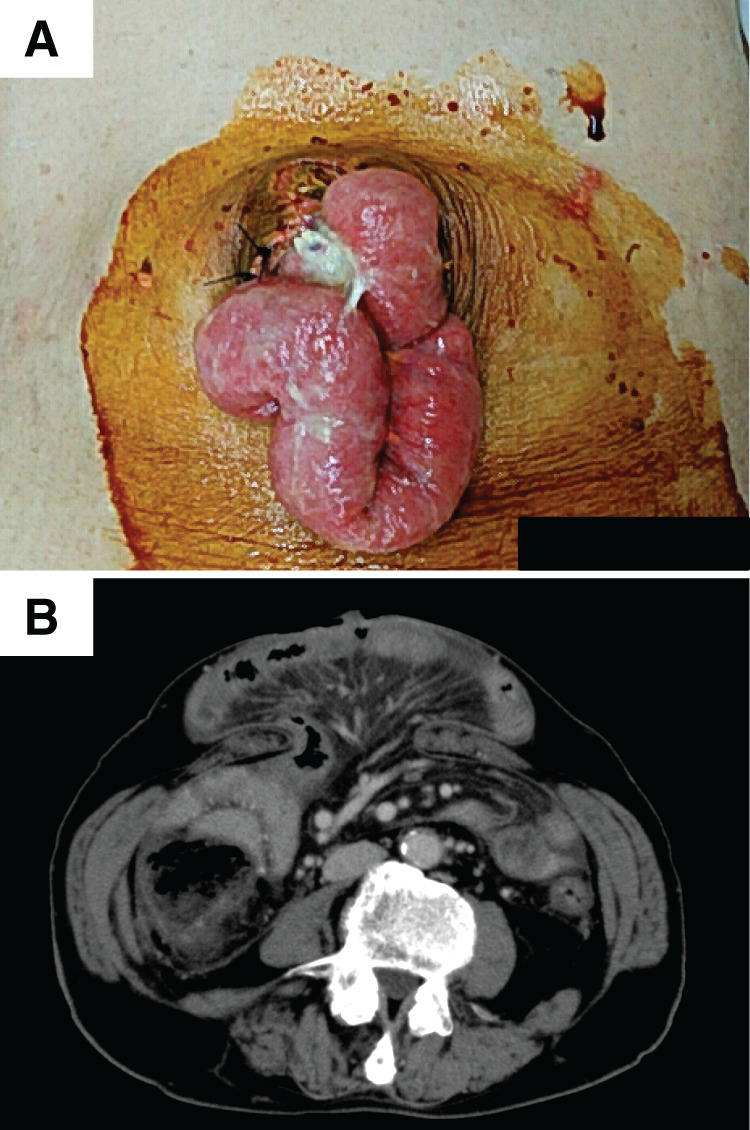 Fig. 1
Fig. 1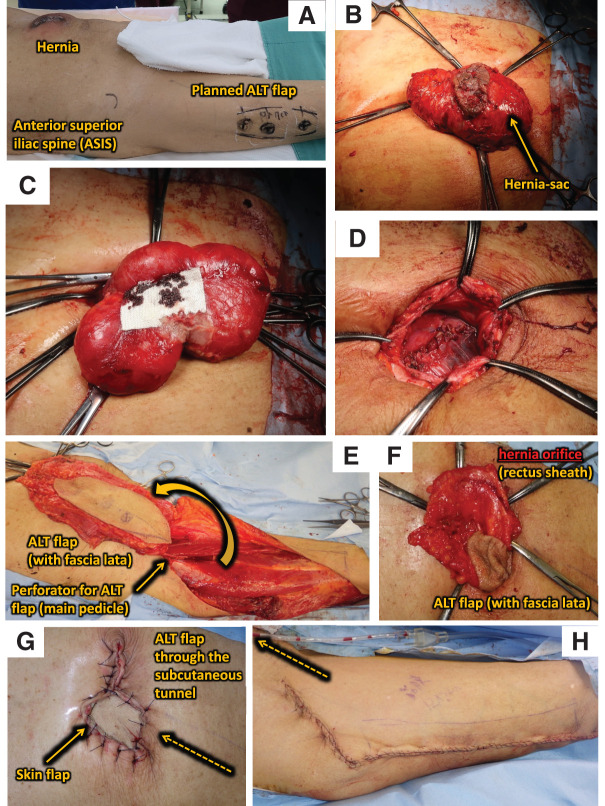 Fig. 2
Fig. 2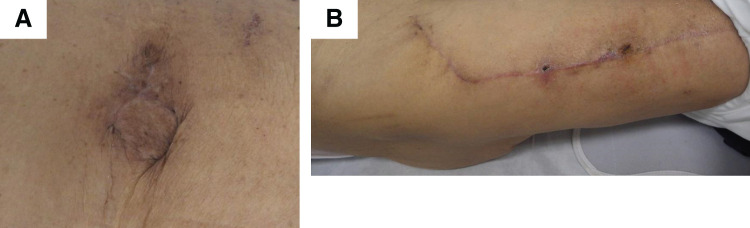 Fig. 3
Fig. 3| Definition | Evaluation | |
|---|---|---|
| Preoperative variables | ||
| Age | Years since birth | 79 |
| Sex | M; F | M |
| BMI | Weight (kg)/height2 (m2) | 20.7 |
| COPD | Diagnosis of COPD | No |
| Smoker | EuraHS6 (never smoker, ex-smoker > 12 months; occasional smoker; daily smoker) | Ex-smoker >12 months |
| Diabetes (types 1 or 2) | Diagnosis of type 1 or 2 diabetes | Type 2 diabetes |
| Immunosuppression/steroids | Diagnosis requiring immunosuppression or chemotherapy | No |
| ASA fitness grade | ASA fitness grade | 2 |
| Hernia variables | ||
| Hernia width | Maximum defect width; EHS classification | 6 cm |
| Loss of domain | Volumetric measurement: Sabbagh method | Not calculated |
| European Hernia Score | EHS classification; incisional hernia | M3W2 |
| No. of hernia defects | No. of defects in anterior abdominal wall | 1 |
| Divarification | Separation >2 cm between rectus muscles | No |
| Reducibility | Reducible; irreducible, no skin changes; irreducible, with skin changes; irreducible, causing bowel obstruction | Irreducible, with skin changes |
| Previous abdominal operations | No. of midline, subcostal, and transverse incisions | Single umbilical incision and five trocar sites incisions in the upper abdomen |
| No. of previous hernia repairs ± mesh | No. of previous hernia repairs and mesh | No |
| Previous wound infection (SSI) | Previous SSI at site of hernia repair | No |
| Hernia defect area | Defect area where hernia sac passes through abdominal wall | 23.5 cm2 |
| Stoma present | Abdominal wall ostomy present | No |
| Previous component separation | Previous anterior component/transversus abdominis release | No |
| Current mesh infection | Chronic infection, sinus or abscess at location of mesh | No |
| Perioperative variables | ||
| Mode of surgery | Mode of surgery (laparoscopic; open; robotic) | Open |
| Mesh or suture | Method of repair | Flap reconstruction |
| Ventral Hernia Working Group assessment | Low risk; comorbid; contaminated; dirty | Comorbid |
| CDC assessment | Clean; clean-contaminated; contaminated; dirty | Clean-contaminated |
| Preoperative botulinum toxin | Preoperative injection of botulinum toxin to strap muscles | No |
| Component separation | Anterior component/transversus abdominis release | No |
| Concomitant gastrointestinal procedure | Bowel resection; cholecystectomy; stoma formation | No |
| Mesh repair | Evaluation about flap reconstruction | |
| Exact mesh name | Trade name and flap type | Anterolateral thigh flap |
| Flap fixation technique | Sutures or tacks (absorbable; non-absorbable) | Sutures (absorbable) |
| Position of mesh | ICAP nomenclature | N/A |
| Mesh size | Intraoperative measurement | The size of skin flap and fascia lata were planned as 7 × 22 and 12 × 22 cm. |
| Bridging versus fascial closure | EHS definitions. Anterior fascia completely closed or not completely closed | N/A |
| Mesh overlap | Mesh overlap area/defect area ratio. Ellipse: Overlap = πAB − πab | N/A |
| Suture repair | ||
| Suture type | Absorbable or non-absorbable material used | Absorbable material used |
| Postoperative outcomes | ||
| SSI | CDC definition of SSI: a) Superficial; b) deep; c) organ space | No |
| SSO | Any adverse wound event. SSI, seroma, hematoma, fistula, etc. | No |
| SSO requiring intervention | SSOs requiring procedural intervention | No |
| Mesh infection | Chronic infection, sinus or abscess at location of mesh | No |
| Chronic pain | Pain lasting longer than 3 months after surgery | No |
| Hernia recurrence | EHS definition: a protrusion of the contents of the abdominal cavity or preperitoneal fat through a defect in the abdominal wall at the site of a previous repair of an abdominal wall hernia | No |
| Clavien–Dindo grade | Grades I–V. Grade IIIb: intervention under general anesthesia | No |
| 30-day reoperation rate | Abdominal operation under general or regional anesthesia within 30 days of primary ventral hernia repair | No |
| Value | (Unit) | Value | (Unit) |
|---|---|---|---|
| WBC | 54.6 (102/μL) | Alb | 2.3 (g/dL) |
| RBC | 352 (104/μL) | AST | 25 (IU/L) |
| Hb | 11.5 (g/dL) | ALT | 19 (IU/L) |
| Ht | 34.2 (%) | ALP | 206 (IU/L) |
| PLT | 16.5 (104/μL) | T-bil | 0.7 (mg/dL) |
| Neu | 77.9 (%) | D-bil | 0.2 (mg/dL) |
| Ly | 12.5 (%) | Cre | 1.02 (mg/dL) |
| CRP | 14.79 (mg/mL) | eGFR | 54.2 |
| AFP | 1.6 (ng/mL) | BUN | 25.3 (mg/dL) |
| AFP-L3% | Undetectable (%) | Na | 137 (mEq/L) |
| PIVKA-II | 16 (mAU/mL) | K | 4.5 (mEq/L) |
| HA | 100 (ng/mL) | PT (ratio) | 86.0 (%) |
| HbA1c | 6.4 (%) | PT-INR | 1.10 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHernia repair and management · Abdominal Surgery and Complications · Intestinal and Peritoneal Adhesions
Abbreviations
ALT anterolateral thigh CART cell-free and concentrated ascites reinfusion therapy TFL tensor fascia lata
INTRODUCTION
Laparoscopic liver resection is widely performed for the treatment of hepatocellular carcinoma.^1,2)^ The mortality rate has been decreasing with the improvement of surgical techniques and appropriate perioperative managements in liver resection. However, intractable ascites is sometimes encountered after liver resection, especially in patients with severe cirrhosis.^3,4)^ For refractory ascites following liver resection, treatments such as oral diuretics, branched-chain amino acids, fresh frozen plasma, albumin, and paracentesis followed by CART are considered.^5)^ However, these treatments can cause an increase in medical costs and can prolong hospital stay.^3)^
Incisional hernia is another postoperative complication after abdominal surgery including laparoscopic liver resection. The incidence of umbilical hernias with ascites is reportedly up to 20%.^6)^ A prosthetic mesh is generally used for the treatment of incisional hernia, even in cirrhotic cases.^6,7)^ However, taking into consideration the possibility of intraabdominal infection postoperatively, incisional hernia with ascites is thought to be difficult to treat by prosthetic mesh.^8)^ A definitive treatment strategy for incisional hernia repair with due consideration of the risks of infection has not yet been established. Here, we report a case of ruptured incisional hernia by massive ascites, which was successfully repaired using an ALT flap.
CASE PRESENTATION
Present and past history
A 78-year-old man had hepatocellular carcinoma derived from alcoholic cirrhosis that was detected in the left lateral section during treatment for ruptured esophageal varices. His past history included hypertension, diabetes mellitus, and stroke, and he had received corresponding medical treatment for each respective disease. His background liver function was good enough for the liver surgery (Child-Pugh score 5A), so he underwent laparoscopic left lateral sectionectomy and was discharged on the 16th postoperative day without short-time complications. However, massive ascites gradually accumulated around 5 months postoperatively that was intractable, and resistant to diuretic drugs. Finally, incisional hernia at the umbilical port scar appeared as a result of strong compression by the ascites. One year after the initial surgery, skin breakdown at the umbilicus led to intestinal evisceration (Fig. 1A and 1B). Simple suturing was first attempted several times in the emergency room to close the wound, but the intra-abdominal pressure was so high that the umbilical skin was broken again. We carefully considered operative indications for this situation. Incisional hernia was evaluated according to previous guidelines^9)^ (Table 1). Through the preoperative discussion, we planned incisional hernia repair using an ALT flap in collaboration with plastic surgeons. Liver function was Child-Pugh score 9B; albumin was especially low (Table 2). By using CART, 2000 mL of ascites was preoperatively collected, and albumin products were given at 12.5 g/50 mL per day for 3 days before surgery. Moreover, C-reactive protein was high; therefore, cefazolin was used perioperatively as antibiotic prophylaxis.
(A) Incisional hernia at the umbilical region appeared, caused by the strong compression from ascites. Skin breakdown at the umbilicus led to intestinal evisceration. (B) Abdominal computed tomography showing incisional hernia at the umbilical region.
Surgical procedures
First, as preoperative planning, the locations of an ALT flap and incisional hernia were marked (Fig. 2A). A spindle-shaped skin incision was made and the hernia sac was identified. After careful dissection between the small intestine and the greater omentum for adhesion to the hernia sac without injuring the bowel, we resected the redundant hernia sac (Fig. 2B and 2C). A fascia defect was measured as 5 × 6 cm and the peritoneum was closed by continuous suture using 2-0 Coated Vicryl (Johnson and Johnson, Tokyo, Japan) (Fig. 2D). Then, ALT flap preparation was started by plastic surgeons (Fig. 2E). The size of the skin flap and fascia lata were planned as 7 × 22 and 12 × 22 cm, respectively. Perforators from the descending branch of the lateral femoral circumflex artery were carefully preserved. The ALT flap was rotated around the most cranial perforator. Inguinal skin was not incised and a subcutaneous tunnel was made. The ALT flap was elevated through the inguinal subcutaneous tunnel after de-epithelialization (Fig. 2E–2H) and fixed by interrupted suture using 1-0 PDS plus (Johnson and Johnson) with rectus abdominis fascia and 2-0 nylon with skin. Subcutaneous closed suction drain (SB drain 5 mm; SB-KAWASUMI LABORATORIES, Kanagawa, Japan) was inserted at both the reconstruction and flap donor sites. Operation time was 265 min and the amount of intraoperative bleeding was 15 mL.
Surgical procedures. (A) Preoperative planning. (B) Resection of the hernia-sac. (C) After resection of the hernia-sac, the small intestine is returned to the abdominal cavity. (D) Peritoneal closure and identification of hernia orifice. (E) ALT flap planning. (F) Elevation of an ALT flap through inguinal subcutaneous tunnel. (G) Completed picture (abdomen). (H) Completed picture (leg).
Postoperative management
After the operation, the patient felt his hernia symptoms had dramatically improved. He was given albumin 12.5 g/50 mL/day also for 3 days after the surgery and discharged on postoperative day 16 without any complications. Ascites disappeared by use of diuretic drugs and 3 rounds of CART. The wound was in good condition at 3 months after surgery (Fig. 3A and 3B) and 36 months later there has been no recurrence of incisional hernia since the hernia repair surgery.
Wound 3 months after this surgery. (A) abdomen. (B) right leg.
DISCUSSION
We successfully performed hernia repair using an ALT flap and without artificial materials for ruptured incisional hernia caused by intractable ascites. For this patient, it was necessary to treat the conflicting conditions, both incisional hernia and massive intractable ascites, simultaneously or sequentially. However, these 2 conditions required somewhat contradictory treatment because hernia repair surgery can only be performed after management of ascites and because using artificial prostheses risks infecting the ascites and possibly leading to peritonitis.
Incisional hernia is one of the potential postoperative complications after abdominal surgery including laparoscopic liver resection. Ascites is another potential postoperative complication after liver resection, with frequency reported at about 25.5%.^10)^ Intractable ascites is sometimes seen, especially in patients with more severe liver cirrhosis, and massive ascites with incisional hernia might result in abdominal wall rupture due to excessive compression.^11)^ Hernia repair must remain tension-free,^12)^ and inadequate control of ascites may lead to recurrence due to increased intra-abdominal pressure, as observed in this case. To keep the wound tension-free, prosthetic mesh is generally used for the treatment of incisional hernia,^13)^ however, mesh infection after abdominal wall hernia repair is a life-threating complication.^14)^ Hernia mesh repair with liver cirrhosis and ascites has been reported as a safe approach with a low risk of infection;^11,13)^ on the other hand, there is also a report about abdominal wall repair without mesh in conditions of suspected infection.^15)^ The use of artificial products is therefore controversial, and incisional hernia with ascites may be difficult to treat by prosthetic mesh. Hernia repair using artificial prosthesis has a risk of infection with ascites and may lead to peritonitis. Adaptation of the Denver shunt was also considered for ascites control, but hernia repair may be difficult because Denver shunt should be avoided in conditions of suspected infection by ruptured incisional hernia.^16)^
Previously, we used a pedicled TFL flap for reconstruction of an infected recurrent ventral hernia after a mesh repair.^17)^ We therefore decided to consult with plastic surgeons and planned incisional hernia repair using a flap. Due to its muscular component and relatively greater thickness, the TFL flap is less appropriate for small-volume reconstruction. Furthermore, its use is associated with a higher risk of donor site morbidity compared with the ALT flap. Therefore, the ALT flap was selected as the more suitable option in this case. ALT flap, first reported by Song et al. in 1984, is a large flap harvested from the thigh with a long neurovascular pedicle.^18)^ Blood flow of the flap was based on the descending branch of the lateral circumflex femoral artery. ALT flaps are commonly used in abdominal wall reconstruction.^19,20)^ Reconstruction with an ALT flap appears to be useful when abdominal wall reconstruction with an artificial prosthesis is difficult due to infected ascites.
CONCLUSIONS
Intractable ascites is often a problem in patients after liver resection and may be difficult to treat when complicated by abdominal wall incisional hernias. We successfully performed hernia repair using an ALT flap without the use of artificial materials such as mesh for ruptured incisional hernia with intractable ascites.
ACKNOWLEDGMENTS
We acknowledge proofreading and editing by Benjamin Phillis at the Clinical Study Support Center at Wakayama Medical University.
DECLARATIONS
Funding
The authors have no financial support to declare.
Authors’ contributions
Study conception and design: TY, SH
Acquisition of data: TY, SH
Analysis and interpretation of data: TY, SH, KM
Drafting of manuscript: TY, SH
Critical revision: AM, KN, ST, AS, YK, MS, KM, SA, MK
All authors have read and approved the manuscript, and they are responsible for the manuscript.
Availability of data and materials
De-identified patient data that support the findings of this case report are available upon reasonable request from the corresponding author.
Ethics approval and consent to participate
This work does not require ethical considerations or approval. Informed consent to participate in this study was obtained from the patient.
Consent for publication
Informed consent was obtained from the patient for the publication of this case report.
Competing interests
The authors declare that they have no competing interests.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wakabayashi G Cherqui D Geller DA Recommendations for laparoscopic liver resection: a report from the second international consensus conference held in Morioka. Ann Surg 2015; 261: 619–29.25742461 10.1097/SLA.0000000000001184 · doi ↗ · pubmed ↗
- 2Abu Hilal M Aldrighetti L Dagher I The Southampton consensus guidelines for laparoscopic liver surgery: from indication to implementation. Ann Surg 2018; 268: 11–8.29064908 10.1097/SLA.0000000000002524 · doi ↗ · pubmed ↗
- 3Ishizawa T Hasegawa K Kokudo N Risk factors and management of ascites after liver resection to treat hepatocellular carcinoma. Arch Surg 2009; 144: 46–51.19153324 10.1001/archsurg.2008.511 · doi ↗ · pubmed ↗
- 4Morise Z Ciria R Cherqui D Can we expand the indications for laparoscopic liver resection? A systematic review and meta-analysis of laparoscopic liver resection for patients with hepatocellular carcinoma and chronic liver disease. J Hepatobiliary Pancreat Sci 2015; 22: 342–52.25663288 10.1002/jhbp.215 · doi ↗ · pubmed ↗
- 5Daimon S Yasuhara S Saga T Efficacy of extracorporeal ultrafiltration of ascitic fluid as a treatment of refractory ascites. Nephrol Dial Transplant 1998; 13: 2617–23.9794570 10.1093/ndt/13.10.2617 · doi ↗ · pubmed ↗
- 6Guo C Liu Q Wang Y Umbilical hernia repair in cirrhotic patients with ascites: a systemic review of literature. Surg Laparosc Endosc Percutan Tech 2021; 31: 356–62.10.1097/SLE.000000000000089133347087 · doi ↗ · pubmed ↗
- 7Licari L Salamone G Ciolino G The abdominal wall incisional hernia repair in cirrhotic patients. G Chir 2018; 39: 20–3.29549677 10.11138/gchir/2018.39.1.020PMC 5902140 · doi ↗ · pubmed ↗
- 8Belghiti J Durand F. Abdominal wall hernias in the setting of cirrhosis. Semin Liver Dis 1997; 17: 219–26.9308126 10.1055/s-2007-1007199 · doi ↗ · pubmed ↗