Case Report: Improved hearing in a rare, adult IDH2-mutant brainstem astrocytoma successfully treated with radiation and temozolomide
Takuya Okada, Manabu Natsumeda, Hidemoto Fujiwara, Nayuta Higa, Toshiaki Akahane, Yuki Watabe, Kaoru Tomikawa, Kyoka Nishita, Yoshihiro Tsukamoto, Shinsuke Ohshima, Arata Horii, Akihide Tanimoto, Ryosuke Hanaya, Hiroshi Shimizu, Akiyoshi Kakita, Makoto Oishi

TL;DR
An adult with a rare brainstem tumor showed improved hearing after treatment with radiation and temozolomide, highlighting the importance of accurate diagnosis.
Contribution
This case report demonstrates successful treatment and hearing recovery in a rare IDH2-mutant brainstem astrocytoma using TMZ and radiation.
Findings
The patient's hearing improved significantly after treatment with temozolomide and radiation.
2-hydroxyglutarate levels decreased from 3.602 mM to 0.186 mM following treatment.
Non-canonical IDH2 R172S mutation was identified, guiding effective treatment decisions.
Abstract
Brain stem gliomas harboring IDH mutations can be sensitive to temozolomide (TMZ) treatment, unlike their H3K27-altered counterparts, so distinguishing the two is essential. Here, we report an adult brainstem glioma patient whose hearing loss normalized after treatment. He presented with gradual left hearing loss from two years before, and magnetic resonance (MR) images showed a diffuse mass lesion involving the pons to left middle cerebral peduncle, including the vestibular and cochlear nuclei. On MR spectroscopy (MRS), 2-hydroxyglutarate (2HG) was elevated to 3.602 mM, suggesting an IDH-mutant glioma. Subsequently, an open biopsy was performed via the lateral suboccipital approach, and the pathological diagnosis was astrocytoma, IDH-mutant, CNS WHO grade 3. Molecular analysis revealed a non-canonical IDH2 R172S mutation. Left hearing improved from 87.5 dB to 8.3dB by 6-frequency pure…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
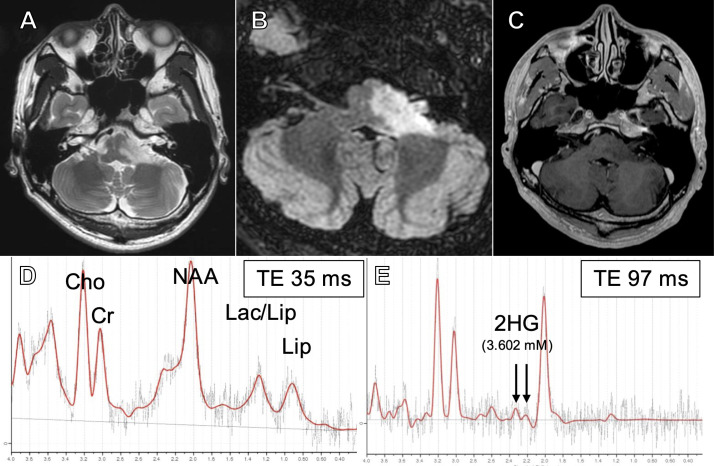 Figure 1
Figure 1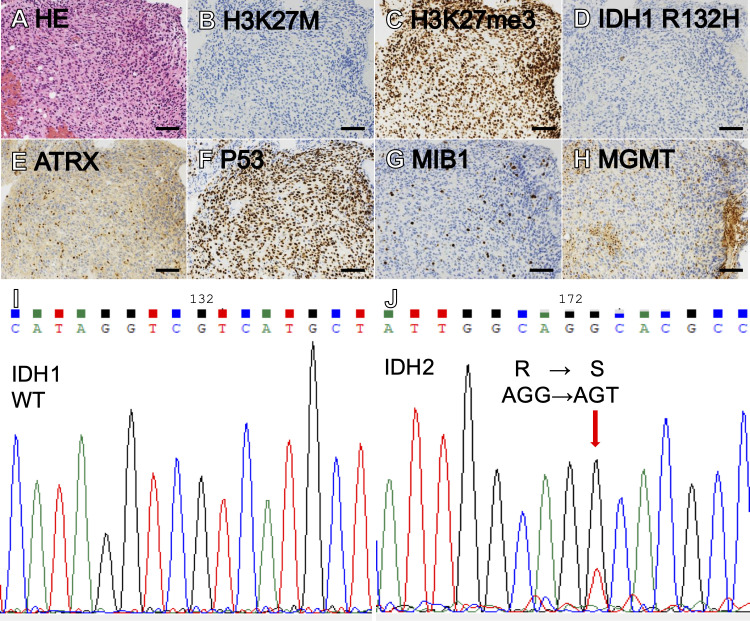 Figure 2
Figure 2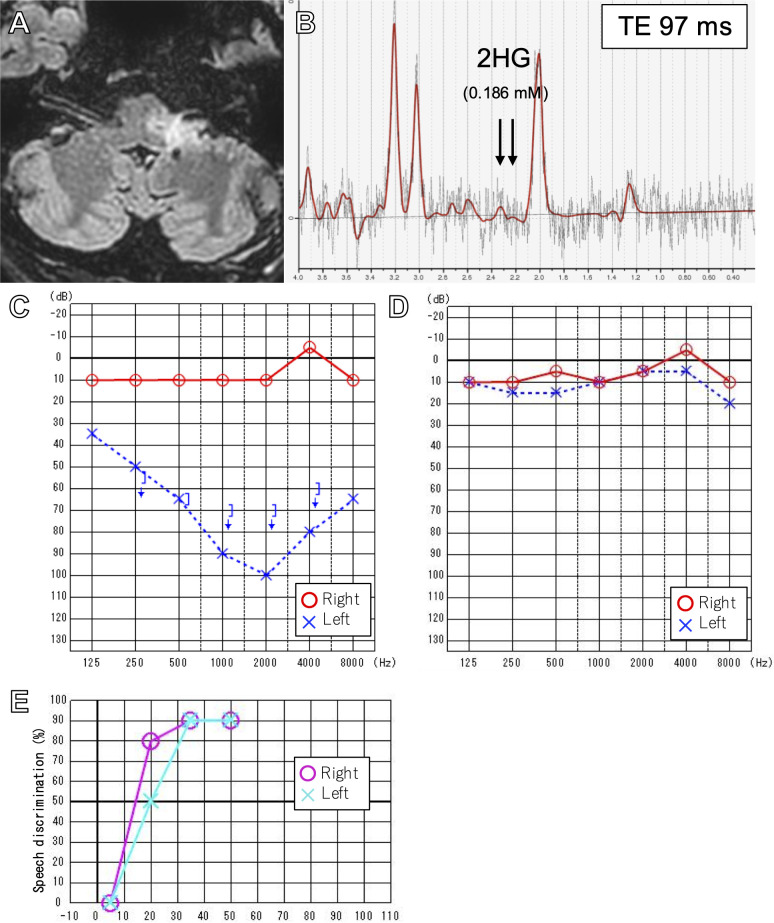 Figure 3
Figure 3- —Japan Society for the Promotion of Science 10.13039/501100001691
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlioma Diagnosis and Treatment · Meningioma and schwannoma management · Brain Metastases and Treatment
Introduction
Adult brainstem gliomas are rare, accounting for less than 2% of all adult gliomas (1). Large-scale studies reporting the genetic profile of adult brainstem gliomas are scarce (2). Their pediatric counterparts, which are known to harbor recurrent alterations of H3F3A K27M (3–5), are now classified along with diffuse gliomas arising from the thalamus (6) and spine (7) as diffuse midline gliomas, H3K27-altered (8). These gliomas almost universally have unmethylated O6-methylguanine-DNA-methyltransferase (MGMT) promoter (9, 10) and generally do not respond to the oral alkylating agent temozolomide (TMZ) (11, 12), with a dismal prognosis (13–17). A couple of studies have shown that mutations in IDH1 and IDH2 genes can be found in 18-31% of adult brainstem gliomas (18–20) and that a majority of these mutations are non-canonical IDH1/2-mutations (21, 22), compared to a high frequency of IDH1 R132H mutations in IDH-mutant supratentorial diffuse gliomas (23, 24). Determining the molecular profile of adult brainstem gliomas is very important clinically because IDH-mutant diffuse gliomas frequently harbor a methylated MGMT promoter and can be expected to respond to TMZ treatment (11, 25).
Here, we present a case of adult brainstem glioma with non-canonical IDH2 mutation and treatment response to radiation and TMZ. Pre-operatively, 2-hydroxyglutarate (2HG) was detected by magnetic resonance spectroscopy (MRS). This rare case report provides rationale that biopsy and genetic testing should be performed in adult brainstem gliomas when feasible to obtain valuable information about treatment response.
Case presentation
A 33-year-old Japanese male with no significant past medical history was referred to Niigata University Medical and Dental Hospital with progressive left hearing loss and tinnitus, which had been worsening for two years. A 6-frequency pure tone audiogram (PTA) was 87.5 dB in the left ear compared to 7.5 dB in the right, and only wave I could be identified on the left auditory brainstem response (ABR) (Supplementary Figure 1A).
Magnetic resonance (MR) images showed a hyperintense lesion extending from the pons to the left middle cerebellar peduncle on T2-weighted and fluid attenuation inverted recovery (FLAIR) images, including the vestibular and cochlear nuclei at the rhomboid fossa (Figures 1A). Post-contrast images showed no enhancement (Figure 1). Magnetic resonance spectroscopy (MRS) showed an increased choline (Cho)-to-creatine (Cr) ratio and decreased N-acetyl aspartate (NAA), suggestive of a malignant brain tumor (Figure 1). In addition, on single voxel MRS with a TE at 97 msec to optimize the detection of 2HG (26), 2HG was detected (3.602 mM at TE =97 msec; S/N =7, Cramer-Rao lower bounds [CRLB] = 32%), suggesting the presence of IDH mutation (Figure 1). 2HG was also detected at a TE of 35 msec (5.692 mM; S/N = 6, CRLB = 42%), although the CRLB was high, suggesting the possible contamination of macromolecules.
T2-weighted (A), fluid-attenuated inversion recovery (FLAIR) (B), and post-contrast (C) magnetic resonance (MR) images at presentation. Short TE (35 msec) single voxel MR spectroscopy (MRS) showing elevated Cho/Cr and decreased NAA (D) and intermediate TE (97 msec) SVMRS showing elevated 2-hydroxyglutarate (E).
A typical DIPG displays more than 50% T2/FLAIR hyperintensity of the ventral pons on MR images (27). In the present case, the tumor progressed to the left middle cerebellar peduncle. Furthermore, considering the results of the MRS and the relatively slow progression of symptoms, the clinicoradiographical presentation was atypical for H3K27-altered DMG of the brainstem. Therefore, we decided that a biopsy was necessary.
We performed a biopsy via the left lateral suboccipital approach, and small pieces of edematous tumor between the root exit zones of the V and VII/VIII complex were sampled. Hematoxylin and eosin (HE) sections showed diffuse astrocytic tumor with nuclear atypia (Figure 2). Immunohistochemically, the tumor cells were negative for H3K27M and positive for H3K27me3 (Figures 2B). Also, IDH1 R132H was negative, but ATRX staining was diminished and P53 was strongly positive, suggestive of an IDH-mutant astrocytoma (Figures 2D). The MIB-1 labeling index was 8% (Figure 2). MGMT was positive in only 5% of tumor cells (Figure 2), below the cutoff of 30% (28), suggesting that the MGMT promoter is methylated. Sanger sequencing (IRB approval #G2022-0012) revealed IDH1 R132 wildtype and IDH2 R172S mutation (Figures 2I). A bimodal DNA and RNA next-generation sequencing panel for integrative diagnosis of glioma (7, 29) was performed (IRB approval #C2023-0039), and IDH2 R172S mutation (variant allele frequency [VAF] 48.1%), as well as TP53 C275F (VAF 91.2%) and ATRX c.3809 + 1G>C (VAF 92.1%), were detected. There was no loss of CDKN2A/B. The integrated diagnosis was astrocytoma, IDH-mutant, CNS WHO grade 3.
Hematoxylin-eosin (HE) staining showed a diffuse, astrocytic tumor with nuclear atypia and moderately increased cellularity (A). The tumor showed negative H3K27M (B), intact H3K27me3 (C), negative IDH1 R132H (D), loss of ATRX (E), and marked staining for P53 (F). MIB labeling index was 8% (G) and MGMT was positive in 5% of tumor cells (H). Sanger sequencing showing IDH1 wildtype (I) and IDH2 R172S (J). (Scale bars = 100 µm).
After the surgery, the patient experienced minimal hypesthesia of the left perioral area. The patient underwent concomitant TMZ and 54 Gy (30 fractions) of intensity-modulated radiation therapy (IMRT), followed by 12 courses of maintenance TMZ. Three months after the completion of treatment, the area of T2/FLAIR hyperintensity on MR images decreased by 51% by volumetric analysis (30) (Figure 3), and 2HG on MRS had drastically decreased to 0.186 mM, suggesting a treatment effect (Figure 3). After finishing TMZ treatment, the patient noticed a partial improvement in his left hearing. His left hearing loss had normalized from 87.5 dB on 6-frequency PTA (Figures 3) to 8.3 dB (Figure 3) and 90% speech discrimination at 35 dB (Figure 3). However, ABR findings remained unchanged, with only wave I identified on the left ABR (Supplementary Figure 1). The patient’s partial improvement of left hearing has persisted, and he is recurrence-free eight months after completion of treatment and 22 months from diagnosis.
FLAIR image after 12 cycles of adjuvant temozolomide (A). Intermediate TE (97msec) SVMRS after treatment showing decreased 2HG (B). Pure tone audiometry before (C) and after treatment (D) showing normalization of left hearing. Speech discrimination after treatment was also normal (E).
Discussion
In the present case, a dramatic response to radiation and temozolomide treatment and subsequent improved hearing were observed in a rare IDH2 R172S-mutant brainstem glioma patient who presented with left hearing loss. Detection of 2HG by MRS served as a less-invasive adjunct to screen for potential IDH mutation, which was confirmed by integrated diagnosis of surgically obtained tissue.
A multicenter review by Shumacher et al. deemed that biopsies are rarely needed to diagnose pediatric brainstem lesions, and MR imaging would suffice in most cases (31). With the introduction of molecular analysis to brain tumor diagnosis, stereotactic and robot-assisted techniques have been implicated in the biopsy of brainstem lesions, however, with the potential for significant morbidity (32).
Up to 90% of pediatric DIPGs are known to harbor H3F3A K27M or HIST1H3B K27M mutations (3–5, 33). Almost all of these H3K27-altered DMGs have unmethylated MGMT promoters (9, 10) and are resistant to TMZ treatment (11, 12, 34). However, a significant percentage of IDH-mutant astrocytomas have been implicated in adult brainstem gliomas, with rates ranging from 18-31% in relatively large series (18–20). It is important to consider that most IDH-mutant astrocytomas arise after the second decade of life (35), likely contributing to the scarcity of IDH-mutant pediatric brainstem gliomas. Almost 70% of IDH-mutant astrocytomas are known to harbor methylated MGMT promoters (23), making them more likely to respond to TMZ treatment (11). In the present case, the diagnosis of IDH mutant astrocytoma was vital in determining treatment with TMZ.
Remarkably, hearing loss dramatically improved after radiation and TMZ treatment. This is especially surprising as hearing loss had been noted for over two years before the presentation. To date, dramatic improvement of cranial nerve signs after treatment has not been extensively reported in gliomas. Visual acuity markedly improved after bevacizumab treatment in 4 cases of pediatric optic pathway gliomas previously treated with chemotherapy or proton-beam radiation (36). Objective hearing improvement was observed in 8 out of 13 (61%) patients with hearing loss in neurofibromatosis type 2-related vestibular schwannomas after receiving bevacizumab (37). We speculate that in the present case, a reduction in compression of the auditory tract by the tumor due to treatment effects led to improved hearing. As seen in both pre- and post-treatment ABR, wave I, which originates from the cochlea, is preserved, suggesting that the cochlear periphery was not affected by the tumor. Different from insults to cochlear peripheries, central auditory pathways may have the potential to recover from injuries via mechanisms such as neural redundancy. Therefore, normal cochlea and reduction of auditory tract compression due to tumor shrinkage could bring about the improvement of hearing on PTA. However, the patient continues to subjectively claim that his left hearing is worse than the right, suggesting that the patient did not attain usable conversational hearing even after the TMZ treatment. Although the post-treatment speech discrimination test seems to be good even in the affected ear, it may be due to the usage of relatively simple syllables in the speech discrimination test in Japan.
In the present case, MRS was performed at presentation, and a high Cho/Cr ratio, decreased NAA, and accumulation of 2HG were noted, suggesting a malignant tumor with possible IDH mutation. We (38, 39) and others (26, 40–42) have succeeded in the detection of 2HG by MRS and also have reported the usefulness of 2HG detection by MRS in non-canonical IDH-mutant gliomas (41, 43). A report by Iwahashi et al. nicely illustrates the diagnosis of non-canonical IDH mutations in brainstem gliomas by MRS (44). 2HG detection by MRS is an important adjunct in diagnosing IDH-mutant brainstem astrocytomas because 72% of infratentorial IDH-mutant gliomas (21) and 59% of IDH-mutant brainstem gliomas (22) have been reported to harbor non-canonical IDH mutations. The IDH2 R172S mutation found in the present case is extremely rare in gliomas. This mutation was not reported in a large series of 170 IDH-mutant gliomas from the US (24) and 286 from Japan (23). Banan et al. report 2 out of 42 (5%) infratentorial and 0 out of 50 (0%) supratentorial IDH-mutant gliomas to be IDH2 R172S-mutant (21).
In addition to the less-invasive detection of 2HG by MRS, surgical biopsy of the lesion and integrated diagnosis of the specimen is strongly recommended when feasible. We have previously reported a specificity of 72.2-81.3% of 2HG accumulation by MRS to detect IDH mutation in gliomas (38, 43). Therefore, false-positive cases can exist. Also, the CRLB of 2HG detection in the present case was 32%, higher than the optimal <20% (26), further necessitating histological confirmation. In the present case, an open biopsy was safely performed, enabling pathological and molecular confirmation.
Conclusion
Marked improvement of hearing was observed after TMZ and radiation treatment in a rare IDH2 R172S-mutant, adult brainstem glioma case. Detection of 2HG by MRS is important for the less-invasive screening of IDH mutation, but a surgical biopsy is strongly recommended when feasible to determine the proper treatment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Reyes-Botero G Mokhtari K Martin-Duverneuil N Delattre JY Laigle-Donadey F. Adult brainstem gliomas. Oncologist. (2012) 17:388–97. doi: 10.1634/theoncologist.2011-0335, PMID: 22382458 PMC 3316925 · doi ↗ · pubmed ↗
- 2Eisele SC Reardon DA. Adult brainstem gliomas. Cancer. (2016) 122:2799–809. doi: 10.1002/cncr.29920, PMID: 27327773 · doi ↗ · pubmed ↗
- 3Wu G Diaz AK Paugh BS Rankin SL Ju B Li Y. The genomic landscape of diffuse intrinsic pontine glioma and pediatric non-brainstem high-grade glioma. Nat Genet. (2014) 46:444–50. doi: 10.1038/ng.2938, PMID: 24705251 PMC 4056452 · doi ↗ · pubmed ↗
- 4Khuong-Quang DA Buczkowicz P Rakopoulos P Liu XY Fontebasso AM Bouffet E. K 27M mutation in histone H 3.3 defines clinically and biologically distinct subgroups of pediatric diffuse intrinsic pontine gliomas. Acta Neuropathol. (2012) 124:439–47. doi: 10.1007/s 00401-012-0998-0, PMID: 22661320 PMC 3422615 · doi ↗ · pubmed ↗
- 5Mackay A Burford A Carvalho D Izquierdo E Fazal-Salom J Taylor KR. Integrated molecular meta-analysis of 1,000 pediatric high-grade and diffuse intrinsic pontine glioma. Cancer Cell. (2017) 32:520–37. doi: 10.1016/j.ccell.2017.08.017, PMID: 28966033 PMC 5637314 · doi ↗ · pubmed ↗
- 6Aihara K Mukasa A Gotoh K Saito K Nagae G Tsuji S. H 3F 3A K 27M mutations in thalamic gliomas from young adult patients. Neuro Oncol. (2014) 16:140–6. doi: 10.1093/neuonc/not 144, PMID: 24285547 PMC 3870821 · doi ↗ · pubmed ↗
- 7Tanaka Y Natsumeda M Ohashi M Saito R Higa N Akahane T. Primary spinal cord gliomas: Pathologic features associated with prognosis. J Neuropathol Exp Neurol. (2024) 83:1010–19. doi: 10.1093/jnen/nlae 084, PMID: 39074166 · doi ↗ · pubmed ↗
- 8Louis DN. World Health Organization classification of tumours of the central nervous system. 5th ed edn. Lyon: International Agency for Research on Cancer (2021).