Potential active ingredients and mechanisms of Shufeitie ointment in the treatment of chronic obstructive pulmonary disease by integrating transdermal chemistry and network pharmacology
Jianing Sun, Di Zhang, Panpan Wang, Junhan Shi, Tan Xue, Panpan Zhang, Qi Wang, Xinjing Gui, Suyun Li, Jiansheng Li, Xuelin Li, Ruixin Liu

TL;DR
This study identifies key active ingredients in Shufeitie ointment that may treat COPD by reducing inflammation through specific biological pathways.
Contribution
The study combines transdermal chemistry and network pharmacology to reveal new insights into the mechanisms of Shufeitie ointment for COPD.
Findings
129 transdermal permeation components were identified in Shufeitie ointment.
Apigenin showed the strongest binding to key targets like EGFR, suggesting it plays a central role in COPD treatment.
The ointment may reduce COPD symptoms by inhibiting inflammatory pathways like AGE-RAGE and TNF.
Abstract
This study aims to identify the transdermal penetration components of Shufeitie ointment (SFTOT) and investigate the potential active components and mechanisms through which SFTOT exerts its effects on Chronic Obstructive Pulmonary Disease (COPD). An in vitro permeation test (IVPT) of SFTOT was conducted using a modified Franz diffusion cell method. Ultra-high-performance liquid chromatography-quadrupole/electrostatic field orbitrap high-resolution mass spectrometry (UHPLC-Q-Orbitrap/MS) was employed to analyze data from the transdermal receiving solution, enabling comprehensive identification of the components that permeate through the skin. To predict the potential mechanisms by which SFTOT may treat COPD, network pharmacology was used to construct a component-target-collaterals network. Additionally, molecular docking was applied to verify the interactions between the potential…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
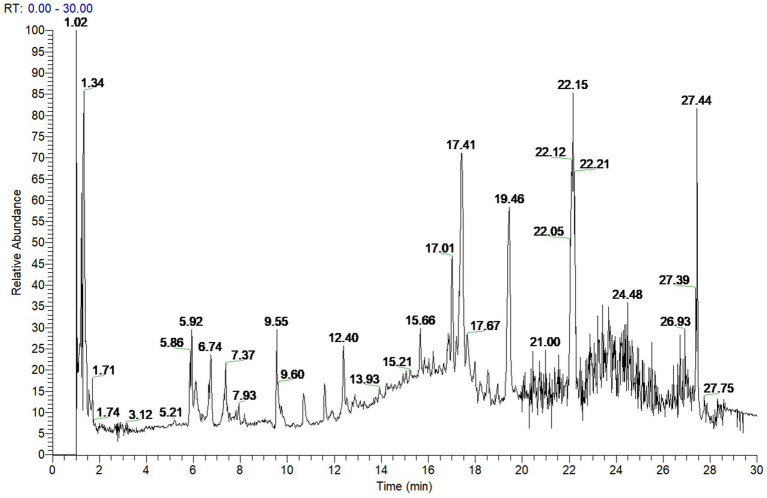 Figure 1
Figure 1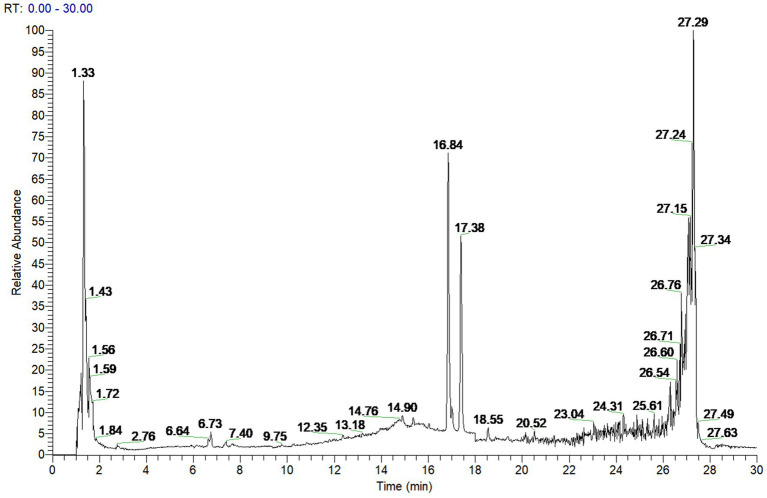 Figure 2
Figure 2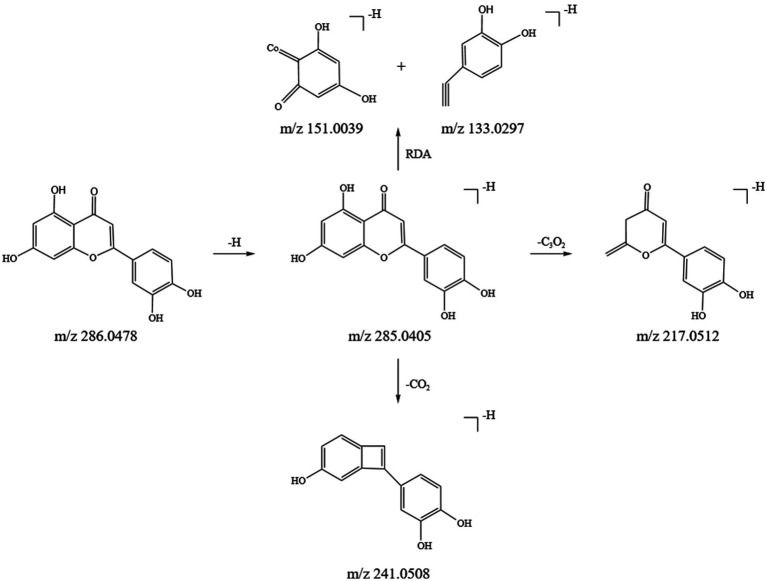 Figure 3
Figure 3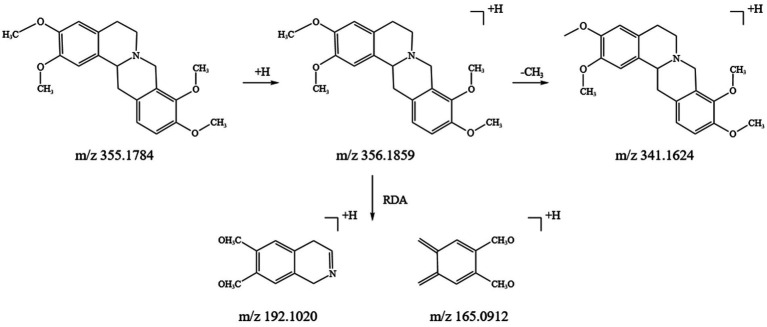 Figure 4
Figure 4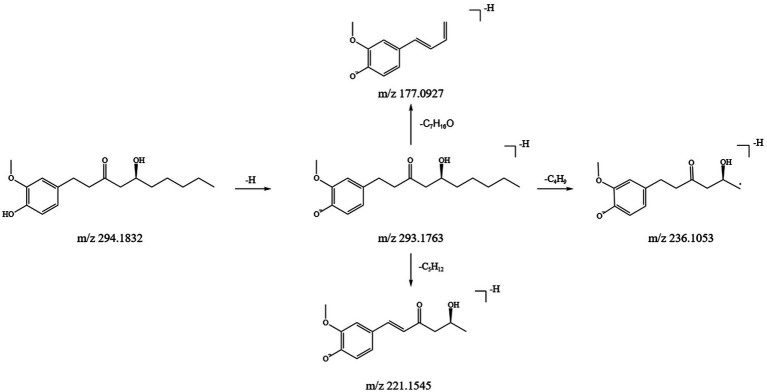 Figure 5
Figure 5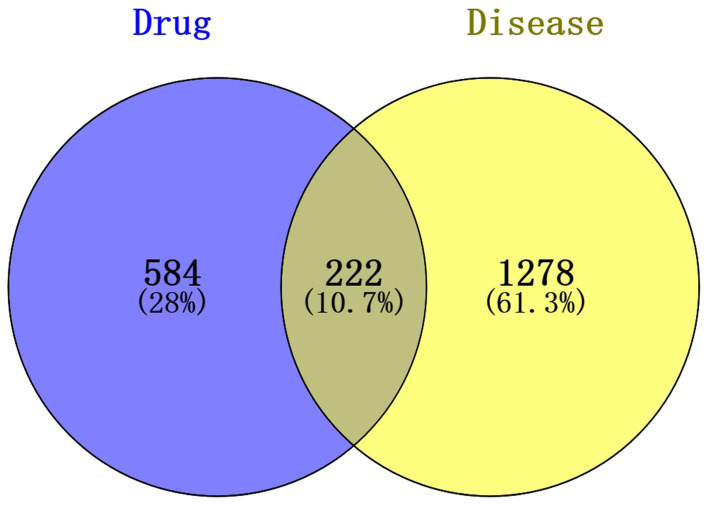 Figure 6
Figure 6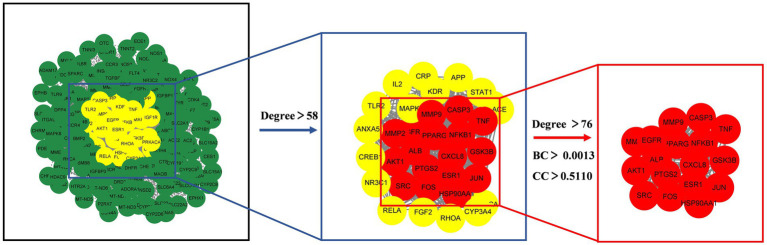 Figure 7
Figure 7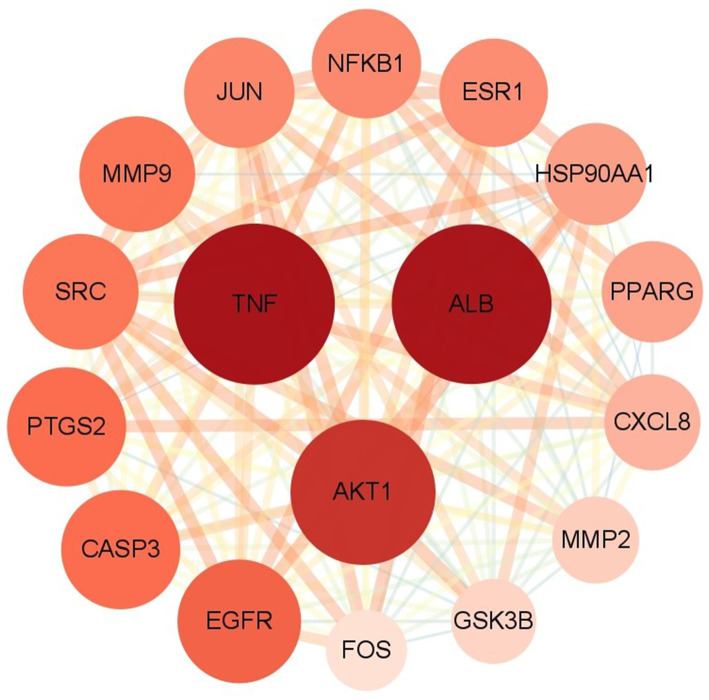 Figure 8
Figure 8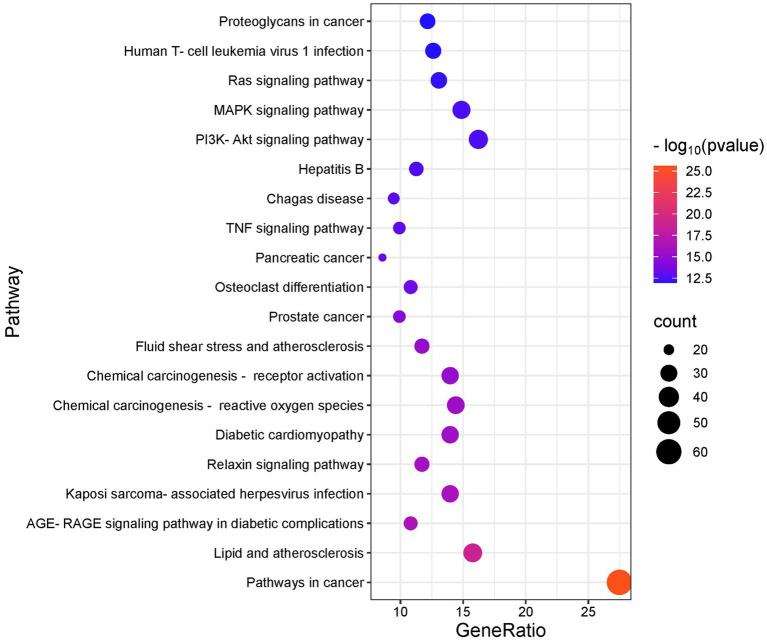 Figure 9
Figure 9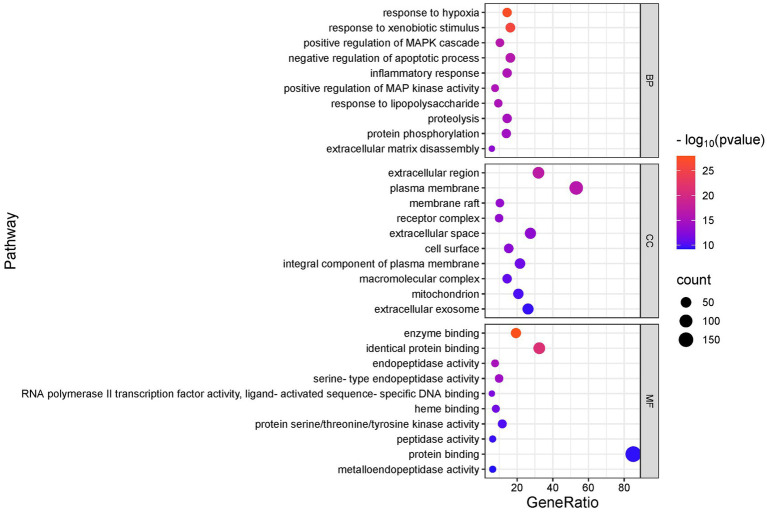 Figure 10
Figure 10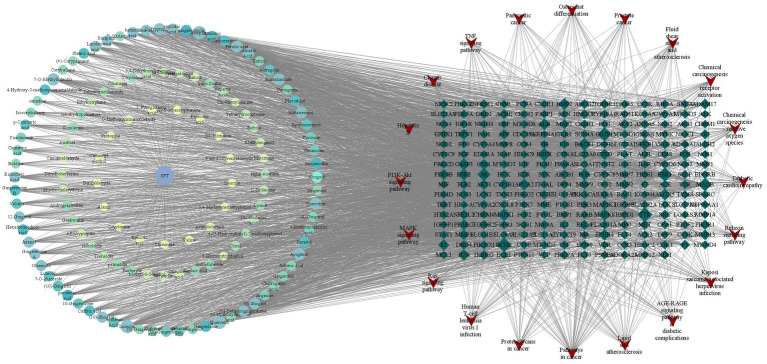 Figure 11
Figure 11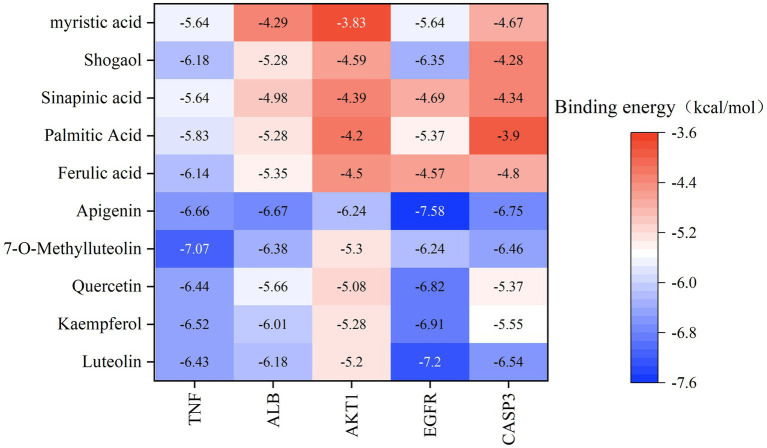 Figure 12
Figure 12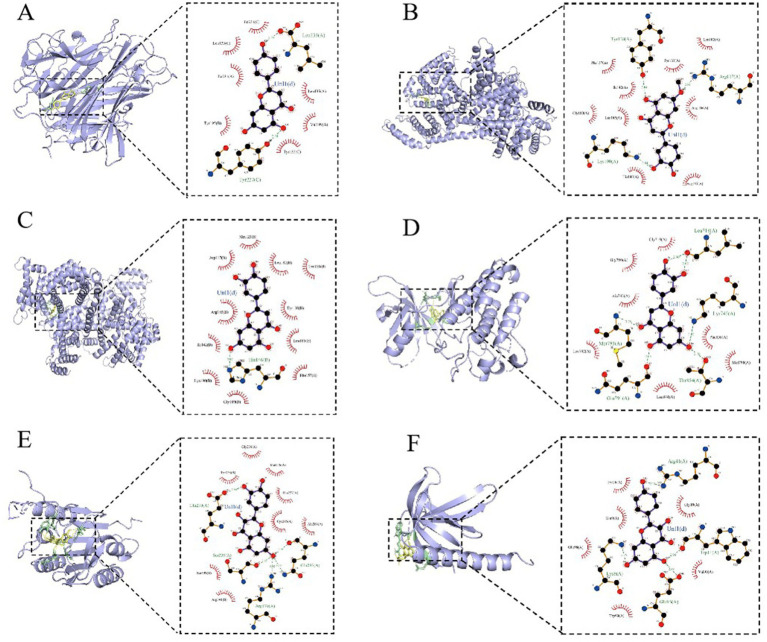 Figure 13
Figure 13| No. | tR/min | Compounds | Formula | Theoretical value(m/z) | Observed value(m/z) | Error(PPM) | Ion mode | Fragment ions (m/z) | Source |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 1.241 | Lysine | C6 H14 N2 O2 | 146.1055 | 147.1128 | −0.05 | [M + H]+ | 147.1134;130.0862;84.0806;56.0495 | JM |
| 2 | 1.249 | Arginine | C6 H14 N4 O2 | 174.1116 | 175.1189 | −0.19 | [M + H]+ | 175.1190;158.0923;116.0706;114.1017 | JM |
| 3 | 1.283 | Histidine | C6 H9 N3 O2 | 155.0695 | 156.0768 | 0.00 | [M + H]+ | 156.0768;110.0711;93.0446;83.0602 | JZ |
| 4 | 1.288 | trans-Zeatin | C10 H13 N5 O | 219.1120 | 220.1193 | 0.11 | [M + H]+ | 220.1193;202.1075;148.0618;136.0619 | JZ |
| 5 | 1.410 | Glutamic acid | C5 H9 N O4 | 147.0532 | 146.0460 | 0.28 | [M-H]− | 148.0604;130.0499;102.0549;84.0443 | JM |
| 6 | 1.435 | Pipecolic acid | C6 H11 N O2 | 129.0789 | 130.0862 | −0.51 | [M + H]+ | 130.0862;84.0807;56.0494 | JZ |
| 7 | 1.476 | Glutamine | C5 H10 N2 O3 | 146.0693 | 145.0620 | 0.88 | [M-H]− | 145.0621;128.0355;127.0515;109.0409;102.0561;84.046 | JZ |
| 8 | 1.504 | Alanin | C3 H7 N O2 | 89.0476 | 90.0549 | −1.18 | [M + H]+ | 90.0549;44.0495 | JM |
| 9 | 1.516 | Threonine | C4 H9 N O3 | 119.0582 | 118.0511 | −0.21 | [M + H]+ | 120.0654;102.0548;74.1600;56.0494 | JM |
| 10 | 1.549 | Trehalose | C12 H22 O11 | 342.1161 | 341.1089 | −0.21 | [M-H]− | 341.1090;179.0561;161.046; | JM |
| 11 | 1.584 | Isocorybulbine | C21 H25 N O4 | 355.1782 | 356.1858 | −0.4 | [M + H]+ | 356.1856;192.1019;151.0753 | CYHS |
| 12 | 1.596 | Luteolin 7-O-glucoside | C21 H20 O11 | 448.1007 | 447.0932 | 0.23 | [M-H]− | 447.0932;285.0405;133.0296;107.0141 | CYH |
| 13 | 1.596 | Quercitrin | C21 H20 O11 | 448.1006 | 447.0932 | −0.03 | [M-H]− | 447.0933;300.0277;271.0249;255.0301;178.9987;151.00310 | CYH |
| 14 | 1.705 | Aspartic Acid | C4 H7 N O4 | 133.0375 | 134.0447 | 0.03 | [M-H]− | 132.0304;116 (115.00376;114.01976);88.0404;74.0246 | JZ |
| 15 | 1.709 | Proline | C5 H9 N O2 | 115.0632 | 116.0705 | −1.04 | [M + H]+ | 116.0705;74.0237;70.0651 | JM |
| 16 | 1.895 | Valine | C5 H11 N O2 | 117.0789 | 118.0862 | −0.67 | [M + H]+ | 118.0862;72.0808;58.0651;55.0543 | JZ, JM |
| 17 | 1.964 | Isoleucine | C6 H13 N O2 | 131.0946 | 132.1018 | −0.63 | [M + H]+ | 132.1017;86.0963 | JZ, JM |
| 18 | 2.021 | 5-Hydroxytryptophol | C10 H11 N O2 | 177.0790 | 178.0862 | 0.14 | [M + H]+ | 178.0865;160.0606;132.0661 | JM |
| 19 | 2.236 | Leucine | C6 H13 N O2 | 131.0946 | 132.1018 | −0.63 | [M + H]+ | 132.1018;86.0963;69.0698 | JZ |
| 20 | 2.237 | Tyrosine | C9 H11 N O3 | 181.0739 | 165.0546 | 0.21 | [M + H]+ | 182.1814;165.0546;147.0443;136.0752;123.0439;119.0491;91.0539 | JZ, JM |
| 21 | 2.243 | Pyroglutamic acid | C5 H7 N O3 | 129.0426 | 130.0499 | 0.02 | [M + H]+ | 130.0498;84.0443;56.0494 | JZ |
| 22 | 2.370 | Phenylalanine | C9 H11 N O2 | 165.0790 | 166.0863 | 0.24 | [M + H]+ | 166.0870;120.0809;103.0543;93.0697;91.0542;79.0542 | JZ |
| 23 | 3.067 | Tryptophan | C11 H12 N2 O2 | 204.0898 | 203.0825 | −0.54 | [M-H]− | 203.0825;142.0667;116.0506;74.0247 | CYHS |
| 24 | 3.314 | 4-Methoxysalicylic acid | C8 H8 O4 | 168.0423 | 169.0495 | −0.03 | [M-H]− | 167.0349;123.0453 | JM |
| 25 | 3.345 | Ethylmorphine | C19 H23 N O3 | 313.1679 | 314.1752 | 0.45 | [M + H]+ | 314.1751;229;257 | CYHS |
| 26 | 4.113 | Chlorogenic acid | C16 H18 O9 | 354.0950 | 353.0877 | −0.14 | [M-H]− | 353.0884;191.0562;179.0351;161.0244;135.0453 | CYH |
| 27 | 4.820 | 3,4-Methylenedioxyphenol | C7 H6 O3 | 138.0317 | 137.0245 | 0.11 | [M-H]− | 137.0245;109.0296;107.0141 | XX |
| 28 | 5.435 | kakuol | C10 H10 O4 | 194.0580 | 195.0652 | 0.19 | [M + H]+ | 195.0651;147.0440 | XX |
| 29 | 5.442 | Caffeic acid | C9 H8 O4 | 180.0423 | 179.0350 | 0.12 | [M-H]− | 179.0349;135.0453 | CYH |
| 30 | 5.500 | Boldine | C19 H21 N O4 | 327.1472 | 328.1545 | 0.54 | [M + H]+ | 328.1548;297.1139;265.0859;178.0864 | CYHS |
| 31 | 5.500 | isoboldine | C19 H21 N O4 | 327.1472 | 328.1514 | 0.54 | [M + H]+ | 328.1538;297.1120;282.0882;265.0859;253.0841;237.0909;233.0595 | CYHS |
| 32 | 5.784 | Yuanhunine | C21 H25 N O4 | 355.1785 | 356.1858 | 0.32 | [M + H]+ | 356.1856;192.1019;177.0786 | CYHS |
| 33 | 5.908 | Dihydromelilotoside | C15 H20 O8 | 328.1159 | 327.1087 | 0.36 | [M-H]− | 327.1068;147.0452 | RG |
| 34 | 5.909 | Suberic acid | C8 H14 O4 | 174.0892 | 173.0819 | −0.14 | [M-H]− | 173.0819;111.0816;83.0502;53.0345 | JM |
| 35 | 5.952 | Protopine | C20 H19 N O5 | 353.1265 | 354.1337 | 0.38 | [M + H]+ | 354.1325;336.1221;275.0710;247.0750;206.0812;189.0786;188.0707;149.0598 | CYHS |
| 36 | 6.005 | tetrahydropalmatine | C21 H25 N O4 | 355.1784 | 356.1856 | 0.02 | [M + H]+ | 356.1859;341.1624;192.1020;165.0912 | CYHS |
| 37 | 6.130 | 3,4-Dihydroxybenzoic acid | C7 H6 O4 | 154.0267 | 153.0194 | 0.54 | [M-H]− | 153.0194;134.6277;109.0296 | RG, CYH |
| 38 | 6.137 | 4-Hydroxybenzaldehyde | C7 H6 O2 | 122.0296 | 121.0296 | 0.15 | [M-H]− | 121.0296;92.0268 | JZ |
| 39 | 6.137 | Tetrahydrocoptisine | C19 H17 N O4 | 323.1158 | 324.1232 | 0.16 | [M + H]+ | 324.1230;176.0705;149.0597 | CYHS |
| 40 | 6.173 | Scoulerine | C19 H21 N O4 | 327.1471 | 328.1544 | 0.24 | [M + H]+ | 328.1542;178.0862;151.0753;119.0491;91.0542 | CYHS |
| 41 | 6.558 | Corybulbine | C21 H25 N O4 | 355.1784 | 356.1857 | 0.22 | [M + H]+ | 356.1857;179.1067;178.0861;163.0622 | CYHS |
| 42 | 6.574 | 4’-Hydroxyacetophenone | C8 H8 O2 | 136.0524 | 135.0452 | −0.12 | [M-H]− | 135.0450;120.0214 | JZ |
| 43 | 6.582 | Dihydroberberine | C20 H19 N O4 | 337.1314 | 338.1387 | 0.03 | [M + H]+ | 338.1386;322.1073;320.0922;306.1123;294.1123;293.1047;280.0965 | CYHS |
| 44 | 6.658 | Astragalin | C21 H20 O11 | 448.1004 | 447.0930 | −0.34 | [M-H]− | 447.0931;285.0402;284.0325;256.0368;227.0350 | XX, CYH |
| 45 | 6.690 | Allocryptopine | C21 H23 N O5 | 369.1577 | 370.1650 | 0.21 | [M + H]+ | 370.1646;352.1549;291.1005;290.0937;188.0705 | CYHS |
| 46 | 6.782 | isoquercetin | C21 H20 O12 | 464.0956 | 463.0883 | 0.21 | [M-H]− | 463.0885;301.0355;300.0277;271.0250;255.03001;151.0039 | CYH |
| 47 | 6.914 | 7-O-Methylluteolin | C16 H12 O6 | 300.0634 | 301.0706 | −0.09 | [M-H]− | 299.0559;284.0326;256.0385;227.0349;151.0039;133.0300 | CYH |
| 48 | 6.968 | Anethol | C10 H12 O | 148.0888 | 181.1223 | −0.26 | [M + H]+ | 149.0960;105.0701;91.0541 | RG |
| 49 | 7.004 | 4-(3-Hydroxybutyl)-2-methoxyphenol | C11 H16 O3 | 196.1100 | 197.1172 | 0.02 | [M + H]+ | 197.1173;179.1065;161.0962;137.0591;135.0805;133.1011;107.0855;93.0698 | GJ |
| 50 | 7.205 | canadine | C20 H21 N O4 | 339.1472 | 340.1545 | 0.47 | [M + H]+ | 340.1546;176.0707 | CYHS |
| 51 | 7.266 | Berberine | C20H17NO4 | 335.1159 | 336.1231 | 0.27 | [M + H]+ | 336.1228;320.0916;306.0758;278.0810 | CYHS |
| 52 | 7.301 | (+)-Corypalmine | C20 H23 N O4 | 341.1627 | 342.1701 | −0.07 | [M + H]+ | 342.1698;178.0860;151.0752;119.0489;91.05410 | CYHS |
| 53 | 7.355 | Benzaldehyde | C7 H6 O | 106.0418 | 107.0490 | −1.09 | [M + H]+ | 107.0491;79.0542 | RG |
| 54 | 7.518 | Ferulic acid | C10 H10 O4 | 194.0579 | 193.0505 | −0.28 | [M + H]+ | 195.0644;177.0546;145.0284;121.0626;117.0334;89.0383 | XX |
| 55 | 7.838 | Sinapinic acid | C11 H12 O5 | 224.0685 | 207.0652 | −0.05 | [M-H]− | 223.0613;208.0373;164.0477;179.0716;149.0244 | JZ |
| 56 | 7.846 | Quercetin | C15 H10 O7 | 302.0426 | 301.0353 | −0.06 | [M-H]− | 301.0352;151.0037;149.0244;107.0128 | CYH |
| 57 | 7.973 | Jaranol | C17 H14 O6 | 314.0791 | 315.0864 | 0.28 | [M + H]+ | 315.180859;300.0625 | CYH |
| 58 | 8.224 | Myristicin | C11 H12 O3 | 192.0787 | 193.0859 | 0.12 | [M + H]+ | 193.0855;161.0609 | XX |
| 59 | 8.256 | Cryptopine | C21 H23 N O5 | 369.1577 | 370.1650 | 0.23 | [M + H]+ | 370.2011;205.1095;190.0862;165.0808;150.0674 | CYHS |
| 60 | 8.277 | Cinnamic acid | C9 H8 O2 | 148.0524 | 147.0452 | −0.15 | [M-H]− | 147.0453;102.9488 | RG |
| 61 | 8.454 | Corydaline | C22 H27 N O4 | 369.1939 | 370.2012 | −0.20 | [M + H]+ | 370.2013;205.1098;192.1019;179.1067;165.0910;151.0753;150.0675;136.0517;135.0448 | CYHS |
| 62 | 8.468 | Medioresinol | C21 H24 O7 | 388.1523 | 387.1449 | 0.18 | [M-H]− | 387.1443;207.0664;163.0756 | CYHS |
| 63 | 8.535 | Sebacic acid | C10 H18 O4 | 202.1205 | 201.1132 | −0.24 | [M-H]− | 201.1132;186.1027;139.1130 | JM |
| 64 | 8.606 | Coumarin | C9 H6 O2 | 146.0371 | 147.0445 | 2.26 | [M + H]+ | 147.0441;119.0491;103.0542;91.0542 | GJ, JZ |
| 65 | 9.075 | Naringenin | C15 H12 O5 | 272.0684 | 273.0758 | −0.14 | [M-H]− | 271.0610;151.0037 | XX, CYH |
| 66 | 9.161 | Kaempferol | C15 H10 O6 | 286.0478 | 285.0405 | 0.30 | [M + H]+ | 287.0549;258.0516;165.0184;133.0282;121.0284 | XX, CYH |
| 67 | 9.178 | Syringaldehyd | C9 H10 O4 | 182.0579 | 181.0506 | −0.15 | [M-H]− | 181.0510;166.0272;151.0038 | XX |
| 68 | 9.184 | Gingerenone B | C22 H26 O6 | 386.173 | 387.1804 | 0.26 | [M + H]+ | 387.1804;207.1015;193.0863;167.0699;137.0596 | GJ |
| 69 | 9.230 | dihydrochelerythrine | C21 H19 N O4 | 349.1317 | 350.1389 | 0.73 | [M + H]+ | 350.1384;334.1072;319.1214;290.0822 | CYHS |
| 70 | 9.359 | Genkwanin | C16 H12 O5 | 284.0684 | 283.0611 | −0.30 | [M-H]− | 283.0249;268.0365;211.0400;117.0347 | CYH |
| 71 | 9.657 | Umbelliferone | C9 H6 O3 | 162.0317 | 163.0390 | −0.05 | [M + H]+ | 163.0396;135.0803;119.0488;107.0491;91.0542 | CYH |
| 72 | 9.720 | Matairesinol | C20 H22 O6 | 358.1417 | 357.1343 | 0.07 | [M-H]− | 357.1345;342.1106;298.9558;221.0819;161.0616;147.0453;16137.0609;122.0373 | CYH |
| 73 | 9.720 | Camphoric acid | C10 H16 O4 | 200.1049 | 199.0976 | 0.08 | [M-H]− | 199.0973;155.1078 | JM |
| 74 | 9.748 | p-Coumaric acid | C9 H8 O3 | 164.0474 | 163.0401 | 0.30 | [M-H]− | 163.0401;162.0312;162.1440;145.0297;135.0452;93.0347;75.1221;74.9537 | RG |
| 75 | 9.825 | Apigenin | C15 H10 O5 | 270.0527 | 271.0599 | −0.57 | [M-H]− | 269.0459;149.0247;117.034;107.0140 | CYH |
| 76 | 9.936 | Cinnamaldehyde | C9 H8 O | 132.0574 | 133.0646 | −1.12 | [M + H]+ | 133.0647;115.0541;91.0541;79.0542 | RG |
| 77 | 9.942 | Epipinoresinol | C20 H22 O6 | 358.1417 | 357.1344 | 0.20 | [M-H]− | 357.1343;151.0760 | XX |
| 78 | 10.554 | Pluviatilol | C20 H20 O6 | 356.1259 | 357.1330 | −0.27 | [M + H]+ | 357.1330;339.1226;205.0858;191.0871 | XX |
| 79 | 10.582 | alpha-Asarone | C12 H16 O3 | 208.1100 | 207.1026 | 0.13 | [M + H]+ | 209.1167;194.0934;178.099;168.0779;153.0544 | XX |
| 80 | 10.758 | Cinnamyl alcohol | C9 H10 O | 134.0731 | 135.0804 | −0.36 | [M + H]+ | 135.0804;105.0697;91.0541;79.0541 | RG |
| 81 | 10.872 | Bergapten | C12 H8 O4 | 216.0422 | 217.0495 | −0.34 | [M + H]+ | 217.0502;202.0268;173.0600 | JM |
| 82 | 11.021 | Sesamolin | C20 H18 O7 | 370.1053 | 371.1126 | 0.06 | [M + H]+ | 371.1129;353.0912;203.0862;135.0440 | XX |
| 83 | 11.246 | Luteolin | C15 H10 O6 | 286.0478 | 285.0405 | 0.05 | [M-H]− | 285.0405;241.0508;217.0512;151.0039;133.0297 | CYH |
| 84 | 11.274 | zingerone | C11 H14 O3 | 194.0943 | 195.1016 | −0.10 | [M + H]+ | 195.1015;161.0027;137.0592;117.0281 | GJ |
| 85 | 11.330 | 4-Hydroxy-3-methoxycinnamaldehyde | C10 H10 O3 | 178.0630 | 179.0703 | −0.04 | [M + H]+ | 179.1701;161.0599;147.0439;119.0490;91.0542;65.0385 | RG |
| 86 | 11.388 | Jasmonic acid | C12 H18 O3 | 210.1254 | 211.1327 | −0.73 | [M-H]− | 209.1182;165.1284;59.012 | JZ |
| 87 | 11.389 | Gingerdiol | C17 H28 O4 | 296.1988 | 295.1915 | 0.18 | [M-H]− | 295.19135;280.1680 | GJ |
| 88 | 11.410 | O-Methoxycinnamaldehyde | C10 H10 O2 | 162.0681 | 163.0754 | −0.03 | [M + H]+ | 163.0754;133.0650;131.0492;107.0491;105.0698;91.0542;79.0541 | RG |
| 89 | 11.703 | Citral | C10 H16 O | 152.1201 | 153.1274 | 0.18 | [M + H]+ | 153.1272;135.1168;95.08855;71.0491;69.0697;59.0491 | JM |
| 90 | 11.864 | Velutin | C17 H14 O6 | 314.0790 | 315.0862 | −0.28 | [M + H]+ | 315.0863;300.0629;272.0679 | CYH |
| 91 | 12.008 | Methyleugenol | C11 H14 O2 | 178.0993 | 179.1066 | −0.25 | [M + H]+ | 179.1065;164.0828;151.0753;138.0674 | XX |
| 92 | 12.231 | Aristololactam | C17 H11 N O4 | 293.0690 | 294.0762 | 0.54 | [M + H]+ | 294.0761;279.0527;251.0579;239.0708 | XX |
| 93 | 12.370 | 10-Hydroxydecanoic acid | C10 H20 O3 | 188.1412 | 187.1340 | 0.00 | [M-H]− | 187.1340;141.1286 | JM |
| 94 | 12.488 | Hexadecanedioic acid | C16 H30 O4 | 286.2145 | 285.2072 | 0.15 | [M-H]− | 285.2072;267.1966;241.2170 | JM |
| 95 | 13.218 | Azelaic acid | C9 H16 O4 | 188.1048 | 187.0975 | −0.10 | [M-H]− | 187.0975;143.1075;125.0972;123.0811;97.0659 | JM |
| 96 | 13.321 | Andrographolide | C20 H30 O5 | 350.2094 | 351.2167 | 0.28 | [M-H]− | 349.2021;331.1905;287.2016 | JM |
| 97 | 13.426 | Gingerenone A | C21 H24 O5 | 356.1625 | 357.1699 | 0.39 | [M + H]+ | 357.1709;339.1235;177.091;163.075;137.0596;145.0649;131.0490 | GJ |
| 98 | 13.668 | palmatine | C21 H22 N O4 | 352.1550 | 353.1623 | 0.35 | [M + H]+ | 353.1624 | CYHS |
| 99 | 13.789 | (8)-Gingerol | C19 H30 O4 | 322.2144 | 321.2071 | −0.19 | [M-H]− | 321.2072;305.0950;127.1130;57.0346 | GJ |
| 100 | 13.809 | alpha-Curcumene | C15 H22 | 202.1721 | 203.1794 | −0.12 | [M + H]+ | 203.1794;161.1326;147.1168;133.1011;119.0853;105.0698;95.0854;81.0698;69.0698 | GJ, XX |
| 101 | 13.935 | Aurantiamide | C25 H26 N2 O3 | 402.1944 | 403.2018 | 0.09 | [M + H]+ | 403.1181;152.1071 | CYH |
| 102 | 13.947 | Paradol | C17 H26 O3 | 278.1882 | 279.1955 | −0.07 | [M + H]+ | 279.1952;261.1868;229.1567;177.0912;163.0754;137.1597;131.0490;103.0540;81.0698 | GJ |
| 103 | 14.104 | pinolenic acid | C18 H30 O2 | 278.2244 | 279.2317 | −0.50 | [M + H]+ | 279.2318;95.0855;91.0699;67.0542 | JM |
| 104 | 14.642 | Gingerdione | C17 H24 O4 | 292.1677 | 275.1643 | 0.67 | [M + H]+ | 293.1749;233.1537;163.0755;137.0597;131.0492 | GJ |
| 105 | 14.657 | (8)-Gingerdione | C19 H28 O4 | 320.1988 | 321.2061 | 0.21 | [M + H]+ | 321.2061;303.2339;261.1852;229.1589;207.1375;191.1075;163.0753;137.0596;95.0853 | GJ |
| 106 | 14.778 | [6]-Dehydrogingerdione | C17 H22 O4 | 290.1518 | 291.1591 | 0.05 | [M + H]+ | 291.1590;270.4919;177.0545;145.0283;103.2844;89.0384;71.0854 | GJ |
| 107 | 14.905 | (10)-Shogaol | C21 H32 O3 | 332.2352 | 333.2425 | 0.29 | [M + H]+ | 333.3425;315.2318;197.1911;177.0909;162.0673;145.0647;137.0596;83.0852 | GJ |
| 108 | 15.224 | Shogaol | C17 H24 O3 | 276.1727 | 277.1799 | 0.37 | [M + H]+ | 277.1810;137.0597 | GJ |
| 109 | 15.225 | Safrole | C10 H10 O2 | 162.0681 | 163.0753 | −0.17 | [M + H]+ | 163.0753;148.0519;135.0803;133.0648;131.0492;121.0647;120.0568;115.0541;107.0499;105.1697;103.0541;91.0544;79.0541;77.0386;55.0178 | XX |
| 110 | 15.284 | (10)-Gingerol | C21 H34 O4 | 350.2457 | 349.2384 | −0.10 | [M + H]+ | 351.2510;333.2384;315.2331;179.0603;137.0595;83.0856 | GJ |
| 111 | 15.507 | 6-Gingerol | C17 H26 O4 | 294.1832 | 277.1799 | 0.22 | [M-H]− | 293.1763;236.1053;221.1545;177.0927 | GJ |
| 112 | 15.822 | Benzoic acid | C7 H6 O2 | 122.0369 | 121.0297 | 1.30 | [M-H]− | 121.0294;77.040 | CYH |
| 113 | 16.210 | Estriol | C18 H24 O3 | 288.1726 | 321.2062 | 0.18 | [M-H]− | 287.2230;171.1028;145.0870;143.1080 | XX |
| 114 | 16.245 | (+)-syringaresinol | C22 H26 O8 | 418.1627 | 417.1554 | −0.24 | [M-H]− | 417.1550;387.1114;181.0507;166.0260 | CYH |
| 115 | 16.563 | 16-Hydroxyhexadecanoic acid | C16 H32 O3 | 272.2352 | 271.2279 | 0.02 | [M-H]− | 271.2278;253.2187;225.2222;155.1440 | JM |
| 116 | 16.634 | (8)-Shogaol | C19 H28 O3 | 304.2039 | 305.2112 | 0.09 | [M + H]+ | 305.2112;287.2013;177.0908;162.0672;137.0596;95.0856;83.0855 | GJ |
| 117 | 16.862 | 12-Gingerol | C23 H38 O4 | 378.2771 | 377.2698 | 0.31 | [M + H]+ | 379.284;361.273;343.254;177.1632;137.0961;109.1014;95.0854 | GJ |
| 118 | 17.139 | Linolenic Acid | C18 H30 O2 | 278.2246 | 279.2319 | −0.05 | [M + H]+ | 279.2316;179.1436;125.0963 | JM |
| 119 | 17.472 | 10-Gingerdione | C21 H32 O4 | 348.2302 | 349.2375 | 0.39 | [M + H]+ | 349.2286;331.2265;193.0867;177.0901;155.1429;145.0283;135.0451;83.0857;57.0698 | GJ |
| 120 | 17.512 | myristic acid | C14 H28 O2 | 228.2090 | 227.2017 | 0.34 | [M-H]− | 227.2016 | XX |
| 121 | 17.625 | Methyl-6-Gingerol | C18 H28 O4 | 308.1989 | 309.2061 | 0.35 | [M + H]+ | 309.2008;291.1955;276.9002;177.1279;151.1118;99.0804;71.0855 | GJ |
| 122 | 18.510 | Linoleic acid | C18 H32 O2 | 280.2402 | 279.1229 | −0.12 | [M-H]− | 279.2326;261.2224 | XX, JM, CYH |
| 123 | 18.937 | Ricinoleic Acid | C18 H34 O3 | 298.2507 | 297.2435 | −0.21 | [M-H]− | 297.2436;279.2333;183.1387 | JM |
| 124 | 20.326 | (4)-Gingerol | C15 H22 O4 | 266.1553 | 265.1480 | 12.98 | [M-H]− | 267.1595;189.1285;169.0865;151.0751;119.0855;83.0489 | GJ |
| 125 | 21.601 | Stearic acid | C18 H36 O2 | 284.2716 | 283.2643 | 0.25 | [M-H]− | 283.2641;143.5420 | RG |
| 126 | 21.635 | Oleamide | C18 H35 N O | 281.2719 | 282.2790 | 0.25 | [M + H]+ | 282.2799;265.2522;97.1011;83.0855 | JM |
| 127 | 23.091 | Palmitic Acid | C16 H32 O2 | 256.2403 | 255.2330 | 0.23 | [M-H]− | 255.2330;183.0441;116.5201 | XX, CYH |
| 128 | 24.794 | Oleic acid | C18 H34 O2 | 282.2560 | 281.2486 | 0.15 | [M-H]− | 281.2485;183.7570 | JM, CYH |
| 129 | 26.875 | behenic acid | C22 H44 O2 | 340.3340 | 339.3267 | −0.39 | [M-H]− | 339.3274;321.3149;183.0122;59.0398 | RG |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHerbal Medicine Research Studies · Psidium guajava Extracts and Applications · Mangiferin and Mango Extracts
Introduction
1
Chronic Obstructive Pulmonary Disease (COPD) is a progressive respiratory disorder characterized by airflow limitation. Although its pathogenesis remains incompletely understood, multiple factors contribute to its development, including smoking, occupational exposure to dust and chemicals, air pollution, infections, and an imbalance between proteases and antiproteases (1). Additionally, autonomic dysfunction, heightened airway responsiveness, and chronic inflammation play crucial roles in disease progression (2). The primary clinical symptoms of COPD include cough, sputum production, and dyspnea (3). As the disease advances, patients may develop respiratory failure, pulmonary hypertension, and pulmonary heart disease, which can become life-threatening. COPD is associated with three major burdens: high prevalence, high mortality, and substantial economic costs. According to the Global Burden of Disease Study (2019), an estimated 212.3 million people worldwide had COPD (4). In 2021, the World Health Organization reported that COPD caused 3.5 million deaths, accounting for approximately 5% of total global mortality. As the fourth leading cause of death worldwide (5), COPD is a critical public health concern requiring urgent attention.
In recent years, Chinese medicine has made significant strides in treating COPD. In Traditional Chinese Medicine (TCM), COPD falls under the categories of lung distension, cough, and asthma. TCM treatment approaches include both internal and external therapies. Internal treatments primarily involve the oral administration of traditional Chinese medicinal decoctions and patent medicines, such as Liuwei Buqi Decoction (6), Shiwei Longdanhua Decoction (7), Jianpi Yifei II Granules (8), and Bufei Jianpi Granules (9). These therapies have been shown to effectively alleviate chronic inflammation and enhance respiratory function in COPD patients. The underlying mechanism may involve the inhibition of inflammatory responses and the reduction of airway epithelial cell apoptosis (10). External treatments include application therapy, acupuncture, and fumigation therapy, all of which have demonstrated positive effects in alleviating COPD symptoms and promoting rehabilitation (11–13). Acupoint application therapy (14, 15), in particular, is a distinctive treatment modality in TCM, grounded in traditional theories and ancient clinical experience. It integrates the concepts of acupoints, meridians, and medicinal substances. By stimulating acupoints and facilitating drug absorption through the skin, this therapy promotes the circulation of qi and blood, unblocks meridians, and helps regulate the zang-fu organs. This approach has shown significant preventive and therapeutic effects on various chronic respiratory diseases, leveraging both the meridian and medicinal properties. The mechanism of action is thought to involve immune regulation and the inhibition of airway inflammation and remodeling.
Shufeitie ointment [SFTOT; Approval No. Yuyao Zhizi Z20120014 (Zheng)] is an external preparation developed by the First Affiliated Hospital of Henan University of Traditional Chinese Medicine. It was formulated based on over 40 years of clinical experience and integrates modern pharmacology and preparation technology. As a novel external treatment for COPD, SFTOT consists of seven traditional Chinese medicinal ingredients, including Sinapis Semen (Sinapis alba L., or Brassica juncea (L.)Czern. et Coss., Jiezi), Genkwa Flos (Daphne genkwa Sieb. et Zucc., Cuyuanhua), Corydalis Rhizoma (Corydalis yanhusuo W. T. Wang., Cuyanhusuo), Cinnamomi Cortex (Cinnamomum cassia Presl., Rougui), Semen Zanthoxyli (Zanthoxylum bungeanum Maxim or Zanthoxylum schinifolium Sieb.et Zucc., Jiaomu), Asari Radix Et Rhizoma (Asarum heterotropoides Fr. Schmidt var. mandshuricum (Maxim.) Kitag., or Asarum sieboldii Miq.var. seoulense Nakai., or Asarum sieboldii Miq., Xixin), Zingiberis Rhizoma (Zingiber officinale Rosc., Ganjiang). Modern pharmacological studies have demonstrated that SFTOT reduces inflammatory cytokines, including tumor necrosis factor (TNF), thereby alleviating inflammation in the airways and lung tissue. Additionally, it significantly increases immunoglobulin levels in COPD rats and modulates T lymphocyte expression, which helps improve lung function and mitigate pathological lung tissue damage (16). These findings align with the pathological and mechanistic understanding of COPD. Clinical studies have shown that the control group was treated with western medicine, and the experimental group was treated with SFTOT acupoint external application combined with western medicine. Each group included 38 patients with acute exacerbation of chronic obstructive pulmonary disease in winter. The results showed that the total effective rate of the experimental group was 94.74%, which was significantly higher than 78.95% of the control group (p < 0.05). The improvement of respiratory function in the experimental group was significantly better than that in the control group (p < 0.05). There was no significant difference in the incidence of adverse reactions between the two groups (p > 0.05) (17). Further observation of patients with stable COPD found that the selection of bilateral Feishu, bilateral Shenshu, Dazhui, Tanzhong and other acupoints for SFTOT application treatment, 8 ~ 12 h application time can effectively alleviate the symptoms of acute exacerbation of COPD, the clinical effect is significant. The study also suggests that the foaming phenomenon after application may be positively correlated with the clinical effect (18, 19). However, systematic and comprehensive studies on the active components and pharmacological mechanisms of SFTOT in COPD treatment remain limited. Therefore, this study aims to identify the transdermal active components of SFTOT and elucidate its mechanism of action against COPD.
TCM compounds exhibit therapeutic effects through multi-component, multi-channel, and multi-target mechanisms. Understanding the pharmacodynamic material basis of these compounds is essential for their development and for elucidating their pharmacological mechanisms. To evaluate the efficacy of SFTOT in COPD treatment, we employed a Franz diffusion cell system combined with UHPLC-Q-Orbitrap/MS technology to investigate its skin permeability. Additionally, we used network pharmacology and molecular docking techniques to identify potential active components and explore their mechanisms of action. This approach overcomes the limitations of previously unknown components and mechanisms of SFTOT, providing valuable insights for new drug development.
Materials and methods
2
Chemicals and reagents
2.1
We sourced all decoction pieces from Henan Zhongyi Pharmaceutical Co., Ltd. (Zhengzhou, China) and Shi Junhan, Deputy Director of the First Affiliated Hospital of Henan University of Traditional Chinese Medicine, verified their authenticity. The ingredients included Sinapis Semen (JieZi, JZ; No: J5772113), Corydalis Rhizoma (CuYanHuSuo, CYHS; No: 230304), Zingiberis Rhizoma (GanJiang, GJ; No: 221201), Asari Radix Et Rhizoma (XiXin, XX; No: 20031316), Cinnamomi Cortex (RouGui, RG; No: 22120207), Semen Zanthoxyli (JiaoMu, JM; No: 2209211), and Genkwa Flos (CuYuanHua, CYH; No: 211102). Sodium carboxymethyl cellulose (No: B2215321) and glycerol (No: D2213012) from Shanghai Aladdin Biochemical Technology Co., Ltd. (Shanghai, China). Ethanol (No: 20220908) from Kangbao Biochemical Technology Co., Ltd. (Shandong, China). Laurocapram (No: 20210302) from Xinxiang Gaojin Pharmaceutical Co., Ltd. (Henan, China). 0.9% NaCl aqueous solution (No: A22120801A) from Henan Kelun Pharmaceutical Co., Ltd. (Henan, China).
Chromatographic acetonitrile and Pierce™ formic acid (chromatographic grade) were purchased from Thermo Fisher (Massachusetts, United States). Chromatographic grade methanol was obtained from Shanghai Aladdin Biochemical Technology Co., Ltd. (Shanghai, China). Ultrapure water was supplied by the Elemental 18,120 Molecular ultrapure water system from Shanghai Moller Scientific Instrument Co., Ltd. (Shanghai, China). The back skin of SPF BALB/C-nu mice was obtained from Yantai Raphael Biotechnology Co., Ltd. (Shandong, China) under License No. SCXK (Lu) 2022–0006 and Animal Certificate No. 370726221101453317.
Shufeitie ointment preparation
2.2
Following the established preparation method for SFTOT at the hospital (20), volatile oils were extracted from JieZi (JZ), GanJiang (GJ), XiXin (XX), JiaoMu (JM), and RouGui (RG) through steam distillation. The resulting distilled water solution was reserved for later use. CuYanHuSuo (CYHS) and CuYuanHua (CYH) were added to the remaining dregs, followed by the addition of 10 times the amount of 70% ethanol. The mixture was refluxed and extracted three times, each for 1 h. The three extracts were combined, filtered, and the filtrate was mixed with the previously prepared aqueous solution. The ethanol was removed by vacuum distillation, and the resulting concentrated mixture was turned into a clear paste and set aside. Next, sodium carboxymethyl cellulose was added to the paste and allowed to swell overnight. After thorough stirring, volatile oil, glycerol, and azone were incorporated. The mixture was stirred to ensure homogeneity, defoamed, and the final preparation was obtained.
In vitro penetration test
2.3
Preparation of the isolated skin
2.3.1
The previously prepared mouse skin was removed from storage at −20°C and placed in normal saline at room temperature for 15 min to thaw. For each mouse, three skin samples were selected and cut into three pieces, each corresponding to the area of the diffusion pool.
Weighing transdermal drug samples
2.3.2
Three portions of Shufeitie ointment (SFTOT) were weighed in parallel, with each portion weighing approximately 1.03 ± 0.01 g, 1.02 ± 0.01 g, and 1.02 ± 0.01 g, respectively.
Collection of samples
2.3.3
The in vitro transdermal absorption experiment of SFTOT was conducted using a Franz diffusion cell system (Model #TPY-2, Shanghai Huanghai Drug Control Instrument Co., Ltd., China). The system consisted of a heating cycle, a temperature control system, magnetic stirring, a vertical diffusion cell with a 25 mL receptor capacity, and an effective diffusion area of 3.14 cm^2^. The upper chamber served as the diffusion cell, while the lower chamber acted as the receiving cell. The isolated skin, as described in section 2.3.1, was fixed between the diffusion pool and the receiving pool, with the stratum corneum facing the diffusion pool. The drug, as weighed in Section 2.3.2, was evenly applied to the stratum corneum of the rat skin, and the diffusion pool was sealed with a sealing film. A magnet was placed in the receiving pool, which contained 7 mL of normal saline, preheated to 32°C and degassed by ultrasound. The liquid surface was in contact with the inner layer of the skin to avoid bubbles between the rat skin and the receiving liquid. If necessary, additional normal saline at the same temperature was added, and any bubbles in the inclined diffusion pool were removed. After setup, the system was maintained at a constant temperature of 32 ± 1°C using a preheated water bath, and stirring was initiated at a constant speed of 300 rpm. Samples were taken at 1, 2, 4, 6, 8, and 12 h and placed into 100 mL centrifuge tubes. An equal volume of degassed homothermal receiving liquid was immediately added to each sample.
Analysis of Shufeitie ointment transdermal permeation components via UHPLC-Q-Orbitrap/MS
2.4
Testing conditions
2.4.1
Chromatographic separation was performed using an Ultimate 3,000 ultra-high-performance liquid chromatography (UHPLC) system (Thermo, United States) equipped with a Hypersil GOLD™ VANQUISH™ C_18_ column (2.1 mm × 100 mm, 1.9 μm). The column was maintained at 40°C, and the flow rate was set to 0.2 mL/min. The mobile phase consisted of 0.1% formic acid in water (A) and acetonitrile (B), with a gradient elution as follows: 0–7 min, 10–40% B; 7–13 min, 40–80% B; 13–25 min, 80–95% B; 25–25.1 min, 95–10% B; 25.1–30 min, 10–10% B. The injection volume was 5 μL.
Mass spectrometry detection was performed using an Orbitrap Exploris 240 MS (Thermo, United States). Electrospray ionization (ESI) was carried out in both positive ion (ESI^+^) and negative ion (ESI^−^) modes. The optimized ESI-MS parameters were as follows: spray voltages of 3,500 V (positive mode) and 3,000 V (negative mode), sheath gas flow rate of 35 Arb, auxiliary gas flow rate of 12 Arb, and a capillary temperature of 350°C. Full Scan/dd-MS^2^ scanning mode was used with a Full MS resolution of 60,000 and dd-MS^2^ resolution of 15,000. The collision energy was set to 20, 40, and 60 eV, and the scanning range was m/z 70–1,050.
Treatment of samples
2.4.2
At 6 time points, 3 mL of the transdermal receiving solution, as described in Section 2.3.3, was pooled. The solution was evaporated to dryness at 45°C using a centrifugal concentrator, then reconstituted in 1 mL of methanol. The mixture was filtered through a 0.22 μm filter membrane, centrifuged at 14,000 rpm for 10 min at 20°C, and the supernatant was collected after two centrifugation steps for further analysis.
Data analysis
2.4.3
Following data collection, the raw data from the UHPLC-Orbitrap Exploris 240 system were imported into Compound Discoverer 3.0 (CD) software for preliminary analysis. This included peak extraction, peak alignment, retention time correction, and extraction peak area determination. The identification of unknown compounds was performed by matching the fragment ions with the mzCloud database,1 mzVault database, and ChemSpider database.2 The results were further compared with relevant literature to ensure accurate identification of the chemical components in the SFTOT transdermal receiving solution.
Network pharmacology analysis
2.5
Screening of drug targets and collection of disease targets
2.5.1
All identified active compounds in Shufeitie ointment (SFTOT) capable of penetrating the skin were uploaded to the SwissTargetPrediction,3 PharmMapper,4 and SEA5 databases for target prediction. To maximize the number of potential targets, we integrated results from all three databases. We selected targets with Probability ≥ 0.2 in SwissTargetPrediction, NormFit ≥ 0.8 in PharmMapper, and MaxTc ≥ 0.4 in SEA. After compiling the data, we removed duplicate entries to establish the SFTOT target library. Next, we identified human target genes associated with Chronic Obstructive Pulmonary Disease (COPD) using the OMIM,6 DrugBank,7 and GeneCards8 databases, using “chronic obstructive pulmonary disease” as the search term. For GeneCards, we applied a GeneScore > 10 threshold to refine our selection. We compiled the retrieved data, removed duplicates, and established the COPD target library.
To standardize gene names, we used the UniProt database9 to convert SFTOT and COPD target names into their standardized gene forms. We then identified overlapping targets between the SFTOT target library and the COPD target library, clarifying the interaction between prescription-related and disease-related targets. This intersection formed the final target library, representing potential SFTOT targets for COPD treatment.
Constructing protein–protein interaction networks
2.5.2
The SFTOT-COPD intersection targets identified in section 2.5.1 were uploaded to the STRING database.10 We selected Homo sapiens as the biological species and set the minimum required interaction score to medium confidence (0.4). All other parameters were kept at their default settings. After screening the targets, we excluded unrelated ones, exported the data as a TSV file, and constructed the PPI network using Cytoscape (version 3.7.1) software to predict interactions between the targets. To analyze network topology, we employed the CytoNAC plug-in to calculate the closeness centrality (CC) and betweenness centrality (BC) of each node. Based on these results, we selected the key targets.
Gene ontology and Kyoto encyclopedia of genes and genomes signaling pathway enrichment analysis
2.5.3
To further explore the mechanism of SFTOT, we imported the selected SFTOT-COPD intersection targets into the DAVID database11 and restricted the target gene list to human genes. We performed GO biological function enrichment analysis and KEGG pathway enrichment analysis (21). GO analysis was divided into three categories: cellular component (CC), biological process (BP), and molecular function (MF). We sorted the results by p-value and visualized the top 10 GO terms and top 20 KEGG pathways as bubble plots.
Construction of the component-target-pathway network model
2.5.4
The SFTOT-COPD intersection targets enriched through KEGG analysis in section 2.5.3 and the SFTOT-COPD targets identified in section 2.5.1 were uploaded to Cytoscape 3.7.112 to construct a component-target-pathway network. We calculated network topology parameters and identified the key active components of SFTOT involved in COPD intervention based on these parameters and relevant literature.
Molecular docking
2.6
We obtained the three-dimensional crystal structure of potential targets from the RCSB PDB database13 and saved them in PDB format. The three-dimensional structures of active compounds were retrieved from PubChem, saved as SDF files, and converted to PDB format using Open Babel 2.4.1 (22). We imported the PDB files of target proteins and active compounds into AutoDock 1.5.714 for preprocessing, including water removal and hydrogenation. We designated the target protein as the receptor and the active compound as the ligand. Using the receptor protein’s grid box coordinates and size, we performed molecular docking to generate receptor-ligand binding results. This allowed us to calculate binding energy values, which we used to assess the stability of interactions between active components and potential targets, as well as to validate the reliability of the network pharmacology predictions. We visualized the docking results using LigPlot software.
Results
3
Qualitative study of Shufeitie ointment chemical constituents in transdermal permeation via UHPLC-Q-Orbitrap/MS
3.1
To investigate the active components of SFTOT against Chronic Obstructive Pulmonary Disease (COPD), we obtained the transdermal receiving solution using a Franz diffusion cell. We rapidly separated and analyzed the compounds using UHPLC-Q-Orbitrap/MS technology. The scanning mode used was Full scan/data-dependent secondary scan (Full MS/dd MS^2^). The total ion chromatogram of the transdermal components of SFTOT, analyzed in both positive and negative ion modes, is shown in Figures 1, 2.
SFTOT transdermal component positive ion pattern.
SFTOT transdermal component negative ion pattern.
Using the high-resolution mass spectrometry data, we derived possible molecular formulas, ensuring that the mass spectrometry deviation remained within 5 × 10^−6^. With the assistance of Compound Discoverer 3.0 software and the unknown identification database, we rapidly identified the target compounds. This identification was based on accurate relative molecular mass, secondary mass spectrometry fragmentation patterns, and corroborated with both domestic and international literature. Ultimately, we characterized a total of 129 chemical components, including: 12 components from JieZi (JZ), 18 components from CuYuanHua (CYH), 20 components from CuYanHuSuo (CYHS), 19 components from GanJiang (GJ), 14 components from XiXin (XX), 11 components from RouGui (RG), 23 components from JiaoMu (JM), and 12 common components from various traditional Chinese medicines. The names, molecular formulas, and secondary fragments of these compounds are listed in Table 1. These compounds are considered the active ingredients of SFTOT, which may exert pharmacological effects through the skin.
Analysis of the fragmentation pattern of flavonoids components
3.1.1
Flavonoids are key active ingredients in SFTOT. Using UHPLC-Q-Orbitrap/MS, we identified 11 flavonoids in the SFTOT transdermal receiving solution, including: 7-O-Methylluteolin, Genkwanin, Jaranol, Luteolin 7-O-glucoside, Luteolin, Quercetin, Apigenin, Quercitrin, Isoquercetin, Syringaldehyde, Dihydromelilotoside, Naringenin, Astragalin, and Kaempferol. These flavonoids are primarily derived from CYH. The primary fragmentation modes of flavonoids under high-energy collision in mass spectrometry are RDA fragmentation and the loss of neutral ions, such as CO_2_. Taking Luteolin, found in CYH, as an example, we speculated its fragmentation pattern. The excimer ion peak of the compound appeared at m/z 285.0405 [M-H]^−^. The parent ion undergoes RDA cleavage, producing the fragment ions at m/z 151.0039 and m/z 133.0297. The A-ring loses C_3_O_2_, generating the characteristic ion fragment at m/z 217.0512 [M-H-C3O2]^−^, while the C-ring loses CO and O, resulting in the characteristic ion fragment at m/z 241.0508. Based on the ion fragment data and literature (23), we identified the compound as Luteolin, and its fragment ions and potential cleavage pathways are shown in Figure 3.
Inference of fragmentation pathway of luteolin quality spectrum.
Analysis of the fragmentation pattern of alkaloid components
3.1.2
Alkaloids are a crucial class of natural compounds with diverse biological activities, including anti-inflammatory, analgesic, antioxidant, and nervous system-regulating properties. In this study, we identified 21 alkaloids in the SFTOT transdermal receiving solution, primarily derived from CYHS. Under high-energy collision in mass spectrometry, alkaloids typically undergo RDA fragmentation and the loss of CH₃, among other pathways. Using tetrahydropalmatine, found in CYHS, as an example, we analyzed its fragmentation pattern. The quasi-molecular ion peak appeared at m/z 356.1859 [M + H]^+^. The loss of a CH₃ group generated a fragment at m/z 341.1624 [M + H-CH₃]^+^. The parent nucleus then underwent RDA cleavage, producing complementary fragment ions at m/z 192.1020 and m/z 165.0912. Based on ion fragment data and literature reports (24), we identified the compound as tetrahydropalmatine. Its fragment ions and potential cleavage pathway are illustrated in Figure 4.
Inference of fragmentation pathway of tetrahydropalmatine quality spectrum.
Analysis of the fragmentation pattern of gingerol components
3.1.3
In this study, we identified 11 gingerol compounds in the SFTOT transdermal receiving solution, all derived from dried ginger. These compounds are characteristic constituents of GJ, sharing a 3-methoxy-4-hydroxyphenyl or a structurally similar parent nucleus. Gingerols exhibit a stronger response in positive ion mode. Under high-energy collision in mass spectrometry, gingerols primarily fragment through the loss of hydroxyl groups from the benzene ring, forming corresponding fragment ions. The side chain cleavage generates characteristic fragments, including m/z 177 (C₁₀H₁₃O₂), m/z 137 (C₈H₉O₂), and small neutral molecules such as CH₃(CH₂)_n_CHO and CH₃COOH, which are readily eliminated. Using 6-Gingerol as an example, we analyzed its fragmentation pattern. The quasi-molecular ion peak appeared at m/z 293.1763 [M-H]^−^. Under high-energy collisions, the main secondary fragment ions included m/z 236.1053, m/z 221.1545, and m/z 177.0927, corresponding to [M-H-C₄H₉]^−^, [M-H-C₅H₁₂]^−^, and [M-H-C₇H₁₆O]^−^, respectively. Based on ion fragment data and literature reports (25), we identified the compound as 6-Gingerol. Its fragment ions and potential cleavage pathway are illustrated in Figure 5.
Inference of fragmentation pathway of 6-gingerol quality spectrum.
Network pharmacology study based on Shufeitie ointment transdermal components
3.2
Construction of the component-disease database of potential targets
3.2.1
To further explore the potential gene targets of SFTOT in Chronic Obstructive Pulmonary Disease (COPD), we used the SwissTargetPrediction, PharmMapper, and SEA databases to predict targets for the 129 transdermal compounds identified through LC–MS analysis. After removing duplicates and performing UniProt correction, we obtained 806 active ingredient targets. Simultaneously, we searched for COPD-related disease targets in the GeneCards, DrugBank, and OMIM databases using COPD as the keyword. After eliminating duplicates and applying UniProt correction, we identified 1,500 human genes associated with COPD. We then intersected the active ingredient targets with the COPD disease targets, resulting in 222 intersection targets. These targets form the SFTOT target database for the treatment of COPD, and a Venn diagram illustrating the intersection is shown in Figure 6.
Venn plot of the intersection between SFTOT and COPD targets.
Protein–protein interaction network analysis of potential active ingredients
3.2.2
The 222 intersection targets were imported into STRING, and a PPI network was constructed using Cytoscape to explore the relationships between the targets. The PPI network revealed a total of 3,927 edges, indicating 3,927 interaction relationships between the proteins. In the network, the Degree value of a node represents the number of connections it has. By examining the Degree value, we identified proteins or molecules that are highly involved in these interactions. We used the CytoNCA plug-in to calculate the network’s topology features and performed two rounds of screening to identify the core targets. The first round used a Degree > 2 times the median, and the second round incorporated Degree, BC, and CC > median. As a result, we identified 17 potential core targets, and the screening process is shown in Figure 7.
Core target screening process diagram.
The potential core targets of SFTOT are visually represented in the network, with color and size variations reflecting their degree value. Deeper node colors and larger node sizes indicate higher interaction, while lighter colors and smaller sizes suggest fewer interactions (Figure 8). We focused on the top five targets in the PPI core target network: Tumor necrosis factor (TNF), Albumin (ALB), AKT Serine/Threonine Kinase 1 (AKT1), Epidermal Growth Factor Receptor (EGFR), and Caspase-3 (CASP3). These targets exhibited significant connectivity with other proteins and may represent key targets for the candidate compounds in COPD treatment. Therefore, we selected these five targets for molecular docking verification.
The core targets analyzed by PPI network.
GO and KEGG signaling pathway enrichment analysis
3.2.3
We conducted GO and KEGG analyses of the intersection targets using the DAVID database to identify the molecular functions and signaling pathways regulated by SFTOT. The GO enrichment analysis identified 838 Biological process (BP), 113 cellular component (CC), and 195 Molecular function (MF) with significant relevance. The KEGG pathway analysis revealed 187 significant pathways. The top 20 pathways from KEGG and the top 10 from GO enrichment are presented in bubble plots (Figures 9, 10). In these plots, the ordinate represents the enriched terms, while the abscissa shows the gene ratio for each term. The size of the bubble corresponds to the number of enriched genes, and the color intensity reflects the significance of the enrichment.
KEGG enrichment analysis of skinpermeable components of SFTOT against COPD (top 20 were listed).
GO enrichment analysis of skinpermeable components of SFTOT against COPD (top 10 were listed). BP, biological process; CC, cellular component; MF, molecular function.
Through GO functional enrichment analysis and KEGG analyses, we predicted that SFTOT regulates several key biological components. These include BP such as response to hypoxia, inflammatory response, and the positive regulation of MAP kinase activity and protein phosphorylation. CC include membrane rafts, receptor complexes, and extracellular exosomes; along with endopeptidase activity, protein serine/threonine/tyrosine kinase activity, protein binding and other MF. Furthermore, SFTOT appears to regulate important signaling pathways such as the Advanced Glycation End-products - Receptor for Advanced Glycation End-products (AGE-RAGE), TNF, PI3K/protein kinase B (Akt) signal transduction pathway (PI3K-Akt), and mitogen-activated protein kinase (MAPK) pathways, which may contribute to its therapeutic effects in COPD.
Component-target-pathway network model
3.2.4
We used Cytoscape 3.7.1 software to construct and analyze the relationship network between the potential active components and targets of SFTOT, resulting in a network diagram with 377 nodes and 3,083 edges. In the diagram, nodes of different colors represent the active components from different drugs (Figure 11). Based on the Degree value and relevant literature, we identified the following as core active ingredients: luteolin, kaempferol, quercetin, 7-O-methylluteolin, apigenin, ferulic acid, palmitic acid, sinapic acid, shogaol, and myristic acid. Among these, Luteolin, quercetin, hydroxygenkwanin, and apigenin are derived from CuYuanHua (CYH). Ferulic acid and myristic acid are from XiXin (XX), while kaempferol and palmitic acid are common to both XX and CYH. Sinapic acid is found in JieZi (JZ), and 6-shogaol originates from GanJiang (GJ). These findings suggest that the core Chinese medicines contributing to SFTOT’s therapeutic effects in this study are CYH, XX, JZ, and GJ. Furthermore, these 10 components play a crucial role in the treatment of COPD.
“Component-target-pathway” network model (The hexagon is the component, the blue diamond is the target, and the red inverted triangle is the pathway).
Molecular docking based on network pharmacology
3.3
Based on the previous data, we identified the intersection targets and main active components of Shufeitie ointment (SFTOT) in the treatment of Chronic Obstructive Pulmonary Disease (COPD). To explore the key signaling molecules involved, we conducted molecular docking to investigate the interaction between the active components and core targets. AutoDock software was employed for pairwise molecular docking between the 10 selected active components and the five top core targets. The binding free energy was used to evaluate the affinity between the active ingredient (ligand) and the core target receptor. A binding energy of <0 indicates that the ligand and receptor can bind spontaneously. When the binding energy is < −5.0 kcal/mol, it suggests that the ligand and receptor are well docked (26), while a docking energy < −7 kcal/mol indicates a strong binding effect. The docking results are shown in Figure 12. The results with lower binding energy were visualized to show the receptor-ligand complex model. Figure 13 highlights the optimal binding site of the ligand small molecules with the receptor protein. Among the 50 receptor-ligand docking groups, 36 exhibited binding energies < −5.0 kcal/mol, accounting for 72%. This indicates that the core components demonstrated strong binding activity with the core targets. The highest docking score was observed for the interaction between Epidermal growth factor receptor (EGFR) and apigenin, with a binding energy of −7.58 kcal/mol. Apigenin, derived from CuYuanHua (CYH), also exhibited stronger binding with the other core targets compared to the other components. These findings suggest that apigenin is a key component in the therapeutic action of SFTOT. These docking results provide valuable data for further optimization of the SFTOT prescription and dosage forms in future research.
Molecular docking binding energy heat map of targets and active ingredients.
SFTOT core components are interconnected with molecules of core targets. (A) Apigenin and TNF. (B) 7-O-Methylluteolin and ALB. (C) Luteolin and ALB. (D) Luteolin and EGFR. (E) Quercetin and CASP3. (F) Kaempferol and AKT1.
Discussion
4
Chronic Obstructive Pulmonary Disease (COPD) is primarily characterized by persistent inflammation of the airways, pulmonary vessels, and lung parenchyma. Its pathogenesis is associated with an imbalance between oxidative stress and antioxidant defenses (2). Although previous studies have demonstrated the significant efficacy of Shufeitie ointment (SFTOT) in treating COPD, its pharmacodynamic components and specific mechanisms of action remain insufficiently understood. Therefore, this study aims to explore the pharmacodynamic basis and mechanisms through which SFTOT exerts its therapeutic effects in COPD, thereby enhancing our understanding of its clinical benefits.
In this study, UHPLC-Q-Orbitrap/MS technology was used to identify the transdermal permeation components of SFTOT. Firstly, the chromatographic conditions were investigated. Referring to the liquid chromatography conditions, combined with the differences of high performance liquid chromatography columns and the characteristics of mass spectrometry, 0.1% formic acid water (A)-acetonitrile (B) was selected as the mobile phase, the column temperature was 40°C, and the flow rate was 0.2 mL/min. The HPLC chromatographic gradient was tried first, and the time was shortened on the basis of the original gradient. It was found that the samples were completely eluted before 18 min and the peak time was compact, concentrated between 12–18 min. Therefore, the gradient was changed, and the chromatographic conditions were finally determined to achieve ideal separation efficiency and single peak width. Full Scan/dd-MS^2^ (full scan + automatic trigger secondary) was used as the scanning mode in the mass spectrometry. Through one injection, high-quality primary and secondary mass spectrometry data can be obtained simultaneously for qualitative results. According to the mass of the chemical constituents of the single herb reported in the literature, the scanning range m/z 70 ~ 1,050 was selected. After preliminary analysis by high performance liquid chromatography separation and mass spectrometry scanning in positive and negative ion modes, the response intensity of each component in positive and negative ion modes was significantly different. According to the physical and chemical properties of each component combined with its mass spectrometry response in different scanning modes, the ion mode with the best response was finally selected as the analysis condition, so that each analyte had a good response value and peak shape, which could meet the rapid and accurate qualitative requirements. This study shows that UHPLC-Q-Orbitrap / MS combined with Compound Discover 3.0 analysis software can achieve a simple and rapid structural identification of the chemical constituents of SFTOT. UHPLC-Q-Orbitrap/MS can realize the separation of unknown compounds in the preparation, complete the high-throughput workflow, and the determination of compounds is not limited by quantity. It can collect more comprehensive compound information, and can quickly and accurately screen and qualitatively analyze low-content potential compounds in complex systems.
The in vitro transdermal experiment is a method used to assess the skin penetration properties of drugs, employing isolated skin (animal, human, or artificial) in combination with specific analytical techniques. Several critical factors influence the experimental outcomes, including the choice of skin type, determination of the receiving medium, dosage settings, and control of the simulated temperature. In this experiment, we selected nude mouse skin based on its characteristics and suitability for the study. In choosing the receiving medium, we took into account the physical and chemical properties of the target drug, the biocompatibility of the medium with the skin, and its potential impact on skin barrier function. Previous studies have reported that a mixture of normal saline and varying concentrations of ethanol is commonly used as a transdermal receiving solution (27, 28). While ethanol can significantly enhance the transdermal rate and amount of non-water-soluble drugs, it may also over-accelerate drug permeation, leading to an inappropriate increase in the amount or rate of drug penetration. Moreover, the permeability of nude mouse skin is superior to that of human skin, further complicating the interpretation of results. Therefore, in this experiment, normal saline was selected as the transdermal receiving medium to avoid the potential over-enhancement caused by ethanol. To ensure appropriate drug delivery, we adhered to the principle of moderate dosing. If the dosage were too small, the drug could penetrate the skin completely before the end of the experiment. Conversely, if the dosage were excessive, uneven distribution and excessive residues could occur. Therefore, 1 g of SFTOT was chosen for use in this experiment. Additionally, since the skin surface temperature typically ranges around 32°C, we strictly controlled the water bath temperature to maintain a consistent range of (32 ± 1) °C to ensure the accuracy of experimental conditions.
In a transdermal drug delivery system, molecular weight and lipophilicity are critical factors that influence transdermal absorption efficiency. Drugs penetrate the skin via the intercellular space; however, when the molecular weight is too large, transmission resistance increases, and the drug is retained within the skin. It is generally accepted that drugs with a molecular weight of less than 500 Dalton (Da) have greater potential for efficient skin penetration (29). This study revealed that the molecular weight of the chemical components detected in the SFTOT transdermal receiving solution predominantly ranged from 80 to 470 Da, with over 95.3% of the components having a molecular weight below 400 Da. These characteristics suggest that the components exhibit excellent transdermal properties and can efficiently penetrate the skin barrier. Utilizing UHPLC-Q-Orbitrap/MS technology, we successfully identified 129 effective transdermal permeation components in SFTOT, providing crucial data for further investigation into the material basis and mechanism of SFTOT’s effects.
Among the 129 transdermal components, the network pharmacology and molecular docking analyses identified Luteolin, Kaempferol, Quercetin, 7-O-Methylluteolin, Apigenin, Ferulic acid, Palmitic acid, Sinapic acid, Shogaol, and Myristic acid as the core active compounds. These substances are the primary contributors to SFTOT’s therapeutic effects in treating COPD. They are mainly derived from CuYuanHua (CYH), XiXin (XX), JieZi (JZ), and GanJiang (GJ). Previous studies have demonstrated that these core active components possess various pharmacological effects relevant to COPD treatment. For example, Luteolin has been shown to inhibit macrophage phosphorylation and down-regulate pro-inflammatory factors, including interleukin-6 and tumor necrosis factor-α (30). Quercetin can significantly improve lung function in pulmonary fibrosis models by enhancing cell viability, reducing the production of inflammatory cytokines Tumor Necrosis Factor-alpha (TNF-α), Interleukin-6 (IL-6), Interleukin-8 (IL-8), and inhibiting apoptosis (31). Additionally, XiXin decoction can effectively reduce inflammatory ear swelling in mice (32), and Sinapic acid exerts anti-inflammatory effects by inhibiting the cyclooxygenase-2 and Nuclear Factor Kappa-light-chain-enhancer of Activated B cells (NF-κB) signaling pathways (33). Furthermore, Gingerol, derived from GJ, has been shown to reduce lung tissue injury by inhibiting the activation of the NF-κB pathway and to improve alveolar coagulation and fibrinolysis in rats with acute respiratory distress syndrome induced by lipopolysaccharide (34). The research presented above demonstrates that SFTOT contains various effective components that alleviate cough and asthma-related diseases by reducing the inflammatory response. These findings offer significant insight for further investigation into SFTOT’s therapeutic potential.
Protein–protein interaction (PPI) network analysis further suggests that SFTOT may exert its therapeutic effects in COPD through key targets, including Tumor necrosis factor (TNF), Albumin.
(ALB), AKT Serine/Threonine Kinase 1(AKT1), Epidermal Growth Factor Receptor (EGFR), and Caspase-3 (CASP3). TNF-α, a small molecule protein secreted by macrophages, plays a critical role in both the local and systemic inflammatory responses associated with COPD. Elevated levels of TNF-α in COPD patients exacerbate inflammation and damage alveolar epithelial cells (35), making it a crucial mediator in the regulation of COPD inflammation. ALB, the most abundant protein in human plasma, is often found at decreased levels in COPD patients, reflecting a disruption in its normal function during the disease (36). AKT1, a member of the AGC protein kinase family, is integral in regulating cell growth, division, and apoptosis inhibition. Its multifaceted role may influence the cellular mechanisms central to the pathological processes of COPD (37). EGFR, a key regulator of cellular activities, is associated with increased airway mucus secretion. SFTOT may help reduce airway mucus hypersecretion in COPD by modulating EGFR expression (38). CASP3, involved in the regulation of airway smooth muscle cell apoptosis through the Polo-like Kinase 1 - Caspase-3 (PLK1-CASP3) pathway, is another vital target for COPD treatment (39).
To further elucidate the underlying mechanisms of SFTOT, Kyoto Encyclopedia of Genes and Genomes (KEGG) pathway enrichment analysis was conducted on the component-disease intersection targets. The results of the analysis were primarily enriched in key signaling pathways, including Advanced Glycation End-products - Receptor for Advanced Glycation End-products (AGE-RAGE), TNF, PI3K/protein kinase B (Akt) signal transduction pathway (PI3K-Akt), and mitogen-activated protein kinase (MAPK). Among these, RAGE, TNF, and the MAPK signaling pathways are closely associated with the inflammatory response and oxidative stress (40–42). The PI3K-Akt pathway, a crucial intracellular signaling cascade, regulates various cellular biological processes and the cell cycle. By influencing downstream effector molecules involved in apoptosis, transcription, translation, metabolism, and angiogenesis, the PI3K-Akt pathway plays a pivotal role in COPD airway remodeling (43, 44). These findings suggest that SFTOT may exert its therapeutic effects through the modulation of multiple signaling pathways, offering a novel perspective and potential strategy for COPD treatment.
Conclusion
5
Research on the material basis of Traditional Chinese Medicine (TCM) compounds is essential for ensuring quality control and safety, playing a key role in the modernization of TCM. In this study, Shufeitie ointment (SFTOT) was selected as the research object. Using the high sensitivity and precision of liquid chromatography-mass spectrometry (LC–MS), we conducted the first qualitative analysis of the transdermal permeation components, identifying the chemical constituents. This laid a solid scientific foundation for subsequent formulation optimization and comprehensive quality control research. Additionally, by employing network pharmacology and molecular docking techniques, we made the first molecular-level predictions of the pharmacodynamic mechanisms of SFTOT. We also identified key quality markers associated with its efficacy, providing valuable insights for improving the quality standards of SFTOT.
However, due to the complexity of traditional Chinese medicine’s chemical composition, several limitations exist in this study. These include the inability to identify isomers and potentially new components generated in the prescription. While we employed high-resolution LC–MS, the analysis did not cover volatile components. Although we performed preliminary molecular docking validation, experimental verification is still lacking. As a result, some discrepancies between the predicted results and the actual outcomes may exist. Addressing these limitations, we plan to conduct further research in the future to fill these gaps and refine the findings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fortis S Georgopoulos D Tzanakis N Sciurba F Zabner J Comellas AP. Chronic obstructive pulmonary disease (copd) and copd-like phenotypes. Front Med (Lausanne). (2024) 11:1375457. doi: 10.3389/fmed.2024.1375457, PMID: 38654838 PMC 11037247 · doi ↗ · pubmed ↗
- 2Luo M Tang Y Qiu J Yang K Dai W Fang E. Proteomic insights into copd pathogenesis and therapeutic targets: a causal analysis of circulating proteins. Front Med (Lausanne). (2025) 12:1529495. doi: 10.3389/fmed.2025.1529495, PMID: 40421300 PMC 12104083 · doi ↗ · pubmed ↗
- 3Agusti A Celli BR Criner GJ Halpin D Anzueto A Barnes P. Global initiative for chronic obstructive lung disease 2023 report: gold executive summary. Am J Respir Crit Care Med. (2023) 207:819–837. doi: 10.1164/rccm.202301-0106 PP, PMID: 36856433 PMC 10111975 · doi ↗ · pubmed ↗
- 4Safiri S Carson-Chahhoud K Noori M Nejadghaderi SA Sullman M Ahmadian HJ. Burden of chronic obstructive pulmonary disease and its attributable risk factors in 204 countries and territories, 1990-2019: results from the global burden of disease study 2019. BMJ. (2022) 378:e 69679. doi: 10.1136/bmj-2021-069679 PMC 932684335896191 · doi ↗ · pubmed ↗
- 5Tangedal S Nielsen R Aanerud M Drengenes C Husebo GR Lehmann S. Lower airway microbiota in copd and healthy controls. Thorax. (2024) 79:219–226. doi: 10.1136/thorax-2023-220455, PMID: 38331579 · doi ↗ · pubmed ↗
- 6Zhao J Wu B Luan X Jiang Q Fang Y Liu X. Intervention effect of compound traditional Chinese medicine liuwei buqi decoction in treatment of COPD based on network pharmacology and animal experiments. J Hainan Med Univ. (2024) 30:1–16. doi: 10.13210/j.cnki.jhmu.20241126.002 · doi ↗
- 7Wei L Hongping H Chufang L Cuomu M Jintao L Kaiyin C. Effects of shiwei longdanhua formula on lps induced airway mucus hypersecretion, cough hypersensitivity, oxidative stress and pulmonary inflammation. Biomed Pharmacother. (2023) 163:114793. doi: 10.1016/j.biopha.2023.114793, PMID: 37121151 · doi ↗ · pubmed ↗
- 8Chen Y Gong X Zhou M Xu Y Fan F Xiao J. Treatment with jianpiyifei ii granules for patients with moderate to very severe chronic obstructive pulmonary disease: a 52-week randomised, double-blinded, placebo-controlled, multicentre trial. Phytomedicine. (2022) 100:154057. doi: 10.1016/j.phymed.2022.154057, PMID: 35349835 · doi ↗ · pubmed ↗