The effect of remimazolam and propofol on post-hysteroscopy sleep quality under general anesthesia: a post hoc analysis
Chen Yang, Le Zhang, Yan Cheng, Jianying Hu, Yuyan Nie, Shen Sun, Shaoqiang Huang

TL;DR
This study compared remimazolam and propofol for sleep quality and fatigue after hysteroscopy surgery, finding remimazolam may reduce mental fatigue on the first day.
Contribution
The study is the first to compare remimazolam and propofol's effects on postoperative sleep and fatigue using specific sleep and fatigue scales.
Findings
Patients in the propofol group had more awakenings and poorer sleep quality on the first postoperative day.
The propofol group showed higher fatigue, particularly mental fatigue, on the first postoperative day.
No significant differences were found in overall sleep quality scores (AIS) between the two groups.
Abstract
This post hoc analysis trial compared the impacts of remimazolam and propofol anesthesia on sleep quality and fatigue after hysteroscopic surgery. The post hoc analysis excluded patients with a Pittsburgh Sleep Quality Index (PSQI) score >15 or incomplete data. Preoperative PSQI scores were compared between patients receiving remimazolam and propofol. Intraoperative monitoring was conducted using the Modified Observer’s Assessment of Alertness/Sedation (MOAA/S) scale. Postoperative sleep and fatigue were assessed using the Athens Insomnia Scale (AIS) and Fatigue Scale-14 (FS-14) via WeChat questionnaires on the first and second postoperative days. Fifteen patients were included in this post hoc analysis. No significant differences were observed in AIS scores on postoperative days 1 and 2. Compared to the remimazolam group, patients in the propofol group experienced more awakenings (1…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
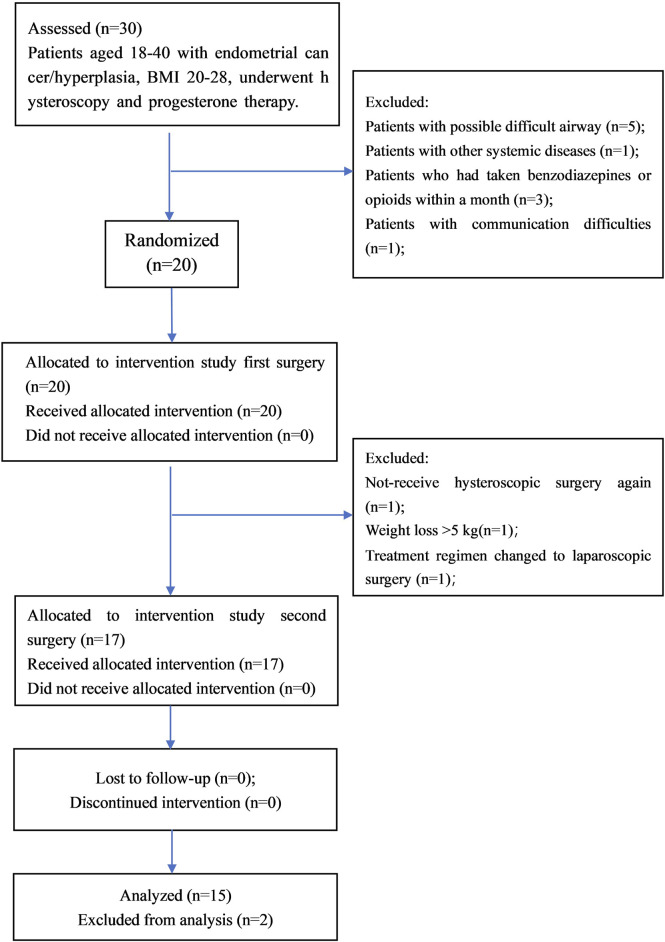 FIGURE 1
FIGURE 1| Time points | MAP | HR | ||
|---|---|---|---|---|
| Remimazolam | Propofol | Remimazolam | Propofol | |
| T0 | 95.3 ± 12.7 | 97.5 ± 11.4 | 71.1 ± 12.2 | 71.6 ± 8.9 |
| T1 | 88.9 ± 10.1 | 88.4 ± 10.6 | 72.6 ± 12.1 | 71.3 ± 12.5 |
| T2 | 86.4 ± 13.4 | 85.7 ± 8.9* | 73.5 ± 15.3# | 64.2 ± 12.9* |
| T3 | 88.1 ± 13.1 | 84.2 ± 10.5* | 72.0 ± 12.9# | 66.2 ± 10.7* |
| T4 | 88.7 ± 9.1 | 87.1 ± 10.7 | 69.7 ± 14.2# | 61.3 ± 13.2* |
| Questionnaire content | Postoperative day 1 | Postoperative day 2 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Remimazolam | Propofol | Mean difference | 95% CI of the difference | P | Remimazolam | Propofol | Mean difference | 95% CI of the difference | P | |
| Insomnia scoring | 4 (1.5) | 4 (2.6) | 0.40 | (-1.42, 0.62) | 0.219 | 2 (1.3) | 2 (1.4) | 0.78 | (-2.86, 0.39) | 0.121 |
| Time taken to fall asleep | 0 (0.1) | 0 (0.1) | 0.02 | (-0.13, 0.38) | 0.568 | 0 (0.1) | 0 (0.1) | 0.04 | (-0.32, 0.56) | 0.562 |
| Night time awakenings | 1 (0.2) | 2 (1.3) | 0.34 | (-0.03, 0.58) | 0.029 | 0 (0.2) | 1 (0.2) | 0.25 | (-0.11, 0.67) | 0.063 |
| Waking up earlier than desired | 0 (0.1) | 0 (0.2) | 0.09 | (-0.23, 0.31) | 0.073 | 0 (0.1) | 0 (0.1) | 0.06 | (-0.13, 0.31) | 0.343 |
| Total sleep duration | 1 (1.2) | 1 (0.2) | 0.05 | (-0.12, 0.11) | 0.121 | 1 (0.2) | 1 (0.1) | 0.14 | (-0.25, 0.32) | 0.152 |
| Overall sleep quality | 1 (0.2) | 2 (1.2) | 0.07 | (-0.06, 0.10) | 0.043 | 1 (0.2) | 1 (1.2) | 0.20 | (-0.14, 0.55) | 0.078 |
| Daytime physical functions | 0 (0.1) | 0 (0.1) | 0.02 | (-0.09, 0.28) | 0.573 | 0 (0.1) | 0 (0.1) | 0.07 | (-0.12, 0.25) | 0.471 |
| Daytime mood | 0 (0.1) | 1 (0.1) | 0.12 | (-0.11, 0.35) | 0.073 | 0 (0.1) | 1 (0.1) | 0.12 | (-0.09, 0.68) | 0.067 |
| Daytime sleepiness | 0 (0.1) | 0 (0.1) | 0.08 | (-0.45, 0.24) | 0.452 | 0 (0.1) | 0 (0.1) | 0.06 | (-0.13, 0.27) | 0.473 |
| Questionnaire | Postoperative day 1 | Postoperative day 2 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Remimazolam | Propofol | Mean difference | 95% CI of the difference | P | Remimazolam | Propofol | Mean difference | 95% CI of the difference | P | |
| Fatigue Score | 3 (2.6) | 5 (3.8) | 0.51 | (0.13, 0.25) | 0.035 | 3 (1.6) | 4 (2.6) | 0.55 | (-0.59, 1.78) | 0.092 |
| Physical Fatigue | 3 (1.7) | 4 (2.8) | 0.27 | (-0.03, 1.28) | 0.052 | 3 (0.5) | 4 (1.6) | 0.66 | (0.16, 2.16) | 0.047 |
| Mental Fatigue | 1 (0.2) | 3 (2.4) | 0.65 | (0.36, 0.81) | 0.023 | 1 (0.2) | 1 (0.2) | 0.45 | (-0.64, 1.21) | 0.421 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAnesthesia and Sedative Agents · Intraoperative Neuromonitoring and Anesthetic Effects
1 Introduction
Postoperative Sleep Disorders (PSD) refer to a clinical syndrome characterized by reduced nighttime sleep duration, disrupted sleep structure, and abnormal circadian rhythms following surgery (Luo et al., 2020). Postoperative Fatigue Syndrome (POFS) is subjectively felt fatigue after surgery, manifesting as persistent tiredness, weakness, and decreased concentration (Rubin and Hotopf, 2002). Both are closely related and commonly occur after various surgeries, significantly reducing the quality of postoperative recovery (Su and Wang, 2018). Studies have shown that patients experience decreased postoperative sleep quality (Lei et al., 2017) and increased fatigue scores after propofol anesthesia (Li et al., 2018). In recent years, a safe and effective new benzodiazepine sedative, remimazolam, has been widely used for anesthesia induction and maintenance. Unlike propofol, remimazolam’s metabolites are inactive, and its effects can be reversed by flumazenil (Sneyd and Rigby-Jones, 2020; Kilpatrick, 2021).
In our hospital, young patients with endometrial cancer or complex hyperplasia, aiming to preserve fertility, undergo a treatment protocol involving hysteroscopic evaluation and resection combined with progestin therapy (Guan and Chen, 2022). We enrolled patients who underwent two hysteroscopies within a 3-month period, randomly assigning them to remimazolam or propofol anesthesia in a crossover study (Yang et al., 2024).
Given the scarcity of studies on the effects of remimazolam on postoperative sleep and fatigue, both domestically and internationally, the impact of remimazolam on these outcomes remains unclear. This study aims to address this knowledge gap by comparing the effects of remimazolam and propofol on postoperative sleep and fatigue in patients undergoing hysteroscopic surgery.This post hoc analysis trial compared the effects of remimazolam and propofol on the postoperative sleep and fatigue status of patients undergoing hysteroscopic surgery.
2 Methods
2.1 Design
This article documents a post hoc analysis of a previous single-blind, randomized crossover trial, which showed that BIS was higher and hemodynamic fluctuation was less in patients with ramazolam anesthesia compared with propofol anesthesia.Details on interventions can be found elsewhere (Yang et al., 2024). Briefly, the inclusion criteria were patients aged 18–40 years with a body mass index (BMI) of 20–28 kg/m^2^, scheduled for hysteroscopic evaluation and resection combined with progestin therapy for endometrial cancer or complex hyperplasia. On the day before surgery, After obtaining informed consent, the anesthesiologist responsible for the study added eligible patients to WeChat, distributed the Pittsburgh Sleep Quality Index (PSQI) questionnaire, (Zak et al., 2022), random numbers were generated using a random number generator software, and the pre-prepared sealed envelope marked with the corresponding number was opened, and patients were regimened according to the information inside the envelopes, marking the We Chat contacts with the regimen information. Depending on the anesthetic regimen for hysteroscopy, patients were randomly assigned to two regimens: one regimen received propofol first, followed by remimazolam anesthesia 3 months later; the other regimen was treated with remimazolam first, followed by propofol anesthesia 3 months later.
2.2 Samples and settings
Assuming a standard deviation of 10 for BIS values between groups when sedation scores are ≤1, and aiming to detect a mean BIS difference of ≥15, a paired t-test with α = 0.05 and power of 85% requires a sample size of 14. Given the 3-month study duration and an estimated attrition rate of 40%, we planned to enroll 20 patients.A total of 17 patients completed the randomized crossover study. In the post hoc analysis, the withdrawal criteria were those with PSQI >15 or incomplete postoperative data.
Upon admission to the operating room, routine non-invasive monitoring of blood pressure (Mean Arterial Pressure, MAP), heart rate (HR), and oxygen saturation (SPO2) was commenced. Anesthesia induction (T0) involved TCI pump-administered remifentanil (Ce 1.58 ng/mL). Concurrently, patients received either a slow injection of remimazolam (0.27 mg/kg over 30s, followed by a continuous infusion at 1 mg/kg/h followed by a continuous infusion at 1 mg/kg/h) or propofol (2.0 mg/kg over 30s, followed by a continuous infusion at 6 mg/kg/h). The Modified Observer’s Assessment of Alertness/Sedation Scale (MOAA/S) (Pastis et al., 2022) was assessed every minute after administration. T1 was recorded when MOAA/S fell below 2. T2, T3, and T4 marked the insertion of the laryngeal mask, the start of hysteroscopic cervical dilation, and surgery end, respectively. Patient awakening was denoted as T5. All patients were discharged on the same day,no postoperative analgesic protocol was implemented.
2.3 Data collection
Postoperatively, patients were surveyed at 8 a.m. on the first and second days via WeChat using the Athens Insomnia Scale (AIS) (Gómez-Benito et al., 2011) to assess sleep quality. The AIS includes eight items evaluating sleep onset, nocturnal awakenings, early morning awakening, total sleep time, overall sleep quality, daytime mood, daytime physical function (memory, cognitive ability, attention), and daytime somnolence. Each item is scored from 0 (none) to 3 (severe); a total score <4 indicates no sleep disturbance, 4–6 suggests possible insomnia, and >6 indicates sleep disturbance. The Fatigue Scale (FS-14) (Chalder et al., 1993) consisting of 14 items across two dimensions—physical and mental fatigue—was also administered. This binary scale scores from 0 to 1, with physical fatigue maxing at 8, mental fatigue at 6, and a total possible maximum of 14. A score ≥5 indicates fatigue syndrome. Intraoperative awareness was assessed on the first day postoperatively, and anesthesia satisfaction was evaluated on the second day postoperatively. Blinded anesthesia nurses recorded questionnaire data.
The primary outcome was AIS scores on the first postoperative day. Secondary outcomes included AIS scores on the second postoperative day and FS-14 scores on both the first and second postoperative days. Intraoperative hemodynamic data (MAP, HR, etc.) were re-evaluated.
2.4 Data analysis
Data analysis was conducted using SPSS 22.0. The Kolmogorov‒Smirnov test assessed univariate data distribution. Normal data are reported as mean ± standard deviation ( ± s). The paired-sample t-test compared regimens, with Bonferroni correction for intra-group comparisons, setting significance at P < 0.0125. Non-normal data are presented as median (interquartile range), with the paired rank sum test used for inter-regimen comparisons. Count data, expressed as rates, were analyzed using the chi-squared test, with P < 0.05 indicating significance.
2.5 Ethical considerations
The original study (Yang et al., 2024) had been approved by the University’s Institutional Review Board (IRB2022-134), and all patients had provided informed written consent. The original trial was registered at the Chinese Clinical Trial Registry (ChiCTR2200064551, Principal investigator: Chen Yang, https://www.chictr.org.cn/showproj.html?proj=177003, Date of registration: 2022/10/11).
3 Results
There were 17 patients in the crossover trial, two were excluded due to incomplete follow-up data. Consequently, the final analysis was conducted on 15 patients (Figure 1). Of the 15 patients, mean age was 34.4 ± 5.8 years; height, 163.5 ± 7.3 cm; weight, 63.5 ± 11.7 kg; post-three-month weight, 63.9 ± 12.3 kg, with no significant weight change (P = 0.67). Intraoperatively MAP and HR were assessed (Table 1). Remimazolam induced no significant changes in MAP and HR from baseline. Propofol led to significant changes in MAP at T2 and T3, and HR at T2, T3, and T4 vs. baseline (p < 0.0125). Comparing regimens remimazolam resulted in higher HR at T2, T3, and T4 than propofol (p < 0.05), with no significant MAP differences between regimens.
Flow chart.
Preoperative PSQI scores were similar between regimens: 4 (3–5) vs. 4 (3–6), p = 0.377. Surgical durations were comparable. Postoperative AIS scores on days 1 and 2 were not significantly different between regimens (Table 2). However, careful analysis of the contents of AIS score showed that on the first postoperative night, patients in the propofol regimen had more night time awakenings (1 [0, 2] versus 2 [1, 3], p = 0.029) and poorer sleep quality (1 [0, 2] versus 2 [1, 2], p = 0.043) compared those in remimazolam regimen.
FS-14 scores, detailed in Table 3 showed higher fatigue on the first day in the propofol regimen (5 [3, 8] versus 3 [2, 6], p = 0.035). Mental fatigue was lower in the remimazolam regimen than those in the propofol regimen (1 [0, 2] versus 3 [2, 4], p = 0.023). Physical fatigue on second postoperative day was also lower than those in the propofol regimen (3 [0, 5] versus 4 [1, 6], p = 0.047). There was no intraoperative awareness, and anesthesia satisfaction was similar for both regimens (9 [8–10] vs. 9 [8–10], p = 0.78).
4 Discussion
This post hoc analysis of previous single-blind, randomized crossover trial compared the effects of remimazolam and propofol on postoperative sleep and fatigue in patients undergoing hysteroscopic surgery. Additionally, physical fatigue scores were lower on postoperative day 2 in remimazolam regimen. However, no significant differences were observed in overall postoperative insomnia scores or anesthesia satisfaction between the regimens.
The study employed the PSQI scale to assess patients' sleep quality over the month preceding surgery. Considering that the PSQI may not accurately reflect short-term changes in sleep or the impact of specific events on sleep, (Zitser et al., 2022), the Athens Insomnia Self-report Questionnaire was used postoperatively to evaluate sleep changes more specifically, including nocturnal sleep patterns and daytime functioning. (Chung et al., 2011). Concurrently, the FS-14 scale was utilized to assess fatigue levels, offering a quantitative evaluation of both physical and mental fatigue with good internal consistency. (Nøstdahl et al., 2019). The study used WeChat push to collect postoperative 2-day scales. As patients were young women with a high acceptance of new media methods. WeChat is an effective way to build a communication platform between hospitals and patients. (Montag et al., 2018).
Sleep is a cyclical process, divided into NREM (non-rapid eye movement) sleep, typically constituting 75%–80% of the sleep cycle, and REM (rapid eye movement) sleep, characterized by heightened brain activity and dreaming. (Al et al., 2021). Compared with men, women experience unique physiological changes during puberty, pregnancy, the postpartum period, and perimenopause, which can predispose them to sleep disturbances. (Aksan and Dilbaz, 2024). Research has consistently demonstrated a higher prevalence of sleep disorders in women. (Van Someren, 2021). Postoperative sleep disturbances, including difficulty falling asleep, nighttime awakenings, and early morning awakenings, may arise from various factors such as surgical trauma, effects of anesthetic medications, pain, discomfort, and psychological stress. These disturbances can negatively impact patient recovery and rehabilitation. (Rosenberg-Adamsen et al., 1996). In this study, the majority of the participants were young women may further contribute to an increased risk of postoperative sleep disorders.
Numerous studies have shown that propofol disrupts the postoperative sleep-wake cycle by affecting melatonin secretion and the locus coeruleus-norepinephrine (LC-NE) system, leading to decreased sleep quality on the first postoperative day. (Li et al., 2018; Kushikata et al., 2016; Du et al., 2018). Additionally, propofol has been found to influence the levels of inflammatory mediators, such as IL-6 and IL-8, thereby affecting inflammatory pathways and contributing to the occurrence of postoperative sleep disturbances. (Sayed et al., 2015; Qiao et al., 2015). Propofol inhibits REM sleep but can prolong slow-wave sleep, increasing deep sleep duration. (Lewis et al., 2018). Benzodiazepines also alter sleep architecture by extending NREM sleep, which increases total sleep time but notably suppresses slow-wave and REM sleep. (de Mendonça et al., 2023). Intraperitoneal administration of midazolam in rats significantly increased NREM sleep after 6 h. (Lancel et al., 1997). The latest retrospective cohort study found that compared with propofol, remimazolam in elderly patients undergoing spinal surgery was associated with smaller changes in melatonin and cortisol concentrations. It is speculated that the smaller impact on sleep rhythm may help alleviate postoperative sleep disorders. (Yaqiu et al., 2025).
In elderly patients undergoing total joint arthroplasty, the use of remimazolam for intraoperative sedation did not significantly improve postoperative sleep quality as assessed by the Richards-Campbell Sleep Questionnaire (RCSQ). However, there was a slight increase in scores related to sleep recovery and overall sleep quality. (Deng et al., 2023). This study found no differences in overall postoperative AIS scores between the two regimens. The minor differences observed in the number of nocturnal awakenings and overall sleep quality may not be clinically significant, considering the mean differences and the range of the 95% confidence intervals.Despite using a randomized crossover method to minimize bias from population differences, considering the short duration of hysteroscopic surgery, averaging around 10 min with total anesthesia time not exceeding 20 min, it is unlikely to have a significant effect on postoperative insomnia index scores on the first and second days. The effects of longer surgeries warrant further investigation.
Previous studies have found that changes in HR after anesthesia reflect the excitability of the vagus nerve and the circulatory function of patients, and the low functional state of the cardiovascular system is significantly related to the occurrence of POFS (Yu et al., 2015). This study found smaller HR fluctuations after remimazolam induction compared to propofol, suggesting circulation stability in line with prior results (Ye et al., 2023). This might explain the lower fatigue scores on day 1 with remimazolam. Inflammatory responses are also tied to subjective postoperative fatigue (Späth-Schwalbe et al., 1998).
This study has some limitations. Firstly, it does not exclude the impact of opioid medications on postoperative sleep. Clinical reports indicate that although remifentanil does not inhibit nocturnal melatonin secretion, it significantly suppresses REM sleep in subjects (Cao and Javaheri, 2018; Cutrufello et al., 2020). The disruptive effect of opioids on sleep architecture is dose-dependent; however, for patients experiencing pain, the analgesic effect of opioids reduces awakenings during sleep and improves sleep efficiency (Kondili et al., 2012). Secondly, this study only involves data from 1 day before surgery to 2 days after surgery, monitoring short-term sleep and fatigue conditions in patients. Research shows that postoperative sleep-wake cycle disturbances are most evident from day 1 to day 2 after surgery and can persist until day 6 (van Zuylen et al., 2022). It remains unclear whether longer follow-up would yield positive findings. Lastly, this study used subjective scales widely employed both domestically and internationally. Although simple and practical, these scales are susceptible to emotional and environmental influences. Objective assessment methods, such as using sleep monitors for EEG readings, wearable devices like smartwatches to track physiological parameters, and software to evaluate task completion speed and accuracy, are potential options for obtaining objective evaluation indices. However, these methods have limitations, particularly in requiring specialized equipment. Given that patients in this study were not hospitalized, implementing monitoring within 2 days post-operation was challenging. Future applications of these methods may be more feasible in studies involving hospitalized patients.
5 Conclusion
This post hoc analysis trial compared the effects of remimazolam and propofol anesthesia on postoperative sleep and fatigue status in patients undergoing hysteroscopic surgery. Although no differences were observed in the AIS scores over two postoperative days, patients in the remimazolam regimen exhibited lower levels of fatigue on postoperative day 1, particularly in terms of mental fatigue. This suggests that remimazolam may enhance early postoperative recovery quality in short-duration surgeries, making it a preferable choice for accelerating postoperative recovery compared to propofol. Future research is warranted to further compare the effects of propofol and remimazolam on fatigue levels and multidimensional evaluations of postoperative sleep quality in longer surgical procedures.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Aksan A.Dilbaz B. (2024). Sleep disorders in women: what should a gynecologist know? Geburtshilfe Frauenheilkd 84 (11), 1043–1049. Published 2024 Aug 15. 10.1055/a-2371-0763 39524035 PMC 11543111 · doi ↗ · pubmed ↗
- 2Albqoor M. A.Shaheen A. M. (2021). Sleep quality, sleep latency, and sleep duration: a national comparative study of university students in Jordan. Sleep. Breath. 25 (2), 1147–1154. 10.1007/s 11325-020-02188-w 33034880 · doi ↗ · pubmed ↗
- 3Cao M.Javaheri S. (2018). Effects of chronic opioid use on sleep and wake. Sleep. Med. Clin. 13 (2), 271–281. 10.1016/j.jsmc.2018.02.002 29759277 · doi ↗ · pubmed ↗
- 4Chalder T.Berelowitz G.Pawlikowska T.Watts L.Wessely S.Wright D. (1993). Development of a fatigue scale. J. Psychosom. Res. 37 (2), 147–153. 10.1016/0022-3999(93)90081-p 8463991 · doi ↗ · pubmed ↗
- 5Chung K. F.Kan K. K.Yeung W. F. (2011). Assessing insomnia in adolescents: comparison of insomnia severity index, Athens insomnia scale and sleep quality index. Sleep. Med. 12 (5), 463–470. 10.1016/j.sleep.2010.09.019 21493134 · doi ↗ · pubmed ↗
- 6Cutrufello N. J.Ianus V. D.Rowley J. A. (2020). Opioids and sleep. Curr. Opin Pulm Med. 26 (6), 634–641. 10.1097/MCP.0000000000000733 32925368 · doi ↗ · pubmed ↗
- 7de Mendonça F. M. R.de Mendonça GPRR Souza L. C.Galvão L. P.Paiva H. S.de Azevedo Marques Périco C. (2023). Benzodiazepines and sleep architecture: a systematic review. CNS Neurol. Disord. Drug Targets 22 (2), 172–179. 10.2174/1871527320666210618103344 34145997 · doi ↗ · pubmed ↗
- 8Deng C. M.Meng Z. T.Yang J.Zhang C. J.Lu M.Wang Y. X. (2023). Effect of intraoperative remimazolam on postoperative sleep quality in elderly patients after total joint arthroplasty: a randomized control trial. J. Anesth. 37 (4), 511–521. 10.1007/s 00540-023-03193-5 37055671 PMC 10390348 · doi ↗ · pubmed ↗