A Study of Clinical Profile and Factors Affecting Mortality in Patients With Acute-on-Chronic Liver Failure in a Tertiary Care Hospital in Nepal
Pradip Kumar Kafle, Anurag Jha, Brindeswari Kafle Bhandari, Rabin Hamal, Tshering W Sherpa, Dinesh Koirala, Tulsiram Bhattarai, Manoj Lamsal, Sushil Parajuli, Rahul Pathak

TL;DR
This study examines factors affecting mortality in patients with acute-on-chronic liver failure in Nepal, finding that multiple predictors at admission can improve patient outcome predictions.
Contribution
The study evaluates the effectiveness of various severity scores and biochemical parameters in predicting mortality in ACLF patients within a Nepalese context.
Findings
The overall mortality rate was 56.9% among ACLF patients.
The CLIF-C ACLF score showed the highest predictive accuracy (AUC: 0.990) for mortality.
Multivariate analysis did not identify a single independent predictor of mortality.
Abstract
Background and aim Acute-on-chronic liver failure (ACLF) is a dynamic condition with very high short-term mortality. Although several mortality predictors have been studied, no single factor can reliably predict its course and outcome. This study aimed to evaluate various biochemical parameters and severity scores at presentation to assess their ability to predict mortality in ACLF patients. Methods An observational cross-sectional study was conducted from March 2024 to February 2025 at a tertiary care center in Nepal. A total of 51 patients were enrolled over one year. ACLF was diagnosed based on the Asia-Pacific Association for the Study of the Liver (APASL) criteria and/or the European Association for the Study of the Liver-Chronic Liver Failure Consortium (EASL-CLIF) criteria. Clinical features, biochemical parameters, and severity scores at admission were analyzed. Results The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
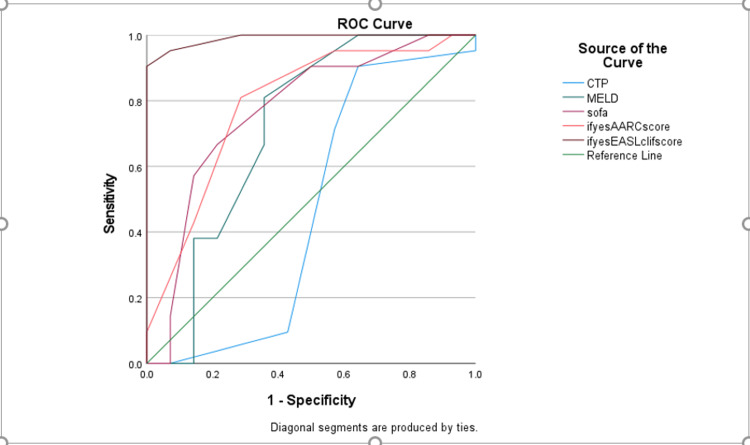 Figure 1
Figure 1| Dead | Survived | P-value | |
| Gender | |||
| Male | 20 (69) | 17 (77.3) | 0.510 |
| Female | 9 (31) | 5 (22.7) | |
| Clinical symptoms | |||
| Jaundice | 29 | 22 | |
| Abdominal distension | 29 | 21 (95.5) | 0.246 |
| Pedal edema | 28 (96.6) | 18 (81.8) | 0.080 |
| Oliguria | 26 (89.7) | 13 (59.1) | 0.011 |
| CAM | 19 (65.5) | 16 (72.7) | 0.583 |
| Past history of jaundice | 21 (72.4) | 10 (45.5) | 0.051 |
| Altered sensorium | 25 (86.2) | 14 (63.6) | 0.060 |
| Hematemesis | 9 (31) | 2 (9.1) | 0.059 |
| Melena | 11 (37.9) | 5 (22.7) | 0.246 |
| Blood transfusion | 11 (37.9) | 2 (9.1) | 0.019 |
| HE | |||
| Absent | 1 (3.4) | 8 (36.4) | 0.016 |
| Grade 1 | 8 (27.6) | 7 (31.8) | |
| Grade 2 | 10 (34.5) | 5 (22.7) | |
| Grade 3 | 7 (24.1) | 2 (9.1) | |
| Grade 4 | 3 (10.3) | 0 | |
| Etiology of CLD | |||
| ALD | 19 (65.5) | 17 (77.3) | 0.746 |
| Hepatitis B | 5 (17.2) | 3 (13.6) | |
| Hepatitis C | 1 (3.4) | 1 (4.5) | |
| NASH | 2 (6.9) | 0 | |
| Wilson disease | 1 (3.4) | 0 | |
| Others | 1 (3.4) | 1 (4.5) | |
| Precipitating factor of ACLF | |||
| Alcohol | 3 (10.3) | 6 (27.3) | 0.406 |
| Hepatitis A | 3 (10.3) | 1 (4.5) | |
| Hepatitis E | 2 (6.9) | 1 (4.5) | |
| Acute hepatitis B reactivation | 2 (6.9) | 0 | |
| DILI | 10 (34.5) | 5 (22.7) | |
| Alcohol+DILI | 5 (17.2) | 7 (31.8) | |
| Others | 4 (13.8) | 2 (9.1) | |
| APASL criteria | 29 (100) | 21 (95.9) | 0.246 |
| EASL criteria | 21 (75) | 15 (75) | 1.000 |
| Grade of CLIF-C ACLF | |||
| Ia | 0 | 5 (33.3) | <0.001 |
| Ib | 0 | 2 (13.3) | |
| II | 5 (23.8) | 8 (53.3) | |
| IIIa | 15 (71.4) | 0 | |
| IIIb | 1 (4.8) | 0 | |
| Grade of AARC score | |||
| 1 | 0 | 0 | <0.001 |
| 2 | 2 (6.9) | 11 (52.4) | |
| 3 | 27 (93.1) | 10 (47.6) | |
| Age | 47.83±11.86 | 43.05±11.44 | 0.154 |
| Duration of stays (in days) | 11.58±8.58 | 15.09±5.78 | 0.105 |
| Amount of alcohol (in grams) | 159.58±69.99 | 148.42±59.09 | 0.582 |
| Duration of alcohol (in years) | 11.41±4.53 | 12.26±4.65 | 0.574 |
| Ascitic fluid TLC | 916.60±931.30 | 408.00±363.90 | 0.025 |
| Urea (mmol/l) | 23.34±19.20 | 8.47±5.91 | 0.023 |
| Creatinine (mmol/l) | 246.24±148.89 | 184.68±156.40 | 0.159 |
| Total bilirubin | 403.66±187.57 | 391.81±158.52 | 0.813 |
| Direct bilirubin | 217.68±108.92 | 191.81±76.05 | 0.346 |
| Indirect bilirubin | 204.71±94.71 | 194.86±92.77 | 0.712 |
| AST | 213.48±120.38 | 195.36±119.82 | 0.729 |
| ALT | 106.10±12.34 | 94.95±80.67 | 0.816 |
| ALP | 132.05±84.27 | 133.95±38.68 | 0.922 |
| Total serum protein | 59.93±19.32 | 54.86±13.66 | 0.300 |
| Serum albumin | 20.67±6.25 | 21.82±8.20 | 0.568 |
| PT | 38.20±12.15 | 35.52±13.51 | 0.460 |
| INR | 5.05±3.99 | 4.21±4.05 | 0.465 |
| ABG pH | 6.75±1.57 | 6.99±1.14 | 0.552 |
| ABG lactate | 3.28±2.46 | 1.61±0.61 | 0.031 |
| SE | P-value | B | |
| Oliguria | 49954.911 | 0.999 | 0.000 |
| Blood transfusion | 13115.798 | 0.980 | 0.000 |
| HE grade | 1284.197 | 0.983 | 0.000 |
| Endoscopy | 5461.068 | 0.998 | 0.000 |
| Grade of EASL-ACLF | 23321.765 | 0.974 | 0.000 |
| Total serum protein | 57.119 | 0.981 | 0.258 |
| Urea | 239.249 | 0.991 | 15.042 |
| Ascitic fluid TLC | 5.946 | 0.975 | 1.207 |
| ABG lactate | 1791.559 | 0.993 | 12913906.435 |
| AARC score | 3747.933 | 0.997 | 0.000 |
| Test result variable(s) | Area | SE | Asymptotic sig. | Asymptotic 95% CI | Off | Sensitivity | Specificity | |
| Lower bound | Upper bound | |||||||
| CTP | 0.464 | 0.116 | 0.724 | 0.237 | 0.692 | 11 | 66.7 | 66.7 |
| MELD | 0.718 | 0.101 | 0.031 | 0.520 | 0.916 | 24 | 56.86 | 56.86 |
| SOFA | 0.770 | 0.087 | 0.007 | 0.599 | 0.942 | 5 | 60.6 | 88.9 |
| AARC score | 0.791 | 0.082 | 0.004 | 0.630 | 0.951 | 10 | 84.5 | 71 |
| CLIF-C ACLF | 0.990 | 0.012 | <0.001 | 0.967 | 1.000 | 9 | 56.86 | 56.86 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLiver Disease and Transplantation · Liver Disease Diagnosis and Treatment · Organ Transplantation Techniques and Outcomes
Introduction
Acute deterioration of chronic liver disease is a defining feature of acute-on-chronic liver failure (ACLF). The Asia-Pacific Association for the Study of the Liver (APASL) defines ACLF as acute hepatic insult manifesting as jaundice and coagulopathy complicated within four weeks by ascites and/or encephalopathy in a patient with previously diagnosed or undiagnosed chronic liver disease with high short-term mortality [1].
In contrast, it is described as an acute deterioration of pre-existing, chronic liver disease, usually related to a precipitating event and associated with increased mortality at three months due to multi-system organ failure by the working groups of the American Association for the Study of Liver Diseases (AASLD) and the European Association for the Study of the Liver (EASL) [2,3]. Liver injury is the primary component in the APASL statement, whereas organ failure is the main component of ACLF according to the EASL-AASLD consensus. This new entity was necessary because, if the triggering event can be controlled, ACLF may be reversible; if not, the short-term death rate is significant, ranging from 50% to 90% [2-7]. Infections like chronic hepatitis B reactivation are common in the East, whereas alcohol and bacterial infections are typically the acute insult in the West [1,8]. There is a wide range of data from India, and research has found that non-hepatic insults and hepatitis B reactivation are frequent acute precipitant variables [9,10]. This demonstrates that there are etiological disparities within the same country as well as between its various centers.
Because the two groups' definitions of ACLF differ fundamentally, data from the APASL and the EASL collaboration have produced a range of outcomes [8]. A new CLIF-C ACLF score system has been developed by the EASL consortium to better prognosticate these patients and determine which ones require liver transplantation right away. Similar studies have been done from the Indian subcontinent as well as by the Indian National Association for the Study of the Liver (INASL) consortium, which involved retrospective data and supported the fact that organ failure predicts outcome [9-11]. Some new simplified scores have been developed [12]. Since the study on ACLF has not been carried out extensively in Nepal, our current study aimed to identify the acute insults in ACLF and to identify predictors of in-hospital mortality in these patients.
Materials and methods
Study method
This is a single-centered observational cross-sectional study.
Study population
Patients with ACLF who met the inclusion criteria were included in the study from March 2024 to February 2025.
Study site
The study was done in the Department of Gastroenterology, Tribhuvan University Institute of Medicine, Kathmandu, Nepal.
Sample size
The minimum required sample size was calculated by using the formula \begin{document}\text{sample size}=\text{Z2}×\frac{\text{pq}}{\text{e2}}\end{document} where p is the incidence of ACLF in cirrhotic patients in Nepal and is equal to 3% [1], q=1-p, e is the precision and is equal to 0.05, Z is the confidence interval and is equal to 1.96, and the sample size is equal to 51.
Sampling method
Non-probability method was used to include the patients in the study.
Inclusion and exclusion criteria
Patients diagnosed with ACLF based on APASL and/or EASL-Chronic Liver Failure Consortium (CLIF) criteria and aged between 18 and 79 years were included in the study. However, patients diagnosed with ACLF based on criteria other than APASL and/or EASL-CLIF were excluded from the study. Similarly, patients fulfilling the APASL and or EASL-CLIF criteria with age <18 years, who were pregnant, with portal vein thrombosis, with hepatocellular carcinoma, and who were unwilling to participate in the study were also excluded.
Data collection tools and variables
Data was collected in a proforma. We collected data based on history, examination findings, and laboratory investigations. Chronic liver disease and ACLF were defined based on history, clinical examination, and laboratory investigations. The variables included in the study were sociodemographic variables like age and sex, comorbidities, laboratory investigation parameters, and several scoring systems for ACLF. The scoring systems were Child-Turcotte-Pugh (CTP), Model for End-Stage Liver Disease (MELD), Sequential Organ Failure Assessment (SOFA), APASL-ACLF Research Consortium (AARC), and CLIF-C ACLF [13-15]. These scoring systems were calculated manually and using mobile apps. The outcomes of the study were mortality and duration of hospitalization.
Ethics
The Institutional Review Committee of Tribhuvan University Institute of Medicine granted ethical approval (approval number: 517(6-11) E2 080/081). All study participants gave their informed consent to allow the use of anonymous personal and clinical data in research, which was used to ensure complete confidentiality.
Statistical analysis
Data was compiled, edited, and checked daily to maintain consistency. The data was collected in Microsoft Excel (Microsoft Corporation, Redmond, Washington, United States). For statistical analysis, IBM SPSS Statistics for Windows Version 27.0 (Released 2019; IBM Corp., Armonk, New York, United States) was used. Quantitative variables are expressed as mean±SD and categorical variables as frequency and percentage. The normally distributed continuous and categorical variables were compared using Student's t-test and the chi-squared test, respectively. Univariate and multivariate logistic regression analyses with odds ratios were done to ascertain the predictors of mortality. Mortality prediction of various scores is compared by receiver operating characteristic (ROC) curve analysis by calculating the area under the curve (AUC). A p-value of <0.05 was considered statistically significant.
Results
A total of 51 patients who fulfilled our inclusion and exclusion criteria were included in the study. The mean age of presentation was 45.76±11.81 years. In our study, 37 (72.5%) were male, while 14 (27.5%) were female. The most common clinical symptoms were jaundice (51, 100%), followed by abdominal distension (50, 98%), pedal edema (46, 90.2%), and oliguria (39, 76.5%). Icterus and ascites were present in all patients. Alcohol is the most common cause of cirrhosis, which is present in 36 (70.6%) patients, followed by chronic hepatitis B (8, 15.7%), non-alcoholic steatohepatitis (NASH) (2, 3.9%), chronic hepatitis C (2, 3.9%), and Wilson disease (1, 2%). Drug-induced liver injury (DILI) (in the form of complementary and alternative medicine (CAM)) was the most common precipitating insult in 15 (29.4%) patients. The demographic profile, clinical features, examination findings, and laboratory investigation are shown in Table 1.
Out of 51 patients, 29 (56.9%) died. About 50 (98%) patients followed the APASL definition of ACLF; however, only 36 (70.6%) met the EASL definition of ACLF. While staging and comparing mortality ACLF based on AARC score, we found that no one in grade 1 died and 27 (93.1%) patients in stage 3 died. While comparing similar findings in patients who met EASL-CLIF, no patients survived.
Mortality predictors
On univariate analysis, patients with a decrease in urine output, who needed multiple blood transfusions, and who had high HE grade, large varices in endoscopy, higher grades of ACLF, low total serum protein, high urea level, high ascitic total count, and high lactate on admission day died more and were statistically significant (p<0.05 for every variable). Multivariate analysis of those variables was not able to show statistical significance in predicting mortality (Table 2).
We compared the predictability of each score with mortality using the ROC curve, calculating the AUC for each component. CLIF-C ACLF has predictability with an AUC of 0.990, followed by AARC with an AUC of 0.791, SOFA with an AUC of 0.770, and MELD with an AUC of 0.718 (Table 3); however, the CTP score with an AUC of 0.464 did not show concordance to predict mortality (Figure 1).
ROC curves of scores predicting mortality on admissionROC: receiver operating characteristic; CTP: Child-Turcotte-Pugh; MELD: Model for End-Stage Liver Disease; SOFA: Sequential Organ Failure Assessment; AARC: APASL-ACLF Research Consortium
Discussion
Since ACLF is a relatively new entity, our work contributes to the body of emerging and not yet comprehensive literature and evidence. When compared to the West, the etiology of both acute and chronic insults differs in the East [11,13,16-19]. The etiology of chronic liver disease varies greatly within the Indian subcontinent alone [13].
In 70.6% of the patients in our study, alcohol-related liver cirrhosis was the most common primary cause, followed by hepatitis B (15.7%). Although the results are consistent with a small number of other research, these findings contribute to the more varied nature of the underlying causes of cirrhosis [9,16,19] but contrast with other Indian research that found that only 10-30% of people had alcoholic cirrhosis [10,18,20]. According to certain studies, 30-64% of people with ACLF had cirrhosis, with chronic hepatitis B being the most common cause. Similarly, the majority of data from Taiwan and China likewise showed that hepatitis B virus (HBV) was the main cause of cirrhosis in individuals with ACLF [21,22]. However, 50% of patients in a big research by Moreau et al. had liver illness linked to alcohol in the West [8]. This demonstrates that there are etiological distinctions between the East and West of the planet.
In our study, 51 patients were enrolled, with an average age of presentation of 45.76±11.81 years. Males comprised 72.5% of the study population, indicating a male predominance. These findings are comparable to previous studies from India. Sarin et al. [13] reported an average age of 44.7±12 years with 82% male predominance, while Dhiman et al. [23] observed an average age of 46±13 years, with males accounting for 86% of cases. However, the CANONIC study [24] reported a slightly older average age of presentation (56.2±11.6 years), though males remained the predominant group (64.6%). The younger age of presentation in our study may be attributed to the etiology of cirrhosis. A study by Ferreira Cardoso et al. [25] found that ACLF in younger patients was predominantly associated with alcohol-related cirrhosis. Similarly, Arroyo et al. [26] reported ACLF occurring in relatively younger patients, particularly in those with alcohol-related liver disease and untreated chronic hepatitis B infection.
Regarding the etiology of cirrhosis, alcohol was the leading cause in our study, accounting for 70.6% of cases. This finding aligns with a previous Nepalese study, where alcohol-related cirrhosis constituted 84.94% of cases [27]. The high prevalence of alcohol consumption in Nepal could be attributed to factors such as easy availability, cultural acceptance, and inadequate governmental regulations. A study by Rathod et al. [28] reported that 15-57% of Nepali adults had consumed alcohol at some point, with 1.5-25% meeting the criteria for alcohol use disorder. In contrast, Nepal has a relatively low prevalence of hepatitis B (0.9%) and hepatitis C (0.38%) infections [29]. Although NASH is emerging as a significant etiology worldwide, the relatively low average BMI of our study population (20.9±1.8 kg/m²) suggests that it is not yet a major contributor in our setting [30].
DILI, primarily due to the consumption of CAM, was identified as the most common precipitating factor (29.4%), followed by concurrent use of alcohol and CAM and alcoholic hepatitis. Acute viral hepatitis, including hepatitis B reactivation, was responsible for only 18% of cases. The use of herbal products is widespread in Nepalese society, often preceding disease exacerbation and hospitalization. Although there is limited local data, a study from India by Philips et al. [31] found that 32% of patients had used CAM before being diagnosed with cirrhosis and 68% had used it at some point after diagnosis. Additionally, 39% of ACLF cases in that study were linked to CAM use.
The precipitating factors for ACLF vary across different regions. The study by Sarin et al. [13] in India identified alcohol (35.7%) as the most common precipitating factor, followed by viral hepatitis (21.4%) and sepsis (16.6%). In contrast, an Egyptian study by Zakareya et al. [32] found sepsis (49.8%) to be the leading precipitant. Similarly, a study from Taiwan by Huang et al. [33] reported reactivation of hepatitis B (68.4%) as the most common cause. The CANONIC study identified sepsis (32.6%) as the predominant precipitant [34]. Unlike these international studies, our study observed that sepsis and viral hepatitis, including hepatitis B reactivation, were minor contributors to ACLF.
ACLF is associated with high short-term mortality due to rapid hepatic decompensation and subsequent multi-organ failure. In our study, the overall mortality rate was 56.9%, occurring within two weeks of hospital admission. This finding is comparable to the study by Valantine et al. [35] in India, which reported a mortality rate of 56%. However, the CANONIC study [34] observed a lower mortality rate of 33%. The higher mortality rate in Asian populations may be attributed to the lack of or inadequate liver transplant facilities and the unavailability of dedicated liver intensive care units.
Univariate analysis in our study identified oliguria, HE grade, ACLF grades, total serum protein, urea levels, ascitic fluid total leukocyte count, serum lactate, and AARC score as significant predictors of mortality. These findings align with the study by Valantine et al. [35], where HE, total serum protein, and ascites were identified as mortality predictors. However, multivariate analysis in our study did not reveal any statistically significant predictors of mortality. This contrasts with the study by Valantine et al. [35], which found bilirubin levels to be a significant predictor. One limitation of our study was that we only assessed baseline parameters at admission without follow-up measurements. Evaluating these parameters at different time points (e.g., day 3, day 7) might have provided more conclusive insights.
Among various scoring systems, the CLIF-C ACLF score emerged as the most efficient predictor of mortality in our study, with an AUC of 0.99, followed by AARC (0.791), SOFA (0.770), MELD (0.710), and CTP (0.464). These findings are consistent with previous studies. Barosa et al. [36] demonstrated that the CLIF-C ACLF score was superior to SOFA, MELD, and CTP in predicting mortality. Similarly, Leão et al. [37] compared CLIF-C ACLF and AARC scores and found CLIF-C ACLF to be the better predictor. MELD was found to be a better predictor than CTP, as shown in the study by Antunes et al. [38]. The superior predictive ability of CLIF-C ACLF, AARC, and SOFA scores can be attributed to their inclusion of organ failure as a scoring component. In contrast, the CTP score primarily assesses hepatic dysfunction, making it a weaker predictor. The MELD score, which incorporates kidney function along with hepatic dysfunction parameters, is therefore a better predictor than CTP.
This study has some limitations. The sample size was small, which made it difficult to analyze subgroups based on regional differences. Mortality prediction was based on a single assessment of risk factors. Long-term follow-up was not included. Repeated measurements over time could have given better insights into outcomes, especially in critically ill ACLF patients.
Conclusions
The short-term mortality rate of ACLF, an emergent entity, is extremely high. Both the acute triggering cause and the underlying chronic cause vary greatly throughout the world, including within Nepal. In order to classify patients with ACLF into limited intensive care units and develop new treatments, different prognostic ratings may be used. In forecasting these patients' short-term mortality, the CLIF-C ACLF scoring system outperforms conventional prognostic ratings. More research is needed to shed more light on this developing idea of ACLF and help us manage these patients more effectively.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Acute-on-chronic liver failure (ACLF): the 'Kyoto Consensus'-steps from Asia Hepatol Int Choudhury A Kulkarni AV Arora V 1691920253996197610.1007/s 12072-024-10773-4PMC 11846769 · doi ↗ · pubmed ↗
- 2Acute-on chronic liver failure J Hepatol Jalan R Gines P Olson JC 133613485720122275075010.1016/j.jhep.2012.06.026 · doi ↗ · pubmed ↗
- 3Acute-on-chronic liver failure: concept, natural history, and prognosis Curr Opin Crit Care Olson JC Kamath PS 1651691720112132609510.1097/MCC.0b 013e 328344 b 42d · doi ↗ · pubmed ↗
- 4Acute-on-chronic liver failure: current concepts on definition, pathogenesis, clinical manifestations and potential therapeutic interventions Expert Rev Gastroenterol Hepatol Laleman W Verbeke L Meersseman P 523537520112178089910.1586/egh.11.47 · doi ↗ · pubmed ↗
- 5Liver transplantation for acute-on-chronic liver failure Hepatol Int Chan AC Fan ST Lo CM 571581320091968073310.1007/s 12072-009-9148-8PMC 2790588 · doi ↗ · pubmed ↗
- 6Clinical profile, natural history, and predictors of mortality in patients with acute-on-chronic liver failure (ACLF)Wien Klin Wochenschr Mikolasevic I Milic S Radic M Orlic L Bagic Z Stimac D 28328912720152582105310.1007/s 00508-015-0707-9 · doi ↗ · pubmed ↗
- 7Acute-on-chronic liver failure (ACLF)--a new entity in hepatology? [Article in Croatian]Lijec Vjesn MikolasevićI RadićM MilićS Stimac D 3223251352013 https://pubmed.ncbi.nlm.nih.gov/24490333/24490333 · pubmed ↗
- 8Diagnosis, prevalence, and prognosis of acute-on-chronic liver failure (ACLF) : results of the EASL-Chronic Liver Failure (CLIF) consortium : CANONIC study 2 2025 2012 https://difusion.ulb.ac.be/vufind/Record/ULB-DIPOT:oai:dipot.ulb.ac.be:2013/146181/Details