Methodologies for studying depression in persons living with tuberculosis: Protocol for a scoping review
Amanda J. Gupta, Patricia Turimumahoro, Lori Rosman, Jonathan E. Golub, David W. Dowdy, Mickael Essouma, Mickael Essouma, Mickael Essouma, Mickael Essouma

TL;DR
This paper outlines a scoping review protocol to map methodologies used to study depression in people with tuberculosis, aiming to identify research gaps and improve detection and treatment strategies.
Contribution
The study introduces a structured scoping review protocol using the RE-AIM framework to evaluate methodologies for depression in tuberculosis patients.
Findings
The review will assess study designs, diagnostic tools, and treatment interventions for depression in tuberculosis patients.
It will evaluate the reach, effectiveness, adoption, implementation, and maintenance of depression methodologies in TB care.
The findings will highlight gaps in research and inform future study designs and clinical strategies.
Abstract
Tuberculosis (TB) and depression frequently co-occur, yet research has largely focused on prevalence rather than diagnostic or treatment methodologies. Given overlapping symptoms, robust research approaches are critical for improving detection and treatment strategies in persons with TB (PWTB). This protocol defines a scoping review that aims to map methodologies used to study depression in individuals with TB, identifying gaps in research design, diagnosis, and treatment that may hinder clinical and public health advancements. A search was conducted in MEDLINE, Embase, PsycINFO, Global Health, Cochrane Library, and Africa-Wide Information using controlled vocabulary related to TB and depression. Studies examining the TB-depression relationship will be included. We will use Covidence to facilitate screening, selection, and data extraction. We will extract data on study design,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
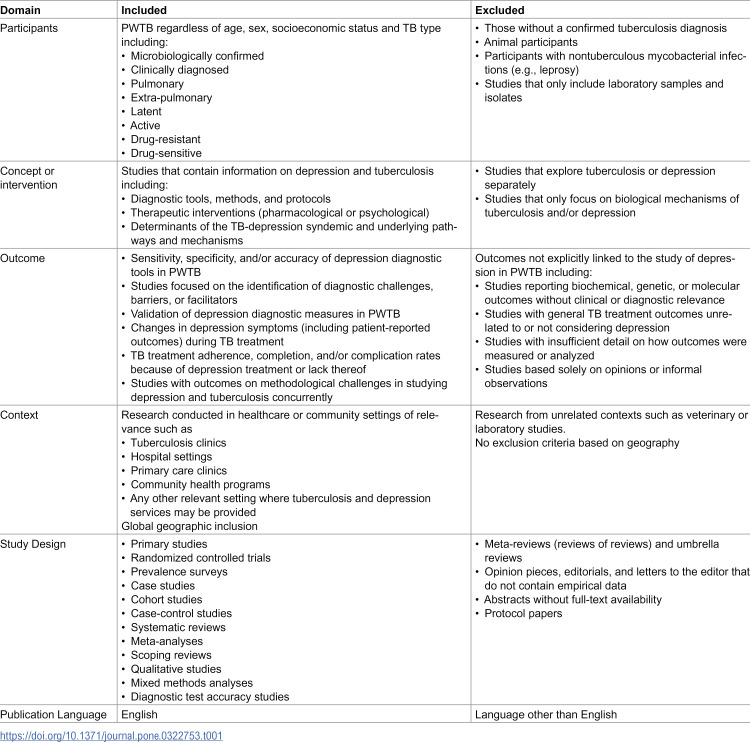 Figure 1
Figure 1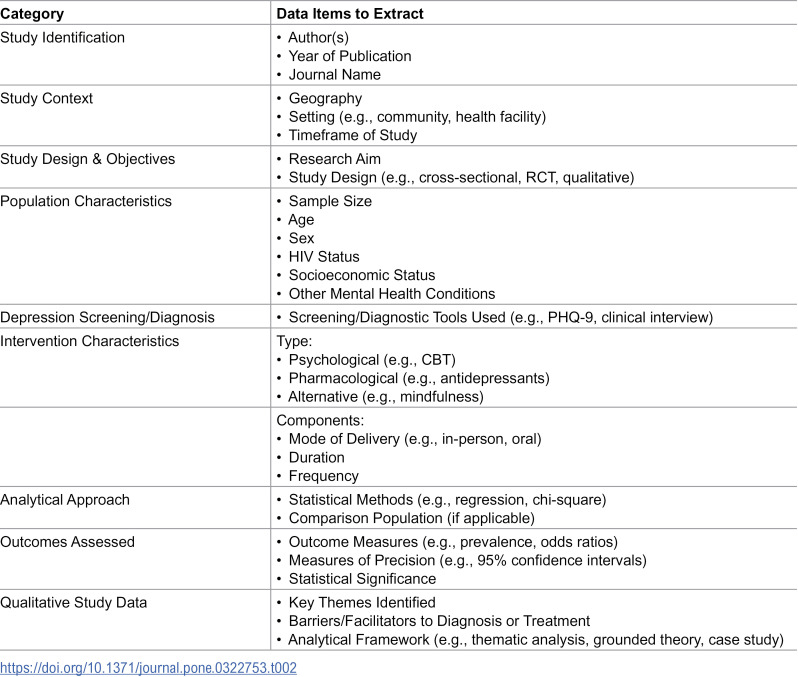 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTuberculosis Research and Epidemiology · Schizophrenia research and treatment · Pneumocystis jirovecii pneumonia detection and treatment
Introduction
Tuberculosis (TB), a communicable disease caused by Mycobacterium tuberculosis, is one of the leading infectious causes of mortality worldwide [1]. While it primarily affects the lungs (pulmonary TB), it can be found in other places throughout the body (extrapulmonary TB). The COVID-19 pandemic accelerated deaths due to TB as less attention, and subsequently funding, has been paid to TB [1,2]. This resulted in ~10.8 million people developing new cases of active TB in 2023 with ~1.25 million deaths due to TB disease [1]. Active TB refers to disease in which TB bacteria are replicating and causing clinical symptoms. Pulmonary TB is typically symptomatic and infectious while extrapulmonary TB is usually symptomatic but not transmissible. This contrasts with latent TB, a state in which an individual is infected but asymptomatic and non-infectious. It is estimated that billions of individuals worldwide have latent TB [1]. Furthermore, TB can be classified by drug resistance with ~400,000 persons with TB (PWTB) having multidrug-resistant TB (MDR-TB) in 2023 [1]. Despite this large burden, TB is vastly underfunded leading to under-supported research endeavors and national TB programs left without appropriate funding to successfully combat the large TB burdens that they may face [1–5]. This results in gaps in TB diagnosis, treatment, and care in high TB burden settings [6–8].
One such gap in care is in the screening, diagnosis, and treatment of comorbidities in PWTB [9]. While the diagnosis and treatment protocols of infectious comorbidities of TB such as Human Immunodeficiency Virus (HIV) have been extensively researched [10–13], the diagnosis and treatment of comorbid mental health disorders have received little attention, despite their impacts on TB treatment [9,14,15]. Depression is one such overlooked comorbidity with potentially large impacts on PWTB [16,17]. Depression, a common mental health condition characterized by persistent sadness, loss of interest or pleasure, and functional impairment, can affect quality of life if not properly managed [18]. While clinically defined in various tools, its expression and recognition vary across cultural contexts, increasing its diagnostic and treatment complexity [19].
Depression appears to impact PWTB more frequently than the general population. One systematic review estimates the depression prevalence amongst PWTB to be 45% [20]. Depression may not only be a consequence of TB, but also a risk factor due to its effects on immune function, health-seeking behavior, and treatment engagement [15,21,22]. TB-depression co-occurrence can be thought of as a syndemic, or an interacting set of conditions that cluster within social disadvantage (e.g., stigmatization of health conditions and economic vulnerability) that results in an increased burden of disease [23–25]. The burden of depression may also vary by TB subtype. For example, individuals with extrapulmonary TB may face diagnostic uncertainty that heightens psychological distress [26,27]. Those with MDR-TB often endure prolonged treatment, more severe side effects, greater economic uncertainty, and greater social isolation, all of which may increase the risk or severity of depression [28,29].
Given this complex interplay, most PWTB are never screened for depression, let alone receive treatment for depression. This is due to a lack of providers, funding, cultural norms, and stigma [20,22,30,31]. From a public health perspective, untreated depression contributes to delays in TB diagnosis and treatment initiation [30,32], non-adherence to TB medications [33,34], and ultimately increases negative TB outcomes such as loss to follow up and death [35,36].
Despite the significant impact of depression in PWTB, research has largely been limited to prevalence surveys. Few studies have used longitudinal designs and even fewer explore the methodologies used to screen, diagnose, or treat depression in PWTB. This may be in part due to diagnostic challenges posed by overlapping symptoms, such as TB-related fatigue, weight loss, and general malaise, all of which can masquerade as signs of depression, leading to misdiagnoses or missed diagnoses.
Given the substantial burden of depression among PWTB and the large focus on prevalence estimates within the literature, a scoping review is particularly needed to broadly map the existing evidence, identify the most pressing knowledge gaps, and clarify how research has been conducted when studying these comorbid conditions. Therefore, we aim to conduct a scoping review to examine the methodologies used to study depression in PWTB, including diagnostic and treatment methodologies, identifying research gaps and highlighting opportunities for improved methodological approaches.
Methods
This section is presented in accordance with the scoping review framework by Arskey and O’Malley [37] and refined by Levac et al [38] which guided the methodology of our scoping review. This framework consists of six steps: 1) Identifying the research question 2) Identifying relevant studies 3) Study selection 4) Charting the data 5) Collating, summarizing, and reporting the results and 6) Consultation with stakeholders on study findings.
Identifying the research question
The research question for our review is: what methodologies have been used in the research literature to study depression (including diagnosis and treatment) among individuals with tuberculosis, and what are the gaps in methodological approaches?
Identification of relevant studies
Table 1 includes the eligibility criteria for this scoping review. We searched the following electronic databases: MEDLINE, Embase, Global Health, the Cochrane Library, the WHO Regional Libraries, Africa-Wide Information, and PsycINFO. These databases were selected for their relevance to the scope of this review: MEDLINE, Embase, Global Health, and the Cochrane Library are widely used for biomedical and public health research; the WHO Regional Libraries and Africa-Wide Information are included to ensure geographic representation, particularly from high TB burden regions such as sub-Saharan Africa; and PsycINFO is included for its comprehensive coverage of psychological and mental health research. The preliminary search strategy, constructed by a trained medical librarian (LR) after several weeks of testing various combinations of terms to ensure maximum reach, focused on combinations of terms related to “tuberculosis” and terms related to “depression” (S1 File).
Table 1: Study eligibility criteria.
We did not include date restrictions. The electronic database search will be supplemented by manual searches, including the screening of reference lists from all included studies to identify any additional relevant articles that may have been initially missed.
Study selection
We are using Covidence to screen study titles, abstracts and full text articles for inclusion. Two reviewers (AJG, PT) will review abstracts in parallel for inclusion. To minimize bias, reviewers will be blinded to each other’s ratings except when resolving conflicts. Reviewers will meet after every 20 abstracts to resolve any conflicts and to propose/implement updates to the search strategy or inclusion criteria. All abstracts that pass screening will have the full text reviewed by the two reviewers, again, in parallel for final inclusion in the review. Disagreements will be resolved via discussion and, if needed, by a third reviewer (DWD).
Charting the data
After piloting the data extraction tool, we will extract data using Covidence. We will extract pertinent study details which can be found in Table 2. Additionally, if the authors identify any limitations relevant to the research question, such as methodological limitations, we will extract this data. One author (AJG) will extract the data with a second reviewer (PT) checking extracted data for accuracy. These two authors will routinely meet during the data extraction phase to ensure the extraction tool is capturing all relevant data needed to answer the overall research question.
Table 2: Data extraction.
Results
Collating, summarizing, and reporting results
We will provide descriptive characteristics of all included studies using figures and tables to fully summarize the studies, stratifying where appropriate by key variables such as by age, TB type, geographic location and/or study design to name a few. While we will not consider literature quality among inclusion criteria, we will conduct a quality appraisal for each study as the presence or absence of high-quality research is relevant to understanding research gaps. As there will be many different study designs, to assess quality, we will use the Jadad scale for randomized controlled trials, the Newcastle-Ottawa scale for observational studies, and the Joanna Briggs Institute Critical Appraisal Tool for Qualitative Research.
We will structure the reporting of our results using the RE-AIM (Reach, Effectiveness, Adoption, Implementation and Maintenance) framework [39]. For reach, we will determine the extent to which studies have explored both directions of the TB-depression relationship. We will also determine the reach of researchers in terms of including representative samples of PWTB and their inclusion of high-risk groups (such as those with HIV, drug-resistant TB, or pediatric cases). For effectiveness we will categorize the study designs used to assess the diversity of methodological approaches. A wide range of designs – such as cross-sectional, longitudinal, and randomized– is essential for fully elucidating the co-occurrence of TB and depression. A lack of diverse study designs may indicate gaps in the field’s ability to fully understand this relationship. Additionally, we will determine the types of diagnostic measures used for depression along with their effectiveness (if reported) as well as how efficacious or effective any treatment interventions were at impacting depression- or TB-outcomes.
For adoption we will look at the extent to which depression screening, diagnosis, and treatment methodologies are being adopted in different settings (such as by national programs, referral centers, local clinics, etc) and by whom (e.g., physicians, nurses, community health works etc.) and examine the way in which research findings on these two diseases have impacted clinical guidelines and public health policies if mentioned by study authors. For implementation, we will determine barriers and facilitators identified to the implementation of depression related care in real-world TB treatment settings. Finally, for maintenance we will determine whether any depression related methodologies for diagnosis or treatment were sustained or embedded within existing health systems. This will include, if reported upon, long-term patient outcomes, if methodologies persisted beyond the research phase, and if any studies evaluated how health systems integrated and sustained any proposed diagnostic or treatment interventions.
Consultation with stakeholders
We will include a consultation phase to enhance the relevance and applicability of our findings. We will engage a diverse group of stakeholders, drawing on global collaborators with expertise in TB and mental health from an established network of the research team, as well as individuals with lived experience of TB, including PWTB from Uganda who are participating in an unrelated, ongoing cohort study. Consultations will offer contextual insights and help identify gaps or implementation issues not captured in the published literature, ensuring the findings are meaningful and actionable for high TB burden settings.
Data sharing
In line with open science principles, we will make the final data extraction sheet and study metadata openly available through a public repository such as the Open Science Framework upon completion of the review.
Timeline
The initial search was conducted on March 31, 2025. All screening, including title and abstract screening and full text screening are taking place from April to June 2025. Data extraction will take place in July 2025. Analysis and synthesis of results will take place from July to August 2025 with final results expected by September 2025.
Discussion
This scoping review will explore the existing literature on the intersection between depression and TB allowing us to identify research gaps. Importantly, this will allow us to understand methodological gaps that exist and approaches that researchers have historically taken to tackle these two diseases concurrently.
Findings from this review could contribute to advancing research beyond cross-sectional prevalence surveys by encouraging the use of other quantitative, qualitative, and mixed-methods study designs that can better inform evidence-based practice. Furthermore, this review could underscore the urgent need for validated diagnostic tools and specialized treatment approaches to address overlapping symptoms between TB and depression, ultimately supporting the development of more effective strategies.
Strengths of our review will include methodological rigor as we are using the Levac et al framework to ensure a systematic and transparent approach to study identification and selection. This will be enhanced through the use of RE-AIM to synthesize results, providing a structured lens to assess how methodological approaches to researching TB and depression have created a knowledge base as well as gaps in studying the diseases concurrently. Finally, the planned stakeholder consultations will add depth and practical relevance to the final interpretation of findings, ensuring methodological rigor and relevance to global TB and mental health research practices.
Our review will have some limitations that are worth discussing a priori. First, we have limited the search to English language studies. Given the burden of tuberculosis in non-English speaking countries, this may exclude several studies that would otherwise be eligible. Second, we are beginning this search with the term depression, a Western term, and its associated synonyms. Many countries use alternate terms for depression, such as shenjing shuairuo (nervous weakness) in China or yuutsu in Japan, meaning that our initial search may not fully capture the available literature. Given the long list of terms that could be used by different countries, it is not likely we will capture all possible terms and subsequently may miss eligible publications. Third, scoping reviews cannot make definitive conclusions about intervention effectiveness or causality given their focus on describing existing literature. However, it may be appropriate to conduct a subsequent systematic review and meta-analysis to assess public health impact of depression-related interventions amongst PWTB. Finally, as with all scoping reviews, the breadth of study types and topics can make data synthesis more complex than in a systematic review. We believe our use of RE-AIM to structure the results, regardless of study type, will aid in creating meaningful outputs.
Conclusions
This scoping review will advance understanding of how depression screening, diagnosis, and treatment have been studied in the context of tuberculosis by systematically mapping existing methodologies and identifying critical research gaps to guide future public health research and intervention development.
Supporting information
S1 FileInitial Search terms by database.(DOCX)
S2 FilePRISMA-P Checklist.(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization. Global Tuberculosis Report 2024. Geneva. 2024. https://www.who.int/teams/global-programme-on-tuberculosis-and-lung-health/tb-reports/global-tuberculosis-report-2024
- 2World Health Organization. Global Tuberculosis Report 2022. Geneva, Switzerland: World Health Organization. 2022. https://www.iom.int/sites/g/files/tmzbdl 486/files/documents/2023-03/Global-TB-Report-2022.pdf
- 3Chaisson RE, Frick M, Nahid P. The scientific response to TB - the other deadly global health emergency. Int J Tuberc Lung Dis. 2022;26(3):186–9. doi: 10.5588/ijtld.21.0734 35197158 PMC 8886961 · doi ↗ · pubmed ↗
- 4Venkatesan P. Worrying lack of funding for tuberculosis. Lancet Infect Dis. 2022;22(3):318. doi: 10.1016/S 1473-3099(22)00073-1 35218748 PMC 8865854 · doi ↗ · pubmed ↗
- 5Treatment Action Group. Tuberculosis research funding trends 2005-2023. New York, New York: Treatment Action Group. 2024.
- 6Armstrong-Hough M, Turimumahoro P, Meyer AJ, Ochom E, Babirye D, Ayakaka I, et al. Drop-out from the tuberculosis contact investigation cascade in a routine public health setting in urban Uganda: A prospective, multi-center study. P Lo S One. 2017;12(11):e 0187145. doi: 10.1371/journal.pone.0187145 29108007 PMC 5673209 · doi ↗ · pubmed ↗
- 7Kim J, Keshavjee S, Atun R. Health systems performance in managing tuberculosis: analysis of tuberculosis care cascades among high-burden and non-high-burden countries. J Glob Health. 2019;9(1):010423. doi: 10.7189/jogh.09.010423 31263546 PMC 6592589 · doi ↗ · pubmed ↗
- 8Subbaraman R, Jhaveri T, Nathavitharana RR. Closing gaps in the tuberculosis care cascade: an action-oriented research agenda. J Clin Tuberc Other Mycobact Dis. 2020;19:100144. doi: 10.1016/j.jctube.2020.100144 32072022 PMC 7015982 · doi ↗ · pubmed ↗