Cytomegalovirus Enteritis: A Rare Culprit of Protein Losing Enteropathy in an Immunocompetent Adult
Nancy Mayer, Vijay Kata, Dhaval Patel, Daniel Errampalli, Thomas O'Connor, Matthew Kaplan, Thomas Betlej, Nikhil Bhargava

TL;DR
A 60-year-old healthy woman developed a rare condition called protein-losing enteropathy due to a cytomegalovirus infection, which was successfully treated with valganciclovir.
Contribution
This case report highlights CMV enteritis as a rare cause of PLE in immunocompetent adults.
Findings
The patient had low serum protein and increased fecal alpha-1 antitrypsin, confirming PLE.
CMV-specific immunohistochemistry confirmed CMV enteritis as the cause of PLE.
Treatment with valganciclovir resolved symptoms and normalized endoscopic findings.
Abstract
Protein-losing enteropathy (PLE) is a rare complication of cytomegalovirus (CMV) enteritis in immunocompetent individuals. We present a case of a previously healthy 60-year-old woman with an acute CMV infection, manifesting as intractable vomiting and diarrhea, refractory electrolyte disturbances, and anasarca. The diagnostic evaluation showed low serum protein levels and an increased fecal alpha-1 antitrypsin clearance, confirming PLE. CMV-specific immunohistochemistry on duodenal samples subsequently confirmed that the PLE was caused by CMV enteritis. She completed treatment with valganciclovir for 3 weeks, resulting in symptom resolution and normalization of endoscopic findings. This case highlights the importance of recognizing CMV-associated PLE, particularly in immunocompetent individuals, for timely diagnosis and treatment.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
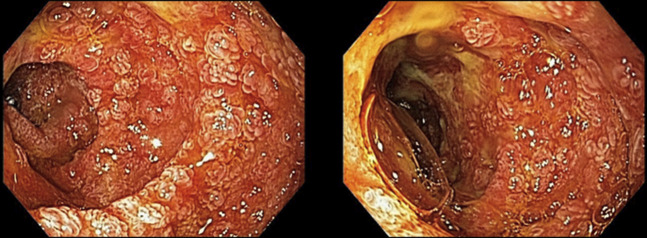 Figure 1
Figure 1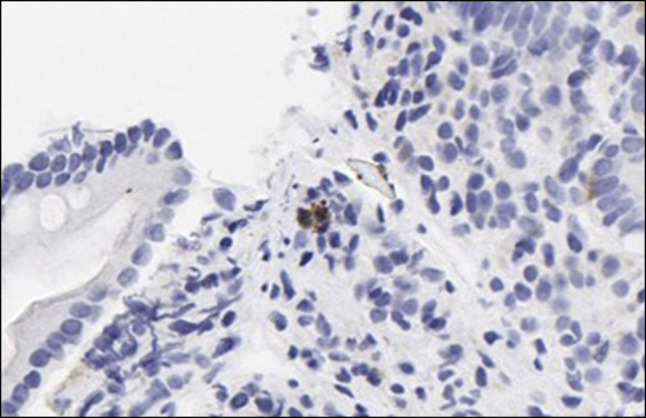 Figure 2
Figure 2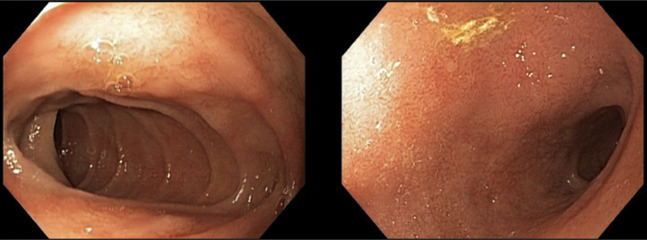 Figure 3
Figure 3| Reference | Age | Sex | Coexisting conditions | Presentation | Laboratory markers of systemic CMV involvement | Imaging results | Endoscopic observations | Histopathologic features | CMV diagnostic methods | Treatment | Outcome |
| Ciavaldini | 28 | M | None | Abdominal pain, edema | Elevated LFTs | Gastric and small bowel inflammation, lymphadenopathy | Ulcerative and congestive gastritis | Ulcerative and edematous gastritis | Serology+ Molecular+ | Symptomatic | Resolution |
| Yasuoka | 40 s | M | HTN, HLD | Diarrhea | — | Ileal and colonic thickening | Ileal and colonic ulceration | Intranuclear inclusion bodies | IHC+ | Ganciclovir | Resolution |
| Ochiai | 74 | F | None | Diarrhea, abdominal pain, edema | — | Ileal edema and thickening | Ileitis with ulceration | Ulcerative mucosa with intranuclear inclusion bodies | IHC+ | Ganciclovir | Resolution |
| Perrineau | 35 | M | None | Abdominal pain, vomiting, peritonitis | Leukocytosis, elevated CRP | Gastric and small bowel thickening | Mild gastritis and duodenitis | Chronic duodenitis with intranuclear inclusion bodies | Serology+ | Symptomatic | Resolution |
| Lalazar | 25 | M | None | Abdominal pain, vomiting, fever | Leukocytosis, elevated LFTs | Hepatomegaly, splenomegaly | Esophagitis, thickened gastric folds with erosions | Foveolar hyperplasia with intranuclear inclusion bodies | Serology+ | Symptomatic | Resolution |
| Chen | 22 | M |
| Epigastric pain, vomiting | Leukocytosis, elevated LFTs | Unremarkable | Erosive gastritis | Acute gastritis with intranuclear inclusion bodies | Serology+ | Ganciclovir | Resolution |
| Engjom | 30 s | M | None | Sore throat, edema, epigastric pain, fever | Elevated fecal calprotectin | Mildly enlarged spleen, enlarged mesenteric lymph nodes | Thickening of the gastric folds | Foveolar hyperplasia with intranuclear inclusion bodies | Serology+ | Ganciclovir followed by oral valacyclovir | Resolution |
| Suter | 34 | M | None | Diarrhea, abdominal pain, fever | Elevated LFTs | Hepatomegaly | Thickening of the gastric folds with erosions | Chronic active gastritis | Serology+ | Symptomatic | Resolution |
| Kraus | 76 | M | Ulcerative colitis | Abdominal pain | — | — | Pancolitis with rectal sparing | Acute pancolitis | Serology+ | Ganciclovir | Resolution |
| Nakase | 22 | M | None | Edema | Leukocytosis | — | - | Edematous ilium | Serology+ | Symptomatic | Resolution |
| Bencharif | 23 | M | None | Epigastric pain, diarrhea, edema, fever | Elevated LFTs | Lymphadenopathy, splenomegaly | Severe gastritis and thickening of gastric folds | Nonspecific gastritis and edematous gastritis | Serology+ | Symptomatic | Resolution |
| Nakazato | 38 | M | None | Sore throat, fever | Elevated LFTs | Lymphadenopathy, hepatomegaly | Thickening of the gastric folds | Foveolar hyperplasia | Serology+ | Symptomatic | Resolution |
| Underwood | 68 | F | None | Stomatitis, diarrhea | Elevated ESR | — | Necropsy: Jejunal ulceration | Jejunitis with intranuclear inclusion bodies | — | — | Deceased from chest infection |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCytomegalovirus and herpesvirus research · Immunodeficiency and Autoimmune Disorders · Pneumocystis jirovecii pneumonia detection and treatment
INTRODUCTION
Protein-losing enteropathy (PLE) is a rare condition characterized by an excessive leakage of plasma proteins into the gastrointestinal tract. Excessive protein loss presents clinically with third-space fluid accumulation (ascites, pleural, and pericardial effusions) along with malnutrition. Though rare, there are diverse causes of PLE that can be divided into inflammatory disorders, disorders of mucosal permeability, and disorders involving lymphatic obstruction. Some culprit diseases include congestive heart failure, lymphoma, and inflammatory bowel disease.^1^ Cytomegalovirus (CMV) is a rarely described culprit of PLE in an otherwise healthy adult, with only 13 documented cases in literature^2–15^ (Table 1). In this study, we present a case of PLE due to acute CMV enteritis in an immunocompetent patient.
CASE REPORT
A previously healthy 60-year-old woman presented to the emergency department with intractable nausea, vomiting, and watery diarrhea for 2 weeks. She reported generalized fatigue during this period but denied fever, chills, myalgias, headache, dyspnea, vision changes, or sore throat. Physical examination was significant for diffuse abdominal tenderness, though the abdomen was soft and nondistended. He had no lymphadenopathy, enlarged tonsils, abnormal lung sounds, rash, or hepatosplenomegaly. Laboratory evaluation revealed mild leukocytosis (11.63 × 10^3^/μL) with normal C-reactive protein levels and liver function tests. Contrast-enhanced computed tomography showed mild splenomegaly with normal-appearing bowel and liver. Initial infectious workup, including Clostridioides difficile toxin, rotavirus and norovirus antigens, and bacterial stool cultures, was negative. Intravenous fluids were initiated; however, within a day, she developed anasarca, bilateral pleural effusions, and pronounced electrolyte disturbances despite aggressive replacement. Proteins including IgG, IgM, and albumin were low (IgG 228 mg/dL [reference range 650–1,600 mg/dL], IgM 41 mg/dL [reference range 50–300 mg/dL], albumin 1.7 g/dL [reference range 3.2–4.8 g/dL]), yet she displayed no signs of malnutrition, proteinuria, or synthetic liver dysfunction to explain the low protein levels. PLE was diagnosed with an elevated fecal alpha-1 antitrypsin (A1AT) clearance of 63.3 mL/day (positive >56 mL/day). Esophagogastroduodenoscopy at symptom onset showed esophagitis, erosive gastritis, and ulcerative duodenitis (Figure 1). Histopathology revealed chronic esophageal inflammation, erosive gastric antral mucosa without Helicobacter pylori, and ulcerative duodenitis with increased intraepithelial lymphocytes. Comprehensive evaluation for the underlying etiology of PLE returned with positive CMV testing (CMV IgM 62.9 AU/mL [positive >34.9 AU/mL], CMV IgG 2.4 U/mL [positive >0.69 U/mL], CMV quantitative DNA polymerase chain reaction 46,100 IU/mL [positive >200 IU/mL]). She was diagnosed with PLE due to CMV, which was later confirmed by CMV-specific immunohistochemistry (Figure 2). CMV immunohistochemical staining was positive only in duodenal tissue, though colonoscopy was not performed. She completed 3 weeks of valganciclovir with resolution of her symptoms. Follow-up laboratory studies demonstrated resolution of leukocytosis (5.3 × 10^3^/μL), normalization of albumin (3.6 g/dL) and IgM levels (57 mg/dL), and undetectable CMV DNA by polymerase chain reaction. IgG levels remained mildly decreased but showed significant improvement (523 mg/dL). Repeat endoscopy showed only mild duodenitis with no erosions or ulcerations (Figure 3).
Erythema, erosions, friability, white plaques, ulceration, and scalloped folds in the whole examined duodenum compatible with ulcerative duodenitis.
Immunohistochemical staining demonstrating cytomegalovirus-positive cells within the duodenal lamina propria (original magnification ×400).
Mild erythema of the duodenum after valganciclovir treatment.
DISCUSSION
In healthy individuals, the daily loss of protein through the gastrointestinal tract plays a minor role in overall protein metabolism; it contributes to only 1%–2% of the total serum protein and less than 10% of the total albumin pool.^15^ However, in cases of PLE, gastrointestinal protein loss can reach up to 60% of the total albumin levels. Serum proteins most impacted by this process are those with slower turnover rates, including albumin, immunoglobulins, and ceruloplasmin. Longer half-lives prevent compensation for such losses.^16^
Diagnosis of PLE begins with exclusion of more common causes of hypoproteinemia, including malnutrition, hepatic disease, and renal disease. Once these potential causes are ruled out, an A1AT clearance can be measured. A1AT is a protein synthesized in the liver that is not actively secreted or absorbed, it has a molecular weight similar to albumin, and it remains intact as it passes through the gastrointestinal tract. These properties allow for detection in feces. Normal A1AT clearance is less than or equal to 21 mL/day or less than or equal to 56 mL/day with diarrhea. An increase in A1AT clearance is indicative of PLE.^1^
CMV-associated PLE in immunocompetent adults is seldom reported. The gold standard for diagnosis of CMV-related gastrointestinal disease relies on immunohistopathology. Gastrointestinal disease may be focal and patchy, so multiple biopsies may be needed to confirm the diagnosis. In addition, visualization of CMV inclusion bodies necessitates that tissue biopsies be taken from the ulcer edge or base and, therefore, is easily missed. Serum CMV testing may assist with early detection and monitoring of response to therapy if positive, but immunohistopathology remains the gold standard for diagnosis.^17^
The treatment of PLE typically includes dietary supplementation and treatment of the underlying disease. While treatment with antivirals is recommended for CMV enteritis in immunocompromised individuals, its role in immunocompetent individuals is not well defined. A majority of immunocompetent patients with CMV disease recover without intervention. Symptomatic and supportive nutritional therapy such as antinausea medications, electrolyte replacement, and a high-protein diet often result in improvement of symptoms.^6^ In similar cases of CMV-associated PLE, patients' symptoms resolved after 2 to 4 months of supportive treatment.^2,5,6,9,11–13^ Practically, the severity of CMV disease must be balanced against the risk of medication toxicity. In severe disease that is nonresponsive to supportive treatment, patients may benefit from antiviral therapy. In our case, the patient's CMV disease required hospitalization with persistent electrolyte derangements, thus antiviral treatment was initiated with significant clinical improvement.
In conclusion, CMV-associated PLE may occur in immunocompetent adults and manifest as anasarca with severe and prolonged gastrointestinal symptoms. Prompt recognition of anasarca with concurrent low serum protein levels as manifestations of a PLE will hasten diagnosis of CMV-associated enteritis and enhance patient outcomes.
DISCLOSURES
Author contributions: N. Mayer participated in patient care, reviewed the literature, and contributed to the writing of the manuscript. N. Bhargava, D. Patel, M. Kaplan, and V. Kata participated in patient care and reviewed and edited of the manuscript. D. Errampalli and T. O'Connor contributed to patient care, endoscopic evaluation of the patient, and reviewed and edited of the manuscript. T. Betlej evaluated the pathology slides and reviewed and edited of the manuscript. N. Bhargava is the article guarantor.
Financial disclosure: The authors have no conflicts of interest to declare.
Previous presentation: Presented as a poster at the ACG 2024 Annual Scientific Meeting, October 2024, Philadelphia, PA.
Informed consent was obtained for this case report.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Umar SB Di Baise JK. Protein-losing enteropathy: Case illustrations and clinical review. Am J Gastroenterol. 2010;105(1):43–50.19789526 10.1038/ajg.2009.561 · doi ↗ · pubmed ↗
- 2Ciavaldini A Delattre C Bousquet A Entéropathie exsudative sévère compliquant une primo-infection à cytomégalovirus chez un adulte immunocompétent [Severe cytomegalovirus-associated protein losing gastropathy in an immunocompetent adult]. Rev Med Interne. 2023;44(4):195–8.36639308 10.1016/j.revmed.2022.12.006 · doi ↗ · pubmed ↗
- 3Yasuoka K Fujikawa H Shibazaki S. Cytomegalovirus enteritis: A surprising cause of severe diarrhoea and protein-losing gastroenteropathy in an intensive care patient. BMJ Case Rep. 2022;15(4):e 249258.10.1136/bcr-2022-249258 PMC 903616835459653 · doi ↗ · pubmed ↗
- 4Ochiai Y Hoteya S Kono K Takazawa Y Matsui A Kikuchi D. Cytomegalovirus ileitis with protein-losing enteropathy in an immunocompetent adult. Clin J Gastroenterol. 2021;14(4):1060–6.33745065 10.1007/s 12328-021-01382-x · doi ↗ · pubmed ↗
- 5Perrineau S Cazals-Hatem D Zarrouk V Fantin B de Lastours V. Cytomegalovirus-associated protein-losing enteropathy in a healthy man. Med Mal Infect. 2017;47(8):562–5.28802763 10.1016/j.medmal.2017.07.003 · doi ↗ · pubmed ↗
- 6Lalazar G Doviner V Ben-Chetrit E. Clinical problem-solving. Unfolding the diagnosis. N Engl J Med. 2014;370(14):1344–8.24693895 10.1056/NEJ Mcps 1300859 · doi ↗ · pubmed ↗
- 7Chen S Lalazar G Barak O Adar T Doviner V Mizrahi M. Protein-loosing entropathy induced by unique combination of CMV and HP in an immunocompetent patient. Case Rep Med. 2012;2012:361892.23197985 10.1155/2012/361892 PMC 3502835 · doi ↗ · pubmed ↗
- 8Engjom T Larsen KK Hove O Gilja OH. En ung mann med akutte generaliserte ødemer [A young man with acute, generalised oedema]. Tidsskr Nor Laegeforen. 2010;130(16):1627–9.20805862 10.4045/tidsskr.09.0771 · doi ↗ · pubmed ↗