The resource requirements of perioperative patient warming in German hospitals – the results of a prospective, multicenter activity-based costing study
Stefan Nardi-Hiebl, Jan Wallenborn, Martin Schniertshauer, Tilo Koch, Tobias Gruebl, Alexander Torossian

TL;DR
This study examines the costs and resource use of keeping patients warm during surgery in German hospitals, finding significant variation in expenses and practices.
Contribution
The study introduces a multicenter activity-based costing approach to quantify resource requirements for perioperative warming in hospitals.
Findings
Perioperative warming costs per patient varied from EUR 3.52 to EUR 49.26 across four German hospitals.
Nurses contributed most of the time required for warming activities, with forced-air warming being the primary method used.
Cost variations were influenced by institutional infrastructure, workflow efficiency, and patient case mix.
Abstract
Perioperative warming is essential in preventing hypothermia during surgery, a condition linked to adverse outcomes like increased infection rates, impaired coagulation, and extended hospital stays. Despite the availability of various active warming methods, such as forced-air warming (FAW) and electric warming systems, their implementation and associated costs vary significantly across hospitals, impacting resource allocation and patient care. This study used a prospective, multicenter, activity-based costing approach across four German hospitals with diverse capacities. The activity-based costing model identified and measured staff time, material use, and direct costs linked to perioperative warming processes in a sample of 225 surgical patients. Warming processes were assessed across stages, including pre-warming, intraoperative warming, and post-anesthesia care. Findings show…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
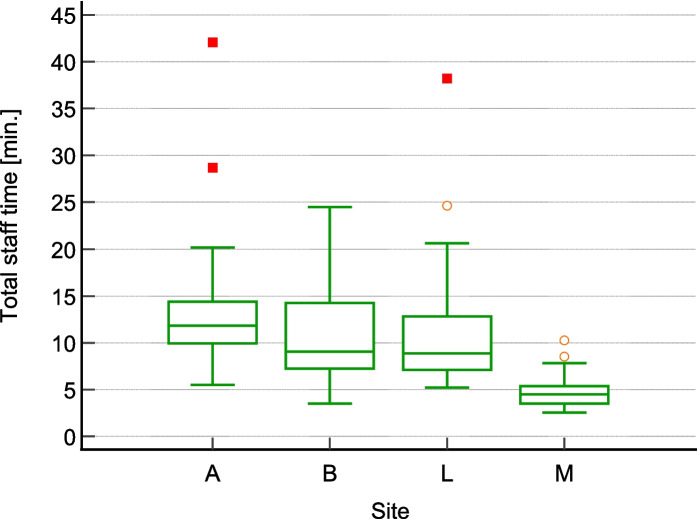 Figure 1
Figure 1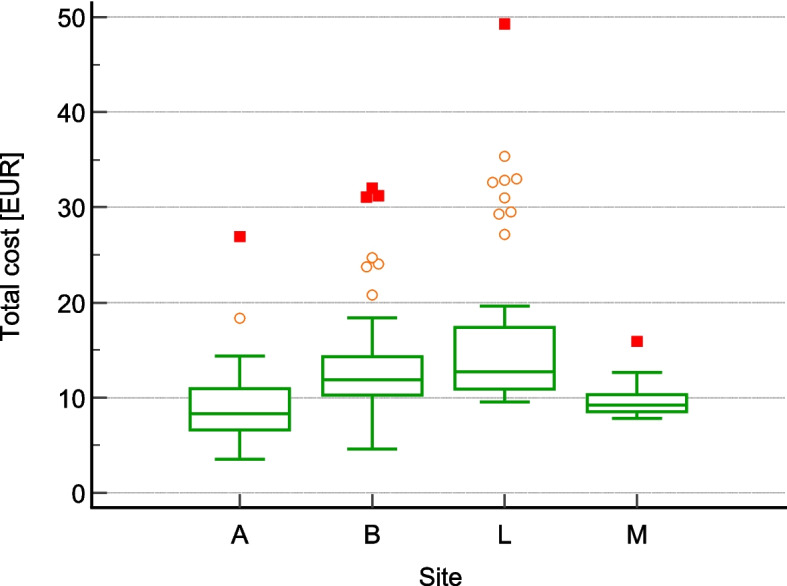 Figure 2
Figure 2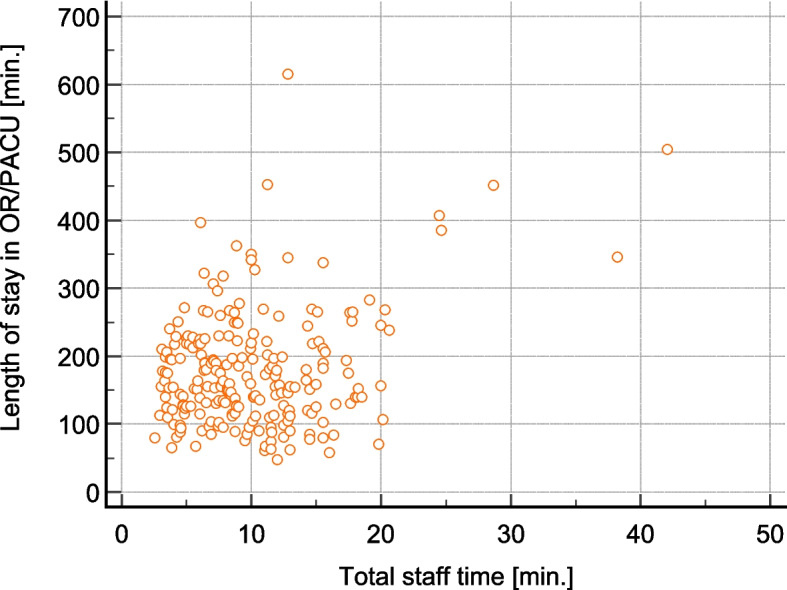 Figure 3
Figure 3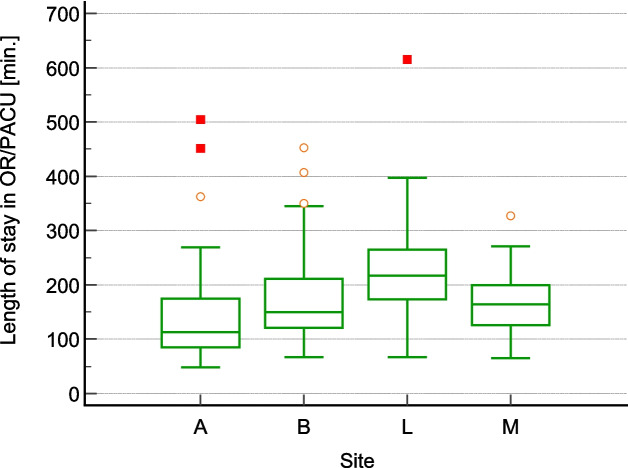 Figure 4
Figure 4- —Mölnlyke Healthcare
- —Philipps-Universität Marburg (1009)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsClimate Change and Health Impacts · Thermal Regulation in Medicine · Thermoregulation and physiological responses
Introduction
Perioperative patient warming is a crucial aspect of surgical care, primarily aimed at preventing inadvertent perioperative hypothermia—a common and significant complication in surgical patients. This condition, defined as a core body temperature below 36 °C, can lead to a range of adverse outcomes, including increased rates of surgical site infections, impaired coagulation, increased blood loss, prolonged hospital stays, and higher incidences of morbid cardiac events [10]. Anesthesiologists play a pivotal role in the implementation and management of perioperative warming strategies to mitigate these risks.
Inadvertent perioperative hypothermia occurs due to the suppression of thermoregulatory control by anesthetics, the exposure of large body surface areas during surgery, and the infusion of unwarmed intravenous fluids [3]. Various active warming systems, including forced-air warming (FAW), resistive heating, and circulating-water systems, have been developed and studied extensively to counteract these effects. Among these, FAW systems have apparently been most widely adopted and are considered highly effective [8].
The importance of active warming extends beyond temperature regulation. Active body surface warming (ABSW) systems not only maintained normothermia but also reduce shivering, and blood transfusion requirements, while improving patient satisfaction and reducing the incidence of surgical wound infections, although not affecting post-operative pain [2]. These findings underscore the multifaceted benefits of effective warming strategies in the perioperative setting.
Despite the evident benefits of perioperative warming, the prevalence of hypothermia remains high. Alfonsi et al. report that 53.5% of patients were hypothermic upon admission to the recovery room, despite the use of warming devices [1]. The study also emphasized that the combination of pre-warming and intraoperative warming was significantly more effective in preventing hypothermia than intraoperative warming alone.
In Germany, the situation mirrors the global challenge of maintaining normothermia during surgery. Gabriel et al. explored the acceptance and implementation of perioperative warming guidelines in German hospitals [7]. The study revealed that while there is a high acceptance of the German S3 Guidelines [13], which recommend strategies like pre-warming and sublingual temperature measurement, the implementation varies significantly across hospitals. Despite these variations, the study found that hospitals generally succeeded in maintaining normothermia in patients, with no postoperative hypothermia detected in a cohort of 431 patients. This highlights the importance of consistent application of warming strategies across different healthcare settings.
However, with the current budget restraints in many healthcare systems proven cost-effectiveness is a critical factor in the adoption of perioperative warming strategies. The implementation of effective warming techniques might lead to cost savings by reducing complications associated with hypothermia. Studies have shown that maintaining normothermia can decrease the incidence of surgical site infections, reduce the need for blood transfusions, and shorten hospital stays, all of which have the potential to contribute to lower healthcare costs [6, 9, 11].
While lower overall healthcare costs are beneficial for the entire system, the direct costs of patient warming play a crucial role for decision making on a hospital level as they constitute a real cash out. Warming strategies are associated with direct costs items, like equipment, consumables, maintenance and operations, implementation and finally labor. To our knowledge there has been no transparency about these cost items related to perioperative patient warming.
We hereby present the results of a prospective, multi-center activity-based costing study along the surgical patient process to collect and to analyze associated activities and cost items. The result of the study illustrates the typical resource requirements and direct costs for perioperative patient warming using various warming strategies.
Materials and methods
The protocol was reviewed by the Institutional Review Board of the University of Marburg, Germany and approved the study as outlined (Ref. 19312). Subsequently, the study was conducted at four German hospitals by applying an activity-based evaluation approach.
Selection of study centers
The selection of the study centers was based on their availability for such a study. We considered status of the implementation of patient warming processes according to the respective German S3 guideline. In addition, the bed capacity which broadly reflects the German hospital landscape (from a university hospital with almost 1.140 beds, a large community hospital with 1.402 beds as well as two mid-sized community hospital with 592 beds and 603 beds in private ownership (Table 1) were also taken into account. Three hospitals used pre-warmed blankets and FAW, one hospital employed an electric warming system. All hospitals use infusion warming systems (Table 2). Table 1. Study sites metadataData itemHospital AHospital BHospital LHospital MNo of beds5926031,4021,140TypeRegular CareRegular CareMaximum CareAcademicInpatient cases per annum24,10013,17044,00043,000Surgeries per annum12,0009,40010,90019,000No. of operating rooms (OR)1061030Average OR temperature21 deg C21.5 deg C21 deg C21 deg CTable 2Available warming technologiesAreaHospital AHospital BHospital LHospital MWard -Pre-surgeryn/an/an/an/aOR—Bed holding arean/aPWB/PWGMPWBPWBOR – Induction areaEWSWI/partially PWBWI/partially PWBWI/partially PWBOR—SurgeryFAW/WIFAW/WIFAW/WIFAW/WIPACUFAWPWB/FAWPWB/FAWPWB/FAWWard—Post-surgeryn/an/an/an/aPWB Pre-warmed blanket, PWGM Pre-warmed gel mattress, WI Warm infusionFAW Forced-air warming, EWS Electric warming system
Study design
The study aim was restricted to resource and cost analysis; the clinical effectiveness of the various warming strategies was outside the scope of this work. The study was conducted using an activity-based costing (ABC) approach, in which relevant activities along a defined clinical process are identified, and the associated resource requirements—such as staff time and material costs—are systematically measured and recorded [4]. In the context of perioperative patient warming, ABC facilitates a structured economic analysis by allocating costs to distinct cost pools and identifying corresponding cost drivers. Typical cost pools include capital investment and maintenance for warming equipment (e.g., forced-air warming systems, fluid warmers), expenditures for single-use consumables, staff time required for setup and intraoperative management, energy consumption, and training related to protocol implementation. Key cost drivers may encompass the number and duration of procedures requiring active warming, the warming modality employed, patient-specific risk factors, adherence to institutional protocols, and perioperative staffing ratios.
To define the warming process at each hospital site, structured workshops were conducted with representatives from anesthesiology, surgery, operating room (OR) staff, and inpatient wards. These sessions served to map the perioperative warming workflow and identify cost pools, cost drivers, activities or activity phases with substantial impact on resource consumption. The findings were synthesized into a unified process model comprising six sequential phases: Ward (preoperative), OR arrival, Anesthesia, Surgery, Post-Anesthesia Care Unit (PACU), and Ward (postoperative). Specific roles and corresponding data points were assigned to each phase. Processes related to procurement, equipment maintenance, and staff training were not included in the analysis. The primary reason for this exclusion was uncertainty regarding whether a sufficiently large sample size for these activities at each hospital site could be obtained to generate meaningful data.
Data collection
Based on the process model, an activity recording form (ARF) was developed to collect the resource requirements along the generalized process. The generalized process outlines all with patient warming associated activities a patient might encounter – from passing from the ward to the OR, receiving anesthesia, undergoing surgery, staying in the PACU and returning to the ward. For the identified activities along this process, the material used, and time stamps were recorded using the ARF. Based on these time stamps the duration of the selected activities were calculated in seconds. The ARF also distinguished between the two different professional roles, nurses and physicians, and offered the opportunity to record deviations from the standard process. The ARFs were made available in paper form to staff at the study sites responsible for patient-warming. Subsequently, the staff was also responsible for documentation. Involved staff were trained in the study concept and the ARF.
A patient was included in the study, when the patient was admitted as an inpatient, received surgery involving patient warming procedures and was under treatment of the nurses trained for the study. Only patients older than 18 years were considered. No further inclusion or exclusion criteria were defined. A pre-study sample size calculation was not conducted as meaningful input figures were not available. Therefore, we decided to collect at least 200 measurements.
Staff costs were calculated based on actual cost data from the four hospitals, averaged across all seniority levels but proportionally weighted. This yielded an average cost of EUR 0.64 per minute for nursing staff and EUR 0.84 per minute for physicians. Material costs, also averaged across the four hospitals, amounted to EUR 5.20 for one FAW blanket, EUR 1.00 for one cotton blanket, and EUR 13.40 for one HOTLINE® infusion system.
Statistical evaluation
All data of the paper-based ARFs was recorded in a Microsoft® Access database (Microsoft® Corporation, Redmond, United States), crosschecked and transferred to the statistical software. All calculations were conducted using MedCalc® Statistical Software version 23.2.6 (MedCalc Software Ltd, Ostend, Belgium). Descriptive statistics, including means, medians, and standard deviations, were used to summarize the data. Statistical significance was determined using the Kruskal–Wallis test for all comparisons, Conover post-hoc analysis and a significance level of p < 0.05. Correlation factors were determined by Spearman’s ρ.
Results
Data from 278 patient sequences were collected, whereby a (patient) sequence was defined as one passage of one patient through the entire generalized process. 53 patient sequences were excluded from data analysis because the ARFs were not entirely completed. The primary cause for non-completion of the ARFs was an emergency or other activities which required the documenting staff to refocus on other aspects. In total, 225 ARFs complied with all formal requirements and thus 225 patient sequences were analyzed. Two hospitals provided 53 completed ARFs each, one hospital 41 and the fourth hospital 78 completed ARFs.
The 225 patient sequences involved 107 male and 118 female patients with an average age of 63 years. Most patients underwent musculoskeletal surgery (88 patients, 39.1%), followed by surgery of the digestive system (35 patients, 15.6%) and surgery of the female productive system (18 patients, 8%) (Table 3). Table 3ARFs statisticsData itemHospital AHospital BHospital LHospital MNo of ARFs collected67886558No. of ARFs completed53785341Average age of patients (years)67.062.365.157.0Gender (male/female)30 m23 f33 m45 f34 m19 f10 m31 fType of surgeries (more than 10 surgeries)1. Urogenital2. Musculoskeletal3. Vascular1. Digestive2. Musculoskeletal1. Musculoskeletal2. Male reproductive system1. Female breast2. Female reproductive system
The overall average for total staff time required for patient warming is 10.09 min (minimum = 2.53 min, maximum = 42.08 min, s = 5.52 min) (Table 4). Nurses contribute the majority of staff time dedicated to patient warming with an average of 9.91 min, whereas physicians make a much lower contribution, averaging 0.19 min. The results for total staff time across all four hospitals differ significantly. Hospitals A and M's results differ markedly from the others, while those of Hospitals B and L do not show a significant difference (Fig. 1). Table 4. ResultsData itemHospital AHospital BHospital LHospital MOverall averageTotal staff time (min.) – Average12.9210.4510.914.7110.09Total staff time(min.)—Minimum5.53.55.22.53*-Total staff time(min.) – Maximum42.0824.538.1310.25-Total staff time(min.) – StdDev5.684.605.851.635.53Nurse(min.)12.8910.0210.904.559.91Physician(min.)0.280.430.010.160.19Total material cost (EUR) – Average0.906.249.436.595.80Total cost (EUR) – Average9.1713.0116.419.6312.29Total cost (EUR) – Minimum3.524.599.537.82-Total cost (EUR) – Maximum26.9332.0549.2615.91-Total cost (EUR)—StdDev3.885.418.511.506.21*Share of material cost in Total Cost—Average9.8%48.0%57.5%68.4%*46.0%*Share of Nurse cost in Total Cost – Average90.0%49.2%42.5%30.2%*53.0%*Fig. 1. Box-whisker plot “Total staff time required”
Material costs average EUR 5.80 per sequence, with total average costs at EUR 12.29 per sequence. The minimum and maximum total costs are EUR 3.52 and EUR 49.26 (s = 6.21) (Table 4). Comparing the total cost, the results of Hospital B and L differ significantly from the others, while the results of Hospitals A and M show no significant difference (Fig. 2).Fig. 2. Box-whisker plot “Total cost of patient warming”
During the 225 sequences recorded, 158 FAW blankets, 309 cotton blankets and 13 infusion warming systems were used. Each patient received at least one pre-warmed cotton blanket; at hospital A each patient was warmed with the electric warming system. All patients in hospitals L and M also were treated by FAW (Table 5). On average, the time interval between intubation and extubation was 148 min, the average time spent in PACU was 123 min (Table 6). Regarding the intubation/extubation time interval, hospitals A and L each differ significantly from all the other hospitals, while hospitals B and M don’t differ significantly from each other. The PACU time of hospital A differs significantly from hospital M, hospital B differs significantly from hospital L and M and hospital L just from hospital B. Table 5. Material statisticsData itemHospital AHospital BHospital LHospital MNo. of patients (Sample)53785341No. of patients receiving PWBn/a78(194 blankets)53(57 blankets)41(58 blankets)No. of patients receiving EWS53n/an/an/aNo. of patients receiving FAW746(55 covers)53(57 covers)41(46 covers)No. of patients receiving WI0490Table 6Time statisticsData itemHospital AHospital BHospital LHospital MOverall averageNo. of patients (Sample)53785341Time interval between intubation and extubation (min.)Average118144197133148Minimum23507648***-Maximum460420592280-StdDev82.7872.2186.2051.7973.25Time spent in PACU (min.)Average10989122172123Minimum0008-Maximum288280255501-StdDev49.1668.2753.10115.0171.38***
There is no observed correlation between the duration of a patient’s stay in the OR/PACU area and the total staff time required for patient warming (Fig. 3). However, the time from admission to discharge in the OR/PACU area differs significantly among the hospitals (Fig. 4).Fig. 3. Correlation plot “Stay at OR/PACU area vs. total staff time”Fig. 4. Box-whisker plot “Stay at OR/PACU area per site”
Discussion
This study presents the direct cost of implementing perioperative warming strategies in diverse hospital settings. Our findings underscore the resource variability required across institutions, with marked differences in material costs and staff time, particularly among hospitals with varying care capacities and resources. The wide range in total costs per patient—from EUR 3.52 to EUR 49.26—illustrates the impact of individualized institutional practices or a specific situation on expenditure, a factor that may influence decision makers’ inclination for specific warming technologies. Our study adds a nuanced perspective by detailing the direct cost impact of these protocols, showing that although comprehensive warming is beneficial, its financial feasibility remains potentially a barrier, particularly for institutions with limited budgets in the current budget climate. Considering the direct costs is important as aggressive warming could improve operating room efficiency. However, the economic benefits are significantly influenced by factors such as staff costs and the price of forced-air warming devices [12].
lthough all hospitals can make use of forced-air warming (FAW), the variations in FAW application and reliance on supplemental warming strategies reflect a lack of standardization in perioperative warming practices. This disparity in practice may lead to uneven patient outcomes, as hospitals with higher staff costs and longer warming durations might be able to achieve greater consistency in normothermia, while others could face limitations in the level of care due to resource constraints. The variation in staff time, particularly among nurses, further underscores the critical role nursing staff play in patient warming and points to the need for streamlined workflows to reduce time burden without compromising care.
The results show significant variability in resource requirements across the four hospitals, with total staff time for perioperative warming ranging from an average of 4.71 min at Hospital M to 12.92 min at Hospital A, and total costs per sequence ranging from €3.52 to €49.26. These discrepancies likely stem from differences in institutional infrastructure, workflow efficiency, and adherence to guidelines, but a specific reason could not be identified. For instance, hospitals with larger capacities and more advanced facilities, such as those equipped with pre-warming protocols and continuous temperature monitoring, tend to incur higher initial costs but may achieve better long-term patient outcomes. Conversely, smaller hospitals with fewer resources may rely more on manual processes or less efficient equipment, resulting in lower immediate costs but potentially higher rates of hypothermia-related complications. However, it must be noted that the study did not record patient-related co-morbidities or complications. Therefore, a suggested relationship between hospital size, resource level, and complication rates is hypothetical and cannot be reliably established based on the available data.
Our data confirm that material expenditure for peri-operative warming is lowest in Hospital A, which relies almost exclusively on electric warming sheets (EWS). However, Hospital A also performs a disproportionately high share of brief procedures, for which many centers forego FAW altogether. Consequently, the apparently favorable cost profile may be a function of case mix rather than inherent efficiency of EWS.
The hospitals reported partially high values for the maximum total staff time. In the case of Hospital A, this reached 42 min, which appears unusual for patient-warming activities alone. These high values were primarily caused by technical issues with the warming systems, where staff either attempted (and succeeded) to fix a fault themselves or arranged for a replacement system. Consequently, we have also recorded these rare but certainly possible occurrences. Whether the elevated staff time in Hospital A’s case is related to the use of EWS can’t be determined from the data. Also, the fact, that hospitals A and L show the highest values for staff time but also for the time interval between intubation and extubation could explain the observation.
But also variations in nursing staff availability and workload play a critical role, as shown by the high proportion of time nurses contribute to warming activities. Moreover, differences in training and familiarity with warming protocols can further amplify disparities. These findings can also serve as a benchmark to evaluate internal processes and encourage the adoption of"best-practice learning"—the transfer of evidence-based approaches tailored to specific resource constraints and capacities.
One noteworthy finding is the absence of a direct correlation between the total duration of warming and the length of stay in the OR or PACU, suggesting that while warming is essential, extending the time invested in warming activities may not significantly affect the immediate perioperative timeline. As such, we think, that the insight calls attention to the need for balancing warming efficiency with workflow demands, especially in high-turnover environments. Further research could explore optimal warming times and methods that maintain efficacy without unnecessarily increasing the patient’s OR time. It should be noted that we have not recorded whether a patient was kept longer or shorter in the PACU, for example due to bed shortages on the ward or PACU capacity constraints. However, a retrospective cursory assessment of the individual times spent in the PACU did not reveal any indications that patients included in the study were affected by such circumstances.
The environmental implications of warming practices merit attention. The widespread use of disposable materials, such as FAW blankets, contributes to medical waste, raising concerns about sustainability. In light of global efforts to reduce the environmental footprint of healthcare, exploring sustainable alternatives is crucial. Studies have shown that reusable devices, potentially also warming tools, while associated with higher initial costs, can reduce waste and long-term expenses [5]. Policymakers and hospital administrators might want to consider research and investment in environmentally friendly solutions that balance efficacy, cost, and sustainability.
This study reinforces the importance of perioperative warming process efficiency while highlighting the challenges associated with its widespread, consistent application. By providing a detailed cost analysis, we offer insights that can inform departmental heads and hospital administrators in the development of financially sustainable warming protocols that do not compromise patient outcomes. Further research focusing on cost-optimization strategies, combined with clinical efficacy studies, is essential to achieving the dual goals of resource efficiency and improved patient care in perioperative settings.
While the activity-based costing model employed in this study offers detailed insights into resource use, it has inherent limitations. For instance, it does not account for indirect costs such as staff training, equipment maintenance, or environmental impacts. Furthermore, reliance on self-reported data introduces the potential for bias, particularly in high-stress environments where documentation may be deprioritized. Regional and institutional variations, such as differences in staffing models and infrastructure, also limit the generalizability of our findings. Future studies should consider these factors to provide a more comprehensive understanding of the financial and operational aspects of perioperative warming.
It is important to note that we did not capture any patient-level temperature outcome, precluding a full cost-effectiveness analysis. Second, marked heterogeneity in case length—particularly the cluster of short operations in Hospital A—introduces confounding, because staff time and warming material use do not scale linearly with duration. Third, institutional policies (e.g. “no FAW for cases < 1 h”) were not formally documented and could not be adjusted for. These factors limit the generalizability of the absolute cost figures.
In addition, this study was conducted within the context of the German hospital system. Given the potential variability in costs and clinical workflows across different countries, a European multi-center study would be valuable to enable international comparisons of patient warming practices. Such an approach would not only facilitate the identification of context-specific strategies but also support the development of evidence-based best practices that could be adapted and implemented within individual hospital environments.
Conclusion
The study illustrates the significant variability in workload and direct costs of patient warming across various hospital settings. The results can serve as input for the overall health-economic equation when assessing the cost-effectiveness of patient-warming strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Campbell, Gillian, Phil Alderson, Andrew F. Smith, and Sheryl Warttig. 2015. ‘Warming of Intravenous and Irrigation Fluids for Preventing Inadvertent Perioperative Hypothermia’. Cochrane Database of Systematic Reviews, no. 4. 10.1002/14651858.CD 009891.pub 2.10.1002/14651858.CD 009891.pub 2PMC 676917825866139 · doi ↗ · pubmed ↗
- 2Cohen, Eva S., Sarah Djufri, Selma Bons, Mike. R. Knoppert, Wouter J. K. Hehenkamp, Lisanne H. J. A. Kouwenberg, and Nicolaas H. Sperna Weiland. 2023. ‘Environmental Impact Assessment of Reusable and Disposable Surgical Head Covers’. JAMA Surgery 158 (11): 1216–17. 10.1001/jamasurg.2023.3863.10.1001/jamasurg.2023.3863 PMC 1048337737672247 · doi ↗ · pubmed ↗
- 3Gabriel, Philip, Jan Höcker, Markus Steinfath, Kevin R. Kutschick, Jana Lubinska, and Ernst-Peter Horn. 2019. ‘Prevention of Inadvertent Perioperative Hypothermia – Guideline Compliance in German Hospitals’. GMS German Medical Science 17 (July):Doc 07. 10.3205/000273.10.3205/000273 PMC 673274631523222 · doi ↗ · pubmed ↗
- 4Harper, C. M., J. C. Andrzejowski, and R. Alexander. 2008. ‘NICE and Warm’. BJA: British Journal of Anaesthesia 101 (3): 293–95. 10.1093/bja/aen 233.10.1093/bja/aen 23318710834 · doi ↗ · pubmed ↗
- 5Song, Shujia, Lijian Pei, Hongda Chen, Yuelun Zhang, Chen Sun, Jie Yi, and Yuguang Huang. 2023. ‘Analysis of Hospital and Payer Costs of Care: Aggressive Warming versus Routine Warming in Abdominal Major Surgery’. Frontiers in Public Health 11 (November). 10.3389/fpubh.2023.1256254.10.3389/fpubh.2023.1256254 PMC 1065278238026375 · doi ↗ · pubmed ↗
- 6Torossian, Alexander, K Becke, B Bein, A Bräuer, D Gantert, R Greif, J Höcker, EP Horn, O Kimberger, and E Klar. 2019. ‘S 3 Leitlinie “Vermeidung von Perioperativer Hypothermie”—Aktualisierung. 2019’. AWMF Online. AWMF-Register, no. 001/018.