Tumor Rupture in a Patient with Recurrent Hepatocellular Carcinoma Following Atezolizumab plus Bevacizumab: A Case Report
Kazuhiro Tada, Shohei Yoshiya, Takaaki Mori, Ryoichi Narita, Kentaro Iwaki, Sota Nakamura, Yasunari Yamada, Hajime Takaki, Yo-ichi Yamashita, Kengo Fukuzawa

TL;DR
A patient with liver cancer experienced a rare tumor rupture after receiving atezolizumab and bevacizumab, which was successfully treated with arterial embolization.
Contribution
This is the first reported case of HCC rupture following atezolizumab plus bevacizumab therapy.
Findings
Tumor rupture occurred in a patient with recurrent HCC after the first cycle of atezo-bev.
The patient was successfully managed with transcatheter arterial embolization.
No further tumor bleeding occurred after resuming atezo-bev treatment.
Abstract
Atezolizumab plus bevacizumab combination therapy (atezo-bev) has been widely used worldwide as the first-line treatment for unresectable hepatocellular carcinoma (HCC). Intratumoral hemorrhage has been reported as a rare adverse event of atezo-bev. However, no previous cases of HCC rupture during atezo-bev have been reported. Herein, we demonstrate a case of tumor rupture in a patient with recurrent HCC following atezo-bev, who was successfully managed with transcatheter arterial embolization (TAE). An 80-year-old man with multiple recurrent HCCs (at least 4 lesions with a maximum tumor diameter of 35 mm protruding from the liver surface) developed epigastralgia immediately after the first cycle of atezo-bev. CT revealed a ruptured HCC in the left lateral lobe. TAE was performed, and the patient continued to receive atezo-bev without any subsequent tumor bleeding. Tumor rupture…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
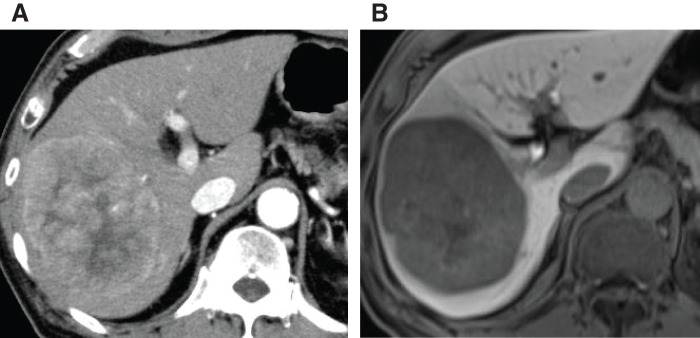 Fig. 1
Fig. 1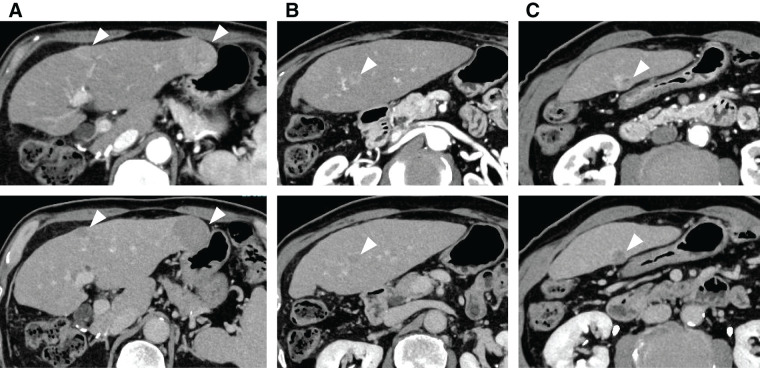 Fig. 2
Fig. 2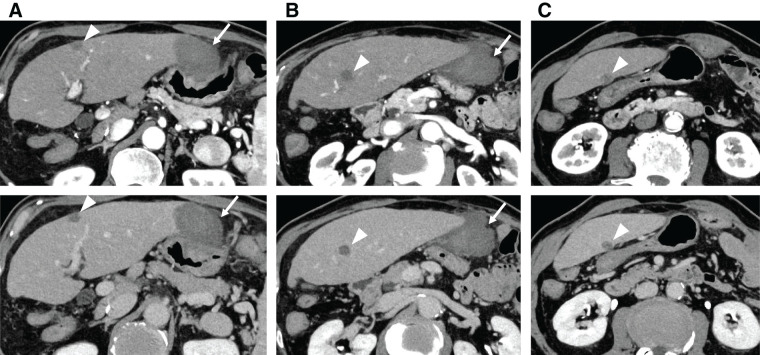 Fig. 3
Fig. 3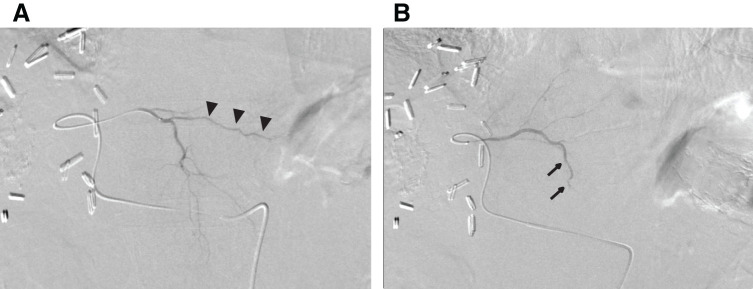 Fig. 4
Fig. 4| Before TAE | After TAE | |
|---|---|---|
| WBC (/mm3) | 6200 | 6800 |
| RBC (/mm3) | 426 × 104 | 425 × 104 |
| Hemoglobin (g/dL) | 13.5 | 13.4 |
| Hematocrit (%) | 40.2 | 40.3 |
| Platelets (/mm3) | 16.3 × 104 | 13.3 × 104 |
| AST (U/L) | 39 | 43 |
| ALT (U/L) | 30 | 32 |
| LDH (U/L) | 304 | 275 |
| GGT (U/L) | 198 | 179 |
| ALP (U/L) | 135 | 135 |
| Total bilirubin (mg/dL) | 0.8 | 0.8 |
| BUN (mg/dL) | 12 | 13 |
| Creatinine (mg/dL) | 0.66 | 0.6 |
| CRP (mg/dL) | 4.4 | 2.6 |
| Alb (g/dL) | 3.0 | 2.8 |
| PT (%) | 80.3 | 78.8 |
| ALBI score | −1.80 | −1.63 |
| HBs antigen | Negative | — |
| Anti-HCV (S/CO) | 0.04 | — |
| Reference | Year | Symptom | Bleeding point | Rupture | Treatment for | Prognosis | Follow-up |
|---|---|---|---|---|---|---|---|
| Mitsuyama et al. | 2023 | Fatigue | Rib metastasis from HCC | No | TAE | Survived | Atezo-bev |
| Park et al. | 2024 | Abdominal pain | Intratumoral hemorrhage | No | TAE | Died due to liver failure | – |
| Our case | 2025 | Epigastric discomfort | Intratumoral hemorrhage | Yes | TAE | Survived | Atezo-bev |
| Before atezo-bev | After 1st cycle of atezo-bev | |
|---|---|---|
| AFP (ng/mL) | 2824 | 159 |
| DCP (mAU/mL) | 42.9 | 17.5 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHepatocellular Carcinoma Treatment and Prognosis · Hepatitis C virus research · Lymphoma Diagnosis and Treatment
Abbreviations
atezo-bev atezolizumab plus bevacizumab therapy HCC hepatocellular carcinoma ICI immune checkpoint inhibitor TACE transcatheter arterial chemoembolization TAE transcatheter arterial embolization VEGF vascular endothelial growth factor
INTRODUCTION
The global phase 3 trial (IMbrave150) demonstrated that atezolizumab plus bevacizumab combination therapy (atezo-bev) had greater benefits than did sorafenib therapy in patients with unresectable hepatocellular carcinoma (HCC).^1)^ Since then, atezo-bev has been recommended as the first-line treatment for advanced HCC.^2)^ However, several adverse events associated with this combination therapy have also been reported. Bleeding is a well-known adverse reaction of bevacizumab.^3)^ The incidence of bleeding events was reported to be 7% in patients receiving atezo-bev compared to 4.5% in those receiving sorafenib therapy.^1)^ Although gastrointestinal bleeding is a common complication, atezo-bev-induced tumor bleeding is relatively rare. Moreover, no previous study has reported tumor rupture during atezo-bev therapy.
Herein, we report a case of tumor rupture in a patient with recurrent HCC following atezo-bev, which was successfully managed with transcatheter arterial embolization (TAE) using gelatin sponge particles.
CASE PRESENTATION
An 80-year-old man with a history of alcoholic hepatitis underwent a laparoscopic right hemihepatectomy for a large HCC (Fig. 1). Histological examination of the resected specimen revealed a moderately to poorly differentiated simple nodular HCC with extranodal growth. The microvascular invasion statuses were vp0, vv1, and va0. No intrahepatic metastases or bile duct infiltration were observed. Six months later, contrast-enhanced CT scans revealed multiple recurrent HCCs in the left lobe (Fig. 2). Liver function was well preserved, categorized as Child–Pugh class A (6 points) and ALBI (albumin-bilirubin) score −1.80 (modified ALBI grade 2b), and the patient’s performance status was zero (Table 1). He had been prescribed medications for diabetes mellitus and hypertension, but had never received anticoagulants. We offered the patient transcatheter arterial chemoembolization (TACE) and systemic drug therapy; the patient preferred drug therapy. He experienced epigastric discomfort 4 days after the initiation of atezo-bev, but did not visit the hospital. The patient visited our hospital on the day of the second atezo-bev cycle. The epigastric discomfort had improved, but the serum C-reactive protein level was elevated (4.4 mg/dL). Abdominal ultrasound sonography indicated an echo-free space in the left upper abdomen. A contrast-enhanced CT scan showed a ruptured tumor at the edge of the left lateral lobe without extravasation, and the vascularity of all tumors was markedly suppressed (Fig. 3). A nonenhanced CT demonstrated high-attenuation areas around the subcapsule of the tumor in the left lateral lobe; moreover, the attenuation value was high in the pelvic fluid collection, indicating intra-abdominal bleeding as a result of the HCC rupture. Since the patient’s vital signs and general condition were stable and there was no anemia (Table 1), elective TAE was performed 3 days after the visit. The primary purpose of TAE was to prevent tumor rebleeding after the resumption of atezo-bev. There was no evidence of overt tumor staining on angiography, indicating a significant decrease in tumor vascularity. The feeder of the ruptured tumor was assumed to be the A2 vessel; therefore, we embolized the A2 vessel using gelatin sponge particles (Fig. 4). Following treatment, there were no adverse events and no change in hepatic reserve (Table 1), and the patient was discharged 6 days after TAE. We determined that atezo-bev was highly effective and decided to continue it. After TAE, atezo-bev was resumed, and no tumor bleeding has been noted since then.
Abdominal contrast-enhanced CT (A) and MRI (B) findings before operation. (A) An enhanced mass measuring 97 × 78 mm in diameter is identified in the right lobe of the liver on arterial-phase imaging. (B) A large mass measuring 100 × 80 mm in diameter is observed in the right lobe of the liver, and the tumor boundary appears clear on the hepatobiliary phase image.
Abdominal contrast-enhanced CT images taken before atezolizumab plus bevacizumab therapy (above: arterial phase images; below: equilibrium phase images). (A) A 14-mm HCC in S3 and a 35-mm HCC lateral to S2 are detected. (B) A 10-mm HCC in the middle part of S2 is detected. (C) A 13-mm HCC in the caudal part of S2 is detected. Four masses are identified in the lateral segment of the liver, showing hyperenhancement in the arterial phase (above images in A–C) and washout in the equilibrium phase (below images in A–C), and are diagnosed as HCCs.HCC, hepatocellular carcinoma
Abdominal contrast-enhanced CT images taken after the first cycle of atezolizumab plus bevacizumab therapy (above: arterial phase images; below: equilibrium phase images). No changes are observed in tumor size (arrowheads); however, the vascularity of all tumors is markedly suppressed (A–C). Ruptured HCC is identified in the lateral portion of S2 (arrows); however, the hematoma is localized in the subcapsular region, and no extravasation or pseudoaneurysm is observed (A, B).HCC, hepatocellular carcinoma
Transcatheter arterial embolization. (A) Angiography of the A2–A3 common vessel reveals no tumor staining. The A2 vessel is indicated by arrowheads. (B) After arterial embolization of A2, the A2 vessel is no longer visible, and the patency of the A3 vessel is preserved. The A3 vessel is indicated by the arrows.
DISCUSSION
To our knowledge, this is the first report of tumor rupture in a patient with unresectable HCC following atezo-bev treatment that was successfully managed with TAE therapy using gelatin sponge particles. Previous reports have described intratumoral hemorrhage in HCC during atezo-bev (Table 2).^4,5)^ Bevacizumab is a humanized monoclonal antibody against vascular endothelial growth factor (VEGF), and its anti-VEGF effect is related to hemorrhagic risk.^6)^ Ramucirumab, a VEGF receptor-2-targeting human immunoglobulin G monoclonal antibody, is also a therapeutic option for HCC. In the REACH-2 trial, the incidences of grade 3 or higher bleeding events were 5.1% and 3.2% in the ramucirumab and placebo groups, respectively.^7)^ So far, only one case of ramucirumab-induced HCC rupture has been reported, but there is concern regarding serious antiangiogenic adverse events during anti-VEGF drug treatment.^8)^ Lenvatinib, an inhibitor of multiple receptor tyrosine kinases, including VEGF receptors, has a pharmaceutical effect similar to that of bevacizumab, and intratumoral hemorrhage and rupture of HCC due to lenvatinib have been reported.^9–11)^ Uchida-Kobayashi et al. reported that 5 (7.4%) of the 68 consecutive patients who received lenvatinib treatment in their retrospective single-center study developed tumor hemorrhage (including 2 cases of rupture). Interestingly, hemorrhage occurred immediately after initiating lenvatinib treatment, with an average dosing period of 4.4 days.^9)^ The mechanism underlying HCC rupture is considered to be the antitumoral effect of lenvatinib, which inhibits tumor angiogenesis and causes the remaining poorly developed tumor microvasculature to collapse.^12)^
Spontaneous HCC rupture occasionally occurs, with an incidence of 2.3%–26%.^13)^ Although the mechanism underlying HCC rupture has not been fully elucidated, several hypotheses have been proposed. According to the intratumoral pressure hypothesis, rapid tumor growth, tumor necrosis, and occlusion of the hepatic vein caused by tumor invasion are related to an increase in the internal pressure of the tumor.^12–14)^ Several studies have reported that tumor size is greater in ruptured HCC than in nonruptured HCC.^9,15,16)^ Previous research has reported that HCCs >5 cm are at high risk of tumor rupture.^16,17)^ Tumor protrusion from the original liver parenchyma may also be related to tumor rupture.^16)^ Li et al. reported that tumor location is related to rupture, and that the majority of ruptured HCCs are located in the left lateral segments (S2 and S3) and the right posterior-inferior segment (S6).^18)^ Sorafenib and lenvatinib, which are multikinase inhibitors of the VEGF pathway, may increase the risk of bleeding and HCC rupture in susceptible individuals.^9,12,13)^ Anti-VEGF drugs, including bevacizumab, can cause the small arteries supplying the tumor to become fragile. Atezolizumab, an immune checkpoint inhibitor (ICI) that exerts antitumor effects by modulating the immune function, may also contribute to HCC rupture. ICIs may trigger “pseudoprogression,” in which a tumor grows before it shrinks.^19)^ Pseudoprogression is thought to be caused by the infiltration of immune cells, followed by tumor necrosis, hemorrhage, and edema in lesions. To date, only a few cases of pseudoprogression in HCC have been reported^20,21)^; however, there is concern regarding pseudoprogression-induced HCC rupture. In our case, the risk of HCC rupture may have been relatively high because of tumor protrusion from the liver surface in segment 2. However, tumor rupture occurred 4 days after atezo-bev administration, and CT findings revealed remarkable suppression of vascularity with a dramatic decline in tumor markers (Table 3); therefore, we speculated that atezo-bev triggered the HCC rupture. In cases of HCC rupture, TAE plays a crucial role in achieving hemostasis and stabilizing the patient's condition. Emergency hepatectomy can be performed in some cases; however, in many cases, patients with ruptured HCC do not tolerate laparotomy well.^14)^
Recently, atezo-bev therapy followed by curative conversion has been demonstrated for the treatment of unresectable, intermediate-stage HCC. Atezo-bev followed by TACE achieved a higher complete response rate than atezo-bev therapy alone.^22)^ Atezo-bev exerts anti-VEGF effects before TACE, thereby enhancing the effects of TACE.^22)^ There are various situations among intermediate-stage HCC, and the indications and timing for attempting conversion to curative therapy should be carefully considered. According to previous reports, HCC rupture often occurs soon after the administration of anti-VEGF agents.^9–11)^ When planning to administer atezo-bev to patients with HCC located on the liver surface, as in our case, TAE or TACE before the initiation of atezo-bev might be effective in preventing HCC rupture. Furthermore, removing only the HCC with a risk of rupture in advance using laparoscopic partial hepatectomy may safely allow systemic chemotherapy for the remaining HCCs.
CONCLUSIONS
The findings of this case suggest that clinicians should consider tumor rupture and check the tumor blood flow when abdominal pain appears after the initiation of atezo-bev for HCC in patients with risk factors for rupture.
ACKNOWLEDGMENTS
We would like to thank Editage (www.editage.jp) for English language editing.
DECLARATIONS
Funding
No financial support was provided.
Authors’ contributions
KT drafted the manuscript.
KT, SY, KI, and SN were involved in patient care.
TM, YYamada, and HT performed the interventional radiology procedures.
SY, RN, YYamada, and YYamashita contributed to manuscript review and editing.
KF gave final approval for the publication version.
All authors read and approved the final manuscript.
Availability of data and materials
All data generated during this study are included in this article.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Competing interests
The authors declare that they have no competing interests.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Finn RS Qin S Ikeda M Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med 2020; 382: 1894–905.32402160 10.1056/NEJ Moa 1915745 · doi ↗ · pubmed ↗
- 2Kudo M. A New Era in systemic therapy for hepatocellular carcinoma: Atezolizumab plus bevacizumab combination therapy. Liver Cancer 2020; 9: 119–37.32399427 10.1159/000505189 PMC 7206602 · doi ↗ · pubmed ↗
- 3Boige V Malka D Bourredjem A Efficacy, safety, and biomarkers of single-agent bevacizumab therapy in patients with advanced hepatocellular carcinoma. Oncologist 2012; 17: 1063–72.22707516 10.1634/theoncologist.2011-0465 PMC 3425524 · doi ↗ · pubmed ↗
- 4Mitsuyama Y Kageyama K Shinkawa H Atezolizumab plus bevacizumab-induced intratumoral hemorrhage in a patient with rib metastasis from unresectable hepatocellular carcinoma. Radiol Case Rep 2023; 18: 3037–40.37434611 10.1016/j.radcr.2023.06.012PMC 10331133 · doi ↗ · pubmed ↗
- 5Park KH Yoo JJ Kim SG Fatal intratumoral hemorrhage in a patient with hepatocellular carcinoma following successful treatment with atezolizumab/bevacizumab:a case report. World J Clin Cases 2024; 12: 5177–83.39109046 10.12998/wjcc.v 12.i 22.5177 PMC 11238802 · doi ↗ · pubmed ↗
- 6Duffy A Wilkerson J Greten TF. Hemorrhagic events in hepatocellular carcinoma patients treated with antiangiogenic therapies. Hepatology 2013; 57: 1068–77.23112096 10.1002/hep.26120 PMC 3584189 · doi ↗ · pubmed ↗
- 7Zhu AX Kang YK Yen CJ Ramucirumab after sorafenib in patients with advanced hepatocellular carcinoma and increased α-fetoprotein concentrations (REACH-2): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol 2019; 20: 282–96.30665869 10.1016/S 1470-2045(18)30937-9 · doi ↗ · pubmed ↗
- 8Haider A Siddiqa A Mehmood M Ramucirumab-induced hepatocellular carcinoma rupture and gastrointestinal perforation. Am J Case Rep 2021; 22: e 929493.33597391 10.12659/AJCR.929493 PMC 7901501 · doi ↗ · pubmed ↗