Statin treatment for cerebral small vessel disease: A systematic review and meta-analysis of randomized controlled trials
David Fresnais, Brynjar Fure

TL;DR
Statin treatment may reduce brain white matter damage, but evidence is limited and more research is needed to understand its effects on cognitive and functional outcomes.
Contribution
A systematic review and meta-analysis of randomized trials on statin use for cerebral small vessel disease.
Findings
A non-significant trend toward reduced white matter hyperintensity volume in the statin group.
Current evidence for statin treatment in cerebral small vessel disease is limited.
Future studies should focus on clinical and patient-centered outcomes, not just imaging results.
Abstract
•Statins may reduce white matter hyperintensities on brain imaging although current evidence is limited.•The mechanisms behind the possible effect of statins for cerebral small vessel disease are not yet known.•Future studies are needed and should focus on patient-centered and clinical outcomes and not exclusively on radiological outcomes. Statins may reduce white matter hyperintensities on brain imaging although current evidence is limited. The mechanisms behind the possible effect of statins for cerebral small vessel disease are not yet known. Future studies are needed and should focus on patient-centered and clinical outcomes and not exclusively on radiological outcomes. Cerebral small vessel disease (CSVD) is a chronic, progressive disorder that affects small blood vessels in the brain's white matter. This white matter damage appears on brain imaging as white matter…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
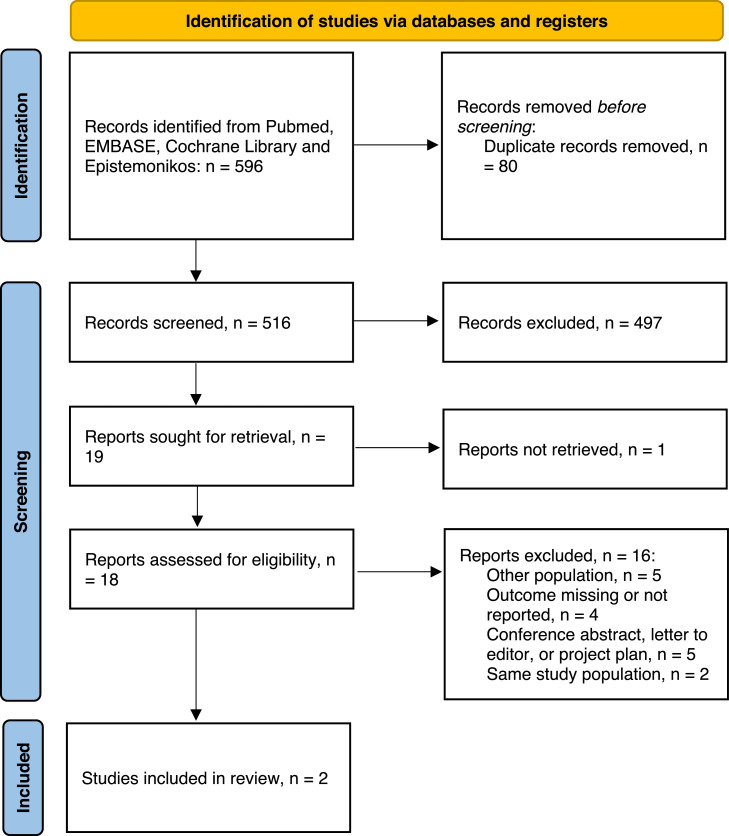 Figure 1
Figure 1 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCerebrovascular and genetic disorders · Neurological Disease Mechanisms and Treatments · Neurological Disorders and Treatments
Introduction
1
Cerebral small vessel disease (CSVD) is a chronic and progressive condition affecting the small vessels and capillaries supplying the brain’s white matter and subcortical structures, where the damage can be visualized as white matter hyperintensities (WMH), lacunes, enlarged perivascular spaces and microbleeds on brain magnetic resonance imaging (MRI) or computed tomography [1].
The prevalence of CSVD increases with age, affecting approximately 5 % of individuals in their 50 s and nearly 100 % of individuals in their 90 s [2]. The most common cause of CSVD is sporadic and associated with age and cardiovascular risk factors, especially hypertension [3]. In the 1960s, Fisher performed autopsies on patients with lacunar stroke and described pathological changes affecting small vessels less than 1 mm in diameter; lipohyalinosis, in which the accumulation of lipids leads to vessel wall-thickening and narrowing of lumen, and microatheroma [4]. These processes, along with arteriolosclerosis, are considered the most important pathophysiological mechanisms in hypertension-related CSVD. Other causes of CSVD include cerebral amyloid angiopathy, inflammatory and immune-mediated vascular diseases, and cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) [3].
CSVD is often asymptomatic, yet it accounts for 20 % of strokes and nearly half of vascular dementia cases, making it a clinically significant problem. Currently, no targeted treatments for CSVD exist beyond the modification of cardiovascular risk factors such as hypertension, hyperlipidemia, and diabetes mellitus [1]. Statins, which are the most commonly used drugs for treating hyperlipidemia, have been shown to reduce cardiovascular mortality in at-risk populations and are recommended by current guidelines for patients with both myocardial infarction and ischemic stroke [5,6]. Some studies have suggested that statins may reduce WMH burden in CSVD [7,8], while others have not demonstrated a clear effect [9].
Our understanding of the pathophysiological processes underlying CSVD remains limited, and although the pathophysiological processes involve deposition of lipids in intracerebral small vessels, the benefit of lipid-lowering treatments in CSVD is debated [10]. Therefore, the present meta-analysis was performed to investigate whether statins can affect the progression of CSVD.
Methods
2
Search strategy
2.1
A systematic search was conducted across Medline, EMBASE, Cochrane Library, and Epistemonikos to identify clinical trials on statin-treatment for CSVD. The search was performed by a trained information specialist in February 2024, using search terms such as “cerebral small vessel diseases,” “leukoaraiosis,” “subcortical infarct,” “lacunar infarct,” “white matter change,” “lipid regulating agent,” “statin,” and “HMG-CoA reductase inhibitor.” The literature search was restricted to studies published in English, Swedish, Norwegian, and Danish. A detailed description of the full search strategy is provided in Supplementary Material 1.
Selection criteria
2.2
This systematic review and meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [11]. Two investigators (D.F. and B.F.) independently screened the titles and abstracts of retrieved studies for inclusion, based on the following pre-specified selection criteria (PICOS): (1) population: older persons examined with brain MRI/CT for evaluation of WMH; (2) intervention: treatment with statins; (3) comparison: age-matched controls receiving placebo; (4) outcome: WMH volume, changes in WMH volume, HR/OR for progression of WMH and (5) study design: RCT, cohort studies with a control group. Articles in full-text were assessed by the same two investigators.
Data extraction and analysis
2.3
Two investigators (D.F. and B.F.) independently extracted data and recorded it in a table that included the following study characteristics: first author, year of publication, country, research setting, study design, sample size, patient demographics, randomization, statin treatment and dosage, and WMH volume and progression.
Statistical analysis
2.4
The differences in WMH volume and progression between the treatment and placebo groups were analyzed. Meta-analysis was conducted using inverse variance with RevMan version 5.4.1.22 [12], which automatically assigned weights according to the program’s algorithm. Two-sided p-values were reported, and effect estimates were presented as mean difference (MD).
Quality assessment and risk of bias
2.5
The quality of the included studies and their risk of bias were independently assessed by two investigators (D.F. and B.F.) using the Center for Evidence-Based Management (CEBM) critical appraisal worksheet tailored for randomized controlled trials [13]. The overall confidence in the effect estimates across studies for each pooled outcome was independently evaluated by the same two reviewers using the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) tool [14].
Resolution of discrepancies
2.6
Any disagreements arising during the study selection process, data extraction, or quality assessment were resolved through consensus between the investigators.
Results
3
Literature search
3.1
A total of 2 studies [7,15] were included in this review and meta-analysis following a full-text assessment of 18 articles, see Fig. 1. Studies that did not meet the eligibility criteria and were excluded are detailed in Supplementary Material 2.Fig. 1PRISMA flow chart of the inclusion process.Fig 1
Study characteristics
3.2
The general characteristics of the studies included in this meta-analysis are summarized in Table 1. Included studies were randomized controlled trials published in 2011 and 2020. Criteria used for diagnosis of CSVD were the Fazekas scale, number of lacunes and computer estimated volume of WMH. The types of statins used were rosuvastatin and atorvastatin. Mean age of the research persons across the included studies ranged from 73 to 78 years. WMH burden and Fazekas score are reported in Table 1.Table 1. General study characteristics**.**Table 1. Author and year of publicationGuo 2020Tendolkar 2011CountryChinaNetherlandsSettingUniversity hospital, community-based sampleOutpatient clinic of university hospitalSamplePersons with hypertension, ≥75 yearOlder-, stroke-free persons with atrial fibrillationSubjects (n; controls, intervention)109, 11817, 17Criteria for CSVDSTRIVE, Fazekas scale, Lacunes – cavities 3–15 mm with cerebrospinal-like signalingManual and computed estimationAge, mean (SD); controls, intervention78.48 (2.58), 78.24 (2.35)73.5 (4.0); 74.5 (4.2)Sex (male; n (%)109 (0.48)17 (50)Years of education, meanNRNRStatin treatment (substance, dose in mg)Rosuvastatin, 10 mg/dayAtorvastatin, 20 – 40 mgTreatment duration in months61.812Baseline Fazekas scorePrevalence of score of 2 or 3: n, 48; 21.1 %NRWMH volume in ml in intervention group at follow-upMean 4.29, SD 1.92Mean 4.19, SD 0.4WMH volume in ml in controls at follow-upMean 5.05, SD 1.91Mean 11.56, SD 0.01WMH progression (OR; HR)0.19, 0.07 – 0.53; 0.408, 0.233 – 0.716)NRProgression of lacunar infarcts (OR; HR)0.34, 0.15 – 0.75; 0.417, 0.257 – 0.676NRCSVD, cerebral small vessel disease; HR, Hazard ratio; NR, not reported; OR, odds ratio; SD, standard deviation; STRIVE, Standards for Reporting Vascular Changes on Neuroimaging; WMH, white matter hyperintensities.
Meta-analysis
3.3
Data from the included studies with a total of 112 persons treated with statins for CSVD and 463 controls were used for meta-analysis. Sample sizes ranged from 34 [15] to 227 [7]. The total WMH volume was 4.44 ml lower (CI -10.19 – 1.31, p = 0.13) in the statin group compared to controls, although not statistically significant, see Fig. 2.Fig. 2. White matter hyperintensities in persons with statins versus no statins.Fig 2
Quality assessment of the included studies
3.4
The quality of the included studies was evaluated using the CEBM checklist designed for randomized controlled trials [13], with results presented in Table 2.Table 2. Assessment of overall risk of bias of included studies.Table 2. Author and year of publicationOverall appraisalGuo 2020+Tendolkar 2012++, low risk.
Certainty of evidence
3.5
The certainty of the pooled estimates was assessed using the GRADE approach, with results presented in Table 3. Our confidence in the pooled estimates was low and it is therefore very likely that future studies will have an impact on the results.Table 3. Confidence in the pooled estimate of progression of white matter hyperintensities according to GRADE.Table 3. Certainty assessment№ of patientsEffectCertaintyImportance№ of studiesStudy designRisk of biasInconsistencyIndirectnessImprecisionOther considerationsStatinplaceboRelative(95 % CI)Absolute(95 % CI)White matter hyperintensity volume in statin vs placebo2randomised trialsnot seriousnot seriousnot seriousvery seriousanone112463-MD 4.44****ml lower(10.19 lower to 1.31 higher)⨁⨁◯◯LowIMPORTANTCI, confidence interval; MD, mean difference.a. Small number of studies.
Discussion
4
The results from this systematic review and meta-analysis of randomized controlled trials indicate that there is currently insufficient evidence to conclude that statins are effective for treatment of CSVD. Meta-analysis of WMH volume in the two included studies showed a non-significant trend towards a protective effect, although the confidence in the pooled estimate was low according to GRADE. A factor that could attenuate the result is the fact that WMH-burden was markedly higher in the treatment group at baseline in one of the included studies. Only one of the included studies has specifically evaluated the impact of statin therapy on lacunar infarcts, reporting a protective effect [7]. Although the protective effect of statins on cardiovascular events has been demonstrated earlier, this study has examined the current evidence for their effect on cerebrovascular disease in a stroke-free population. One previous meta-analysis from 2020 looked at the effects of statins on WHM-burden in addition to silent brain infarcts, although meta-analysis of the former outcome was not possible due to the limited number of studies available at that time [16].
Rosuvastatin was used in one of the studies and atorvastatin was used in the other. While study results were consistent, it is important to consider that the first mentioned is a water-soluble substance and the latter is lipid-soluble, affecting permeability and accumulation in the central nervous system. If the main effect of statins for the prevention of CSVD is dependent on substance-concentration in the brain, this would therefore be important to consider.
The dose of statins used was low-moderate – 10 mg for rosuvastatin and 20 – 40 mg for atorvastatin; highest recommended dosage is 40 mg and 80 mg, respectively. In this patient group, we have not identified any randomized controlled trials of full-dose statin treatment for comparison.
The exact mechanisms by which statin treatment could reduce CSVD-progression are not yet known. In CSVD related to cardiovascular risk factors, such as hypertension, statins may have a protective effect through several interrelated mechanisms: 1) interfere with the build-up of lipids in blood vessel walls preventing the main pathophysiological contributors – arteriolosclerosis, lipohyalinosis and microatheroma [4]; 2) anti-inflammatory effects through reduction of inflammatory mediators including C-reactive protein [17,18] and interleukin-6 [18]; 3) reduced oxidative stress [19]; 4) protection from microvascular thrombosis by counteracting platelet aggregation and promoting fibrinolysis [20].
Slowing down the CSVD-process may not only reduce the risk of vascular dementia but could also affect the risk of developing Alzheimer’s disease. At present, there is evidence that CSVD may be linked to a higher conversion rate from mild cognitive impairment to Alzheimer’s dementia [21] and a higher risk of developing Alzheimer’s disease in people who are free from cognitive impairment [22]. The mechanisms explaining this association between CSVD and Alzheimer’s disease are not clear, but could be associated to changes in brain fluid drainage, disturbance of the blood-brain barrier or even inflammation processes [23].
Limitations of this systematic review and meta-analysis include: 1) it is based on a small number of studies; 2) even though the literature search was conducted by an experienced information specialist, it is still possible that some articles were missed; 3) due to the risk of imprecision, our confidence in the pooled estimate was rated as low according to GRADE; 4) due to the limited number of studies, no meaningful subgroup analysis of statin-type or dosage was possible; 5) in cases of missing information, authors were contacted although not all of them answered or were able to provide the data necessary. The transparent methodology according to the PRISMA protocol is a strength in this study, as well as the thorough review of available evidence from randomized controlled trials of statin-treatment for prevention of CSVD.
In conclusion, the few studies that have examined the effect of statins on CSVD show a possible protective effect on the brain’s microvasculature. The current evidence is limited and largely based on non-clinical outcomes. The clinical impact of reducing the burden of WMH remains difficult to quantify, particularly given that CSVD progression often coincides with normal physiological aging. For patients and clinicians, it is frustrating that CSVD-related cognitive impairment can continue to progress despite comprehensive treatment with antihypertensive, cholesterol-lowering, antidiabetic, and antiplatelet therapies. Taking this current knowledge gap into consideration, more research is strongly warranted, and future research should focus on clinical and patient-centered outcomes, including global cognitive measures and activities of daily living, alongside surrogate radiological outcomes. Additionally, further randomized controlled trials are needed to investigate the effects of different types and doses of statins on both clinical and radiological manifestations of CSVD.
Ethical considerations
The data used for this systematic review and meta-analysis has been gathered from previously published literature only. Therefore, application for ethical consent is not necessary as stated in the Swedish law and guidelines of the Ethical Committee of Uppsala University, Sweden.
Funding
This study was funded by both Örebro University School of Medical Sciences, Örebro, Sweden, and Central Hospital Karlstad, Karlstad, Sweden.
Generative AI statement
No generative AI tools were used in the conception, writing, or analysis of this scientific paper.
CRediT authorship contribution statement
David Fresnais: Writing – original draft, Validation, Methodology, Formal analysis, Conceptualization, Writing – review & editing, Visualization, Project administration, Investigation, Data curation. Brynjar Fure: Writing – review & editing, Validation, Project administration, Investigation, Conceptualization, Visualization, Supervision, Methodology, Data curation.
Declaration of competing interest
There are no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chojdak-Łukasiewicz J.Dziadkowiak E.Zimny A.Paradowski B.Cerebral small vessel disease: a review Adv. Clin. Exp. Med.30320213493563376873910.17219/acem/131216 · doi ↗ · pubmed ↗
- 2de Leeuw F.E.de Groot J.C.Achten E.Oudkerk M.Ramos L.M.Heijboer R.Prevalence of cerebral white matter lesions in elderly people: a population based magnetic resonance imaging study. The Rotterdam Scan Study J. Neurol. Neurosurg. Psychiatry 70120019141111824010.1136/jnnp.70.1.9PMC 1763449 · doi ↗ · pubmed ↗
- 3Cerebral Small Vessel Disease, Hypertension, and vascular contributions to cognitive impairment and dementia | Hypertension [Internet]. [cited 2024 Aug 16]. Available from: https://www.ahajournals.org/doi/10.1161/HYPERTENSIONAHA.123.19943.10.1161/HYPERTENSIONAHA.123.19943 PMC 1073478938044814 · doi ↗ · pubmed ↗
- 4Fisher CM.Lacunes: Small, deep cerebral infarcts Neurology 1519657747841431530210.1212/wnl.15.8.774 · doi ↗ · pubmed ↗
- 52021 Guideline for the prevention of Stroke in patients with Stroke and transient ischemic attack: A Guideline from the American Heart Association/American Stroke Association | Stroke [Internet]. [cited 2024 Aug 16]. Available from: https://www.ahajournals.org/doi/10.1161/STR.0000000000000375.
- 62023 AHA/ACC/ACCP/ASPC/NLA/PCNA Guideline for the management of patients with chronic coronary disease: A report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines | circulation [Internet]. [cited 2024 Aug 16]. Available from: https://www.ahajournals.org/doi/10.1161/CIR.0000000000001168.
- 7Guo Y.Li Y.Liu X.Cui Y.Zhao Y.Sun S.Assessing the effectiveness of statin therapy for alleviating cerebral small vessel disease progression in people ≥75 years of age BMC Geriatr 2020202923280708610.1186/s 12877-020-01682-w PMC 7430010 · doi ↗ · pubmed ↗
- 8Ji T.Zhao Y.Wang J.Cui Y.Duan D.Chai Q.Effect of low-dose statins and apolipoprotein E genotype on cerebral small vessel disease in older hypertensive patients: A subgroup analysis of a randomized clinical trial J. Am. Med. Dir. Assoc.19112018995-1002.e 410.1016/j.jamda.2018.05.02530006015 · doi ↗ · pubmed ↗