Impact of diabetes on three-year outcome after coronary stenting in patients with polyvascular atherosclerotic disease – a secondary analysis of the randomized TWENTE trials
Daphne van Vliet, Tineke H. Pinxterhuis, Eline H. Ploumen, Marlies M. Kok, Rosaly A. Buiten, Paolo Zocca, Ariel Roguin, Carl E. Schotborgh, Rutger L. Anthonio, Peter W. Danse, Edouard Benit, Adel Aminian, Carine J.M. Doggen, Clemens von Birgelen

TL;DR
Diabetes significantly increases the risk of adverse outcomes after heart stenting in patients with widespread artery disease, mainly due to higher death rates.
Contribution
This study quantifies the additional risk diabetes poses in polyvascular disease patients undergoing coronary stenting, showing a more than 50% increase in event risk.
Findings
Diabetes increases the risk of major adverse cardiac events by 49% in polyvascular disease patients after stenting.
All-cause mortality is more than twice as high in diabetic patients compared to non-diabetic ones.
Insulin-treated diabetic patients show the highest risk of adverse outcomes.
Abstract
•Diabetes rises event risk after coronary stenting in polyvascular disease patients.•We examine to which extent diabetes increases the already elevated event risk.•Diabetes rises the event risk in polyvascular disease patients by > 50 %.•This is mainly attributable to more deaths from any cause.•These data suggest that strong preventive measures are warranted in these patients. Diabetes rises event risk after coronary stenting in polyvascular disease patients. We examine to which extent diabetes increases the already elevated event risk. Diabetes rises the event risk in polyvascular disease patients by > 50 %. This is mainly attributable to more deaths from any cause. These data suggest that strong preventive measures are warranted in these patients. The presence of polyvascular atherosclerotic disease is associated with a high-risk of adverse events following percutaneous…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
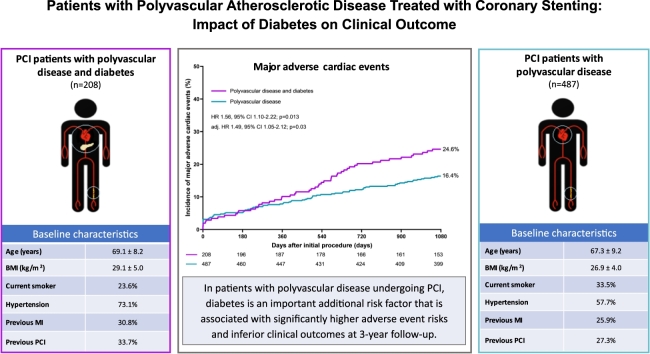 Figure 1
Figure 1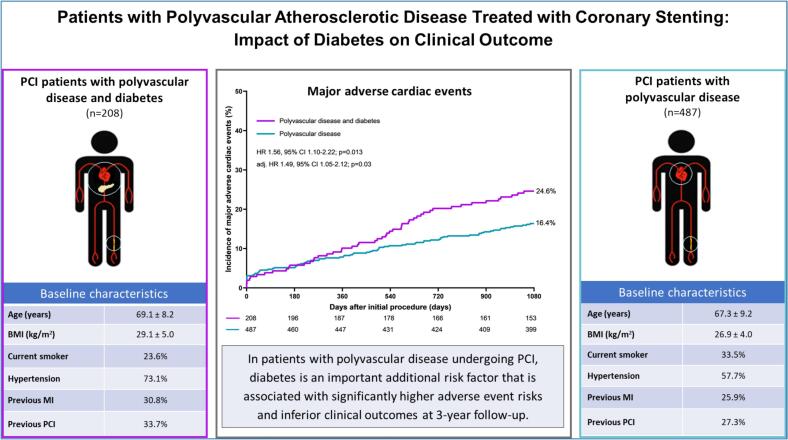 Figure 2
Figure 2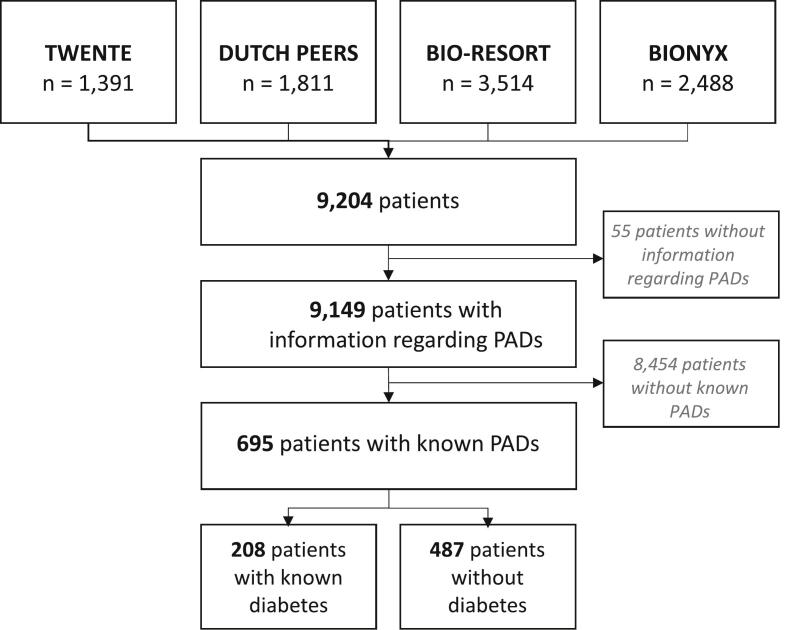 Figure 3
Figure 3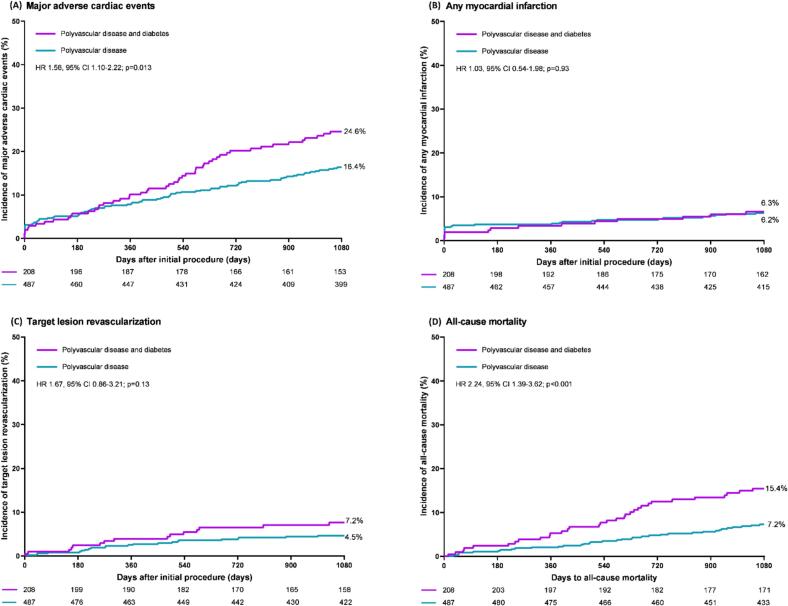 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCoronary Interventions and Diagnostics · Antiplatelet Therapy and Cardiovascular Diseases · Acute Myocardial Infarction Research
Introduction
1
Atherosclerosis is a systemic disease, and the presence of clinically apparent atherosclerosis in one vascular bed is associated with an increased likelihood of symptomatic arterial changes in other vascular beds.[1] Consequently, patients with obstructive coronary artery disease (CAD) are more likely to have concomitant peripheral artery disease, cerebrovascular disease, and aortic disease.[2] These patients with polyvascular disease are at an elevated risk for various adverse events.[3,4] In all-comer patients with obstructive CAD who undergo percutaneous coronary intervention (PCI), the presence of polyvascular disease has been observed in at least 5 % of the cases.[[5], [6], [7]] As previously demonstrated, patients with polyvascular disease are at a markedly elevated risk of adverse clinical events following PCI with contemporary drug-eluting stents (DES), including an almost twice as high mortality as compared to patients without polyvascular disease at long-term follow-up.[5,8,9].
Diabetes mellitus affects both the function and structure of blood vessels throughout the entire human body. It is a well-established risk factor for atherosclerosis and associated with an increased risk of adverse clinical events following PCI.[[10], [11], [12]] The prevalence of diabetes is increased in the presence of polyvascular disease [5], and in all-diabetic populations (not specifically PCI patients) MACE occurred more frequently in the presence of polyvascular disease.[6,7] In a selected population of ACS patients with polyvascular disease, a higher rate of MACE was observed in the presence of diabetes.[8] Yet, the present study is the first to assess in an all-comer PCI population with polyvascular disease the impact of diabetes on post-PCI clinical outcome.
As the precise extent to which diabetes contributes to the elevated risk of adverse clinical events following PCI in patients with polyvascular disease has yet to be determined, this analysis sought to evaluate the impact of diabetes on long-term clinical outcomes following PCI in these patients, which may affect prognosis and secondary prevention. In other words, the present study addresses the question whether diabetes is still a significant additional risk factor in PCI patients who already have a very high adverse event risk due to the presence of polyvascular disease. Data were used from a pooled patient-level database comprising four randomized PCI trials that assessed new-generation DES in all-comers. In particular, we compared the baseline characteristics and 3-year clinical outcomes after PCI in polyvascular disease patients with and without medically treated diabetes.
Methods
2
Study design
2.1
In order to conduct this analysis, patient-level data from 4 randomized controlled trials consisting of 9,204 all-comer patients, were pooled: TWENTE (TWENTE I, NCT01066650), DUTCH PEERS (TWENTE II, NCT01331707), BIO-RESORT (TWENTE III, NCT01674803), and BIONYX (TWENTE IV, NCT02508714)). The details of the original trials have been previously reported.[[16], [17], [18], [19]] Briefly, the trials were investigator-initiated, assessor- and patient-blinded randomized studies. Patients were eligible for enrolment if they were at least 18 years of age, were able to provide informed consent, and required PCI with the implantation of new-generation DES for the treatment of obstructive CAD. Further study details regarding the 4 original trials can be found in Supplementary Table 1. The TWENTE II-IV trials included patients who presented with any type of coronary syndrome, while the TWENTE I trial enrolled all patients except for those presenting with an acute ST-segment elevation myocardial infarction (STEMI). Overall, patients were enrolled at 9 study sites: 6 Dutch centers, 2 Belgian centers, and 1 Israeli center. In the 3-arm BIO-RESORT trial, randomization between stent types was performed in a 1:1:1 fashion, while in the TWENTE, DUTCH PEERS, and BIONYX trials the randomization was performed in a 1:1 fashion. A custom-designed computer program with random block sizes of 4 and 8 was used for web-based randomizations. Stratification was performed for diabetes in the BIO-RESORT and BIONYX trials, and for sex in the TWENTE and BIONYX trials. The trials complied with the Declaration of Helsinki and the Medical Ethics Committee Twente, and the Institutional Review Boards of all participating centers provided approval for all original trials. All trial participants provided written informed consent. Besides the exclusion criteria as described in the 4 randomized trials, no additional exclusion criteria were made for the current analysis.Table 1. Baseline characteristics of patients, target lesions, and PCI procedures.Diabetes****p-valueYes (n = 208)No (n = 487)General patient characteristicsAge (years)69.1 ± 8.267.3 ± 9.20.01Female sex64(30.8)129(26.5)0.25BMI (kg/m^2^)29.1 ± 5.026.9 ± 4.0*<0.001Current smoker48/208(23.6)162/485(33.5)0.01Medical historyRenal failurea31(14.9)50(10.3)0.08Hypertension152(73.1)281(57.7)<0.001*Hypercholesterolemia124/204(60.8)263/479(54.9)0.16Previous stroke33(15.9)57(11.7)0.14LVEF < 30 %10(4.9)22(4.6)0.87Previous myocardial infarction64(30.8)126(25.9)0.19Previous PCI70(33.7)133(27.3)0.09Previous coronary artery bypass grafting36(17.3)64(13.1)0.15Family history of coronary artery disease94/201(46.8)243/469(51.8)0.23Coronary syndrome at presentation0.14Stable angina pectoris92(44.2)202(41.5)STEMI16(7.7)66(13.6)Non-STEMI56(26.9)112(23.0)Unstable angina pectoris44(21.2)107(22.0)Target lesions and PCI proceduresTarget coronaryLeft main stem8(3.8)20(4.1)0.87Right coronary artery93(44.7)217(44.6)0.97Left anterior descending artery89(42.8)187(38.4)0.28Left circumflex artery59(28.4)162(33.3)0.20Bypass graft11(5.3)23(4.7)0.75Total stent length (mm)42.4 ± 29.743.1 ± 30.70.39At least 1 severely calcified lesion64(30.8)130(26.7)0.27At least 1 ostial lesion18(8.7)57(11.7)0.24At least 1 bifurcation lesion^b^65(31.3)145(29.8)0.70At least 1 chronic total occlusion6(2.9)24(4.9)0.23At least 1 complex lesion^c^169(81.3)367(75.4)0.09Small vessel treated (<2.75 mm)135(64.9)285(58.5)0.12Multivessel treatment46(29.1)112(23.0)0.80Values are mean ± SD, n (%) or n/N (%).aDefined as previous renal failure, creatinine ≥ 130 μmol/L, or need for dialysis; ^b^Target lesions were classified as bifurcated if a side branch ≥ 1.5 mm originated from them. ^c^Defined as a lesion complexity of B2 or C. Abbreviations: LVEF = Left ventricle ejection fraction; STEMI=ST-segment–elevation myocardial infarction; PCI = percutaneous coronary intervention; BMI = body–mass-index.
The PCI patients (who by definition all had obstructive CAD) were classified as having polyvascular disease in the presence of concomitant peripheral arterial disease (PADs). In accordance with the methodology employed in previous studies,[20,21] patients were classified as having PADs if they by anamnesis or medical record had a documented history of at least one of the following: (1) symptomatic atherosclerotic lesion in the lower or upper extremities; (2) atherosclerotic lesion in the aorta causing symptoms or requiring treatment; (3) atherosclerotic lesion in the carotid or vertebral arteries related to non-embolic ischemic cerebrovascular event; or (4) symptomatic atherosclerotic lesion in a mesenteric artery.
Procedures, follow-up, and monitoring
2.2
All interventional procedures were performed by experienced interventional cardiologists in consonance with current international guidelines. Generally, dual antiplatelet therapy was prescribed for 12 months in case of an acute coronary syndrome, while this was 6 to 12 months for patients with a chronic coronary syndrome. Data on cardiovascular risk factors and comorbidities were collected at the time of the index PCI from the medical record or via questionnaires. Clinical events were assessed annually after the first PCI at a visit to an outpatient clinic, or by questionnaires or telephone follow-up. Adverse clinical events were confirmed by collecting the source documents from hospitals or treating physicians. The original trials were independently monitored. Potential adverse clinical events were adjudicated by external clinical event committees.
Clinical endpoints
2.3
The main endpoint of the present analysis was major adverse clinical events (MACE), a composite of any myocardial infarction (MI), emergent coronary bypass surgery, clinically indicated target lesion revascularization, or all-cause mortality. Several other clinical endpoints were assessed, including the composite endpoints target vessel failure (TVF; cardiac mortality, target vessel MI, or clinically indicated target vessel revascularization), and the individual components of these composite clinical endpoints. All clinical endpoints were prespecified according to recommendations of the Academic Research Consortium.[22,23].
Supplementary analyses
2.4
We identified trial participants without polyvascular disease from the pooled database of the four randomized TWENTE trials and compared the clinical outcomes between those with and without diabetes. Adverse clinical events were assessed in analogy with the main analysis, applying the same endpoint definitions and statistical methods. The results of this analysis are presented in the Supplementary Material and allow contextualization of the findings of the main analysis in the study population with polyvascular disease. In addition, we performed another supplementary analysis, assessing the clinical outcomes in patients with polyvascular disease, classified by diabetes and insulin treatment.
Statistical analysis
2.5
Differences in categorical variables were assessed with the Chi-square test, and the Student t-test or Wilcoxon Rank Sum test were used to assess differences in continuous variables whichever was appropriate. Kaplan-Meier statistics were used to assess time to primary and secondary endpoints, and the log-rank test was applied for between-group comparisons. Cox proportional hazards analysis were used to compute Hazard ratios (HR) with two-sided confidence intervals (CIs). Potential confounders were identified if a p-value of < 0.15 was found in univariate analyses, both in the association of the potential confounder with diabetes and with MACE. In the first pass of a multivariate Cox regression model, all potential confounders were included. Stepwise backward selection was used to exclude variables with a non-significant association with the main endpoint; the final model consisted of only age and sex. Adding potential confounders hypertension, BMI and hypercholesterolemia or randomized stent arm to the final model did not have an impact on the adjusted hazard ratio of the primary endpoint MACE, and were therefore not included in the final model. Confidence intervals were two-sided and p-values < 0.05 were considered significant. SPSS version 24.00 (IBM, Armonk, NY) was used for the statistical analyses.
Results
3
Study population
3.1
The current study population is based on 695 patients with known polyvascular disease. As shown in Fig. 1, Fig. 2, a total of 208 (29.9 %) of the study patients had known, medically treated diabetes while 487 (70.1 %) had no diabetes.Fig. 1. Graphical abstract.Fig. 2. Study flowchart.
Baseline characteristics
3.2
Patients with diabetes were on average 1.8 years older than patients without diabetes, had a higher body-mass-index (BMI) and a higher prevalence of arterial hypertension, but were less likely to be active smokers at the time of the index procedure (Table 1). There was no statistically significant between-group difference in the characteristics of target lesions and PCI procedures. In both patients with and without diabetes, three out of four patients were treated for at least one complex coronary lesion. Further details on the patient, lesion, and procedural characteristics are presented in Table 1.
Clinical outcome
3.3
At 3-year follow-up, the study population of PCI patients with polyvascular disease showed a significantly higher incidence of the primary endpoint of MACE in the presence of diabetes (24.6 % vs. 16.4 %, HR: 1.56, 95 %CI: 1.10–2.22, p = 0.01). The difference in MACE was primarily attributable to a disparity in its component all-cause mortality (15.4 % vs. 7.2 %, HR: 2.24, 95 %CI: 1.39–3.62, p < 0.001), and it remained statistically significant following adjustment for confounders (adj. HR: 1.49, 95 %CI: 1.05–2.12, p = 0.03). The event rates of the two other individual components of MACE – target lesion revascularization and any MI – showed no statistically significant difference between patients with and without diabetes (7.2 % vs. 4.5 %, p = 0.13, and 6.3 % vs. 6.2 %, p = 0.93, respectively). The time-to-event curves of MACE and its three individual components are displayed in Fig. 3.Fig. 3. Kaplan-Meier time-to-event curves of the incidence of major adverse cardiac events and individual components: Major adverse cardiac events (A), any myocardial infarction (B), target lesion revascularization (C), and all-cause mortality (D). Abbreviations: PADs = peripheral arterial disease, HR = hazard ratio, CI = confidence interval.
The secondary composite endpoint of TVF also showed a higher event rate in patients with diabetes as compared to those without diabetes (20.7 % vs. 14.0 %, HR: 1.53, 95 %CI: 1.04–2.24, p = 0.03). Of the individual components of TVF, both target vessel revascularization and cardiac mortality showed higher rates in patients with diabetes (12.0 % vs. 7.0 %, p = 0.021, and 7.2 % vs. 3.5 %, p = 0.03, respectively), while the there was no difference in target vessel MI (4.8 % vs. 5.5, p = 0.72). The between-group difference in TVF remained statistically significant after adjustment for confounders (adj. HR: 1.48 95 %CI: 1.01–2.18, p = 0.04). Further details on these and other clinical outcomes are presented in Table 2.Table 2. Clinical outcomes at 3-year follow-up.DiabetesHR(95 %-CI)P_log-rank_Adjusted HR^c^****(95 %-CI)****P-valueYes (n = 208)No(n = 487)Major adverse cardiac events ^a^51(24.6)79(16.4)1.56 (1.10–2.22)0.011.49 (1.05–2.12)0.03All-cause mortality32(15.4)35(7.2)2.24 (1.39–3.62)<0.0012.07 (1.28–3.35)0.003Cardiac mortality15(7.2)17(3.5)2.15 (1.08–4.31)0.031.99 (1.00–3.99)0.05Any myocardial infarction13(6.3)30(6.2)1.03 (0.54–1.98)0.931.02 (0.53–1.95)0.96Target vessel related myocardial infarction10(4.8)27(5.5)0.88 (0.42–1.81)0.720.86 (0.42–1.79)0.69Any revascularization28(13.5)59(12.1)1.15 (0.73–1.80)0.551.16 (0.74–1.82)0.53Target vessel revascularization25(12.0)34(7.0)1.82 (1.09–3.05)0.021.88 (1.12–3.16)0.02Target lesion revascularization15(7.2)22(4.5)1.67 (0.86–3.21)0.131.72 (0.89–3.33)0.11Target vessel failure^b^43(20.7)68(14.0)1.53 (1.04–2.24)0.031.48 (1.01–2.18)0.04Definite-or-probable stent thrombosis3(1.4)5(1.0)1.44 (0.34–6.03)0.621.50 (0.36–6.35)0.58Data are n (%), unless otherwise indicated. ^a^Major adverse cardiac events is a composite of all-cause mortality, any myocardial infarction, emergent coronary artery bypass surgery, and clinically indicated target lesion revascularization. ^b^Target vessel failure is a composite of cardiac mortality, target vessel related myocardial infarction, and clinically indicated target vessel revascularization. ^c^Adjusted for sex and age.
Supplementary analysis
3.4
For the purpose of comparison with the clinical outcomes of the present study population, Supplementary Table 2 presents the clinical outcomes of 8,454 PCI trial participants patients without polyvascular disease. A total of 1,539 (18.2 %) of them had known diabetes and showed significantly worse 3-year outcomes for all clinical endpoints: the rate of MACE was 16.7 % in the presence of diabetes and 9.5 % in the absence of diabetes (HR: 1.83, 95 %CI 1.6–2.1, p < 0.001). After adjustment for confounders, the between-group differences with higher event rates in the presence of diabetes remained statistically significant for MACE (adj. HR: 1.70, 95 %CI: 1.47–1.96, p < 0.001) and all other clinical endpoints. Supplementary Table 3 reports the findings of a subanalysis to assess the clinical outcomes among polyvascular disease patients with insulin-treated diabetes versus no diabetes (Table S3a), and between those with non-insulin-treated diabetes versus no diabetes (Table S3b). In total, 83 (39.9 %) patients with diabetes were treated with insulin. The insulin-treated patients showed, also after adjustment for confounders, a statistically higher rate of MACE than patients without diabetes (31.3 % vs. 16.4 %, HR: 2.00 95 % CI: 1.29–3.12, p = 0.002). In contrast, there was no significant difference in MACE between non-insulin-treated patients and those without diabetes (20.0 % vs. 16.4 %, HR: 1.27 95 %CI: 0.81–1.99, p = 0.30). All-cause mortality showed significantly higher rates in both insulin-treated and non-insulin-treated diabetic patients as compared to patients without diabetes, but the target lesion revascularization rate showed a significant difference only between insulin-treated and non-diabetic patients (9.6 % vs. 4.5 %, p = 0.047).
Discussion
4
Study findings
4.1
The current analysis reports the additional impact of diabetes in PCI patients with polyvascular disease, which was primarily driven by patients who were insulin-treated. At long-term follow-up, patients with diabetes showed a 56 % higher incidence of the primary endpoint than patients without diabetes (MACE: 24.6 % versus 16.4 %), a difference that was primarily attributable to its individual component all-cause mortality. In addition, several secondary endpoints (TVF and repeat target vessel revascularization) were significantly increased in the presence of diabetes. The absolute increase in MACE rate associated with the presence of diabetes in the present study population was similar to that in patients without polyvascular disease (+8.2 % and + 7.2 %, respectively). The findings of this study indicate that in the high-risk population of PCI patients with polyvascular disease, the presence of diabetes represents a profoundly relevant additional cardiovascular risk factor that is associated with inferior clinical outcomes at long-term follow-up after coronary stenting.
Cardiovascular risk profile
4.2
Given that atherosclerosis is a systemic disease, patients with obstructive CAD frequently have atherosclerosis in other vascular beds. At least 5 % of all PCI patients have polyvascular disease, meaning they not only have CAD but also PADs.[[5], [6], [7]] Previous studies on clinical outcome after PCI have shown that polyvascular disease is an independent predictor of adverse clinical outcome.[5,6] An analysis of the e-Ultimaster study has shown higher event rates of the composite primary endpoint TLF after PCI in patients with multisite arterial disease than in those without.[5] Another clinical trial has shown that almost half of all patients hospitalized with acute myocardial infarction had known vascular disease.[24] As the number of affected vascular sites increased, the mean age of patients was higher, and patients more often had a history of dyslipidaemia, heart failure, and diabetes. In addition, the odds of major adverse cardiovascular and cerebrovascular events, mortality, and major bleeding incrementally increased and were highest in those with at least three affected vascular beds.[24] Furthermore, a post-hoc analysis of a pharmacological trial has examined the effect of an increasing number of affected vascular beds on the risks of MACE and all-cause mortality in patients with diabetes.[25] At baseline, patients with an increasing number of affected arterial beds were associated with a higher rate of hypertension, dyslipidemia and renal insufficiency. After 5 years of follow-up, each additional diseased bed was associated with higher risks of MACE and all-cause mortality.
In the present study, polyvascular disease patients with diabetes had a higher cardiovascular risk profile with significantly higher age and BMI, and a higher rate of hypertension than those without diabetes. In addition, the prevalence of other comorbidities such as renal insufficiency, dyslipidemia, previous stroke, heart failure, and previous revascularization was numerically higher, which is consistent with the findings of previous studies.[11,12,26].
Outcome of PCI patients with polyvascular disease and diabetes
4.3
Although several studies assessed the prevalence and impact of polyvascular disease in an all-diabetic patient population [13,14], very few studies have evaluated the impact of diabetes on clinical outcome in patients with polyvascular disease,[27] especially in patients undergoing PCI.[15] The IMPROVE-IT trial investigated the long-term cardiovascular risk associated with polyvascular disease (defined as peripheral artery disease or previous stroke or transient ischaemic attack) and diabetes in patients with an acute coronary syndrome.[15] After 7 years of follow-up, the presence of diabetes in addition to polyvascular disease was independently associated with an increased risk of reaching the primary composite endpoint of stroke, major coronary event, or cardiovascular death as compared to patients without diabetes (60.0 % vs. 39.8 %). Assessing a slightly different primary composite clinical endpoint at 3-year follow-up after PCI with new-generation DES, the present study reaches a similar conclusion. Nevertheless, in the IMPROVE-IT trial no more than 82 % of the patients with polyvascular disease underwent a PCI, and the study enrolled patients from 2005 to 2010, which implies that in IMPROVE-IT many PCI procedures have been performed with stents of an earlier generation than used in the present study. To our knowledge, this is the first study to assess in an all-comer PCI population with polyvascular disease the impact of diabetes on post-PCI clinical outcome.
Findings of the present study showed a significantly higher rate of MACE in PCI patients with both polyvascular disease and diabetes. Yet, this higher event rate is driven by all-cause mortality and not by differences in any MI or any revascularization. We can only hypothesize about causal mechanisms. At first, patients with diabetes are at higher risk of having autonomic neuropathy, possibly leading to silent myocardial ischemia and consequently, underdiagnosing of myocardial infarction.[28] In addition, it is possible that the incremental effect of diabetes is less noticeable, as both polyvascular disease and diabetes are independent risk factors of cardiac events post-PCI. Finally, we observed that patients with diabetes are at higher risk of all-cause mortality, making it possible that patients died of non-cardiac causes, before experiencing a cardiac event (competing risk phenomenon).
Clinical implications
4.4
As the presence of diabetes further complicates the prognosis after PCI in patients with polyvascular disease, secondary prevention of diabetes is of paramount importance. This is especially true for patients with diabetes treated with insulin, who show higher rates of MACE, all-cause mortality and target lesion revascularization. Given the increasing prevalence of diabetes and its strong association with PADs, the current ESC guidelines on the management of peripheral arterial and aortic diseases recommend screening for (pre)diabetes in patients with PADs and, if present, additional medical management to reduce the risk of adverse events.[29] Although this recommendation is based on several studies that have shown a beneficial effect of adding GLP-1 receptor agonists or SGTL2 inhibitors to the standard medical treatment in patients with both diabetes and PADs, it is still unclear whether this therapy should be further intensified in patients with polyvascular disease to reduce the additional risk of cardiovascular events.[[30], [31]].
Limitations
4.5
The four original randomized clinical trials were conducted with great care, including external monitoring and independent clinical event adjudication. Nevertheless, the present study has several limitations. Given the post-hoc nature of the analysis, the results should be regarded as hypothesis-generating. As is the case with all clinical studies, the presence of undetected or unmeasured confounders cannot be excluded. As a consequence of the definition of PADs used, undiagnosed and subclinical PADs were not considered. Similar to many other clinical studies, data on risk factors and comorbidities were collected from medical records and questionnaires at the time of enrollment in the randomized trials, while data on risk factors that might have developed during the period of follow-up were not available. Data on the number of affected vascular beds were not available in our database and could therefore not be assessed. In addition, detailed information on anti-diabetic therapy, besides insulin treatment, were not available.
Conclusion
5
In the high-risk population of PCI patients with polyvascular disease, the presence of diabetes represents a profoundly significant additional risk factor at long-term follow-up, associated with significantly higher adverse event risks – most evident in insulin-treated patients. Still, MACE was found to be primarily driven by all-cause mortality rather than device-related events or complications following PCI.
Ethics approval and consent to participate
The trials complied with the Declaration of Helsinki and were approved by the Medical Ethics Committee Twente (TWENTE reference number P08-18, DUTCH PEERS reference number P10-29, BIO-RESORT reference number P12-22; BIONYX reference number P15-19) and the Institutional Review Boards of all centers. All patients provided written informed consent.
Financial support
The present study was performed without any external funding. The department Cardiovascular Research and Education of Medisch Spectrum Twente has received institutional research grants provided by Abbott Vascular, Biotronik, Boston Scientific, and Medtronic, not related to the research question of the present study.
Artificial intelligence use
In the process of composing this manuscript, the authors employed the complimentary version of an artificial intelligence-based translation tool (DeepL; https://deepl.com) to evaluate some sentences, enhance the language level, and find alternative expressions. While this did enhance the readability of the manuscript, it did not affect the content.
CRediT authorship contribution statement
Daphne van Vliet: Writing – review & editing, Supervision, Investigation. Tineke H. Pinxterhuis: Writing – original draft, Visualization, Validation, Project administration, Methodology, Formal analysis. Eline H. Ploumen: Writing – review & editing, Visualization, Validation, Project administration, Methodology. Marlies M. Kok: Writing – review & editing, Supervision, Investigation. Rosaly A. Buiten: Writing – review & editing, Supervision, Investigation. Paolo Zocca: Writing – review & editing, Supervision, Investigation. Ariel Roguin: Writing – review & editing, Supervision, Investigation. Carl E. Schotborgh: Writing – review & editing, Supervision, Investigation. Rutger L. Anthonio: Writing – review & editing, Supervision, Investigation. Peter W. Danse: Writing – review & editing, Supervision, Investigation. Edouard Benit: Writing – review & editing, Supervision, Investigation. Adel Aminian: Writing – review & editing, Supervision, Investigation. Carine J.M. Doggen: Writing – review & editing, Supervision, Methodology, Conceptualization. Clemens von Birgelen: Writing – review & editing, Supervision, Investigation.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Vidakovic R.Schouten O.Kuiper R.The prevalence of polyvascular disease in patients referred for peripheral arterial disease Eur J Vasc Endovasc Surg 38200943544010.1016/j.ejvs.2009.05.00619560948 · doi ↗ · pubmed ↗
- 2Morikami Y.Natsuaki M.Morimoto T.Impact of polyvascular disease on clinical outcomes in patients undergoing coronary revascularization: an observation from the CREDO-Kyoto Registry Cohort-2Atherosclerosis 2228201342643110.1016/j.atherosclerosis.2013.04.00523623262 · doi ↗ · pubmed ↗
- 3Gutierrez J.A.Aday A.W.Patel M.R.Jones W.S.Polyvascular disease: reappraisal of the current clinical landscape Circ Cardiovasc Interv 12122019 e 00738510.1161/CIRCINTERVENTIONS.119.007385 PMC 766052631833412 · doi ↗ · pubmed ↗
- 4Suárez C.Zeymer U.Limbourg T.REACH Registry investigators. Influence of polyvascular disease on cardiovascular event rates. Insights from the REACH Registry Vasc Med 154201025926510.1177/1358863 X 1037329920724374 · doi ↗ · pubmed ↗
- 5Kobo O.Saada M.von Birgelen C.Impact of multisite artery disease on clinical outcomes after percutaneous coronary intervention: an analysis from the e-Ultimaster registry Eur Heart J Qual Care Clin Outcomes.942023 Jun 214174263587664610.1093/ehjqcco/qcac 043PMC 10284265 · doi ↗ · pubmed ↗
- 6Ramzy J.Andrianopoulos N.Roberts L.Melbourne Interventional Group (MIG). Outcomes in patients with peripheral vascular disease following percutaneous coronary intervention Catheter. Cardiovasc. Interv.9442019 Oct 158859710.1002/ccd.2814530790432 · doi ↗ · pubmed ↗
- 7Nikolsky E.Mehran R.Mintz G.S.Impact of symptomatic peripheral arterial disease on 1-year mortality in patients undergoing percutaneous coronary interventions J. Endovasc. Ther.1112004 Feb 607010.1177/15266028040110010814748627 · doi ↗ · pubmed ↗
- 8Van Der Meer M.G.Cramer M.J.Van Der Graaf Y.Appelman Y.Doevendans P.A.Nathoe H.M.The impact of polyvascular disease on long-term outcome in percutaneous coronary intervention patients Eur. J. Clin. Invest.4420142312392437246710.1111/eci.12222 · doi ↗ · pubmed ↗