German cranial reconstruction registry – a prospective multicenter cohort study: 883-day follow-up on the outcome and complications
Maximilian Bschorer, Henrik Giese, Julius Höhne, Karl Michael Schebesch, Christian Henker, Andreas Strauss, Christina Wolfert, Khaled Gaber, Aleksandrs Krigers, Ondra Petr, Vicki M. Butenschoen, Sandro M. Krieg, Klaus Christian Mende, Dirk Lindner, Jan Regelsberger

TL;DR
This study tracks long-term outcomes and complications of cranioplasty surgery in 200 patients, finding a 25% surgical revision rate and factors that predict better or worse outcomes.
Contribution
The study provides new insights into predictors of surgical revision and favorable neurological outcomes following cranioplasty.
Findings
The surgical revision rate after cranioplasty was 25%.
Suction drains were associated with a lower long-term surgical revision rate.
Simultaneous ventriculoperitoneal shunt placement increased the likelihood of surgical revision.
Abstract
This international prospective multicenter cohort study investigates the long-term surgical complication rate and neurological outcomes in patients who underwent autologous or allogeneic cranioplasty (CP) after decompressive craniectomy (DC) for traumatic brain injury, stroke, aneurysmatic subarachnoid hemorrhage, and intracranial hemorrhage. This study investigated the predictors of long-term outcomes and surgical revision after cranioplasty. Patients who underwent CP with a minimum follow-up of at least 12 months were included. Favorable long-term outcome (FLTO) was defined as a Glasgow Outcome Score (GOS) of 4 or 5 and a modified Rankin scale (mRS) score of <4. Univariate and multivariate analyses were performed. A total of 200 patients with a median follow-up of 883.1 ± 520.5 days were included. Ninety-nine patients (50.0 %) had a FLTO, and the surgical revision rate was 25.0 %…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
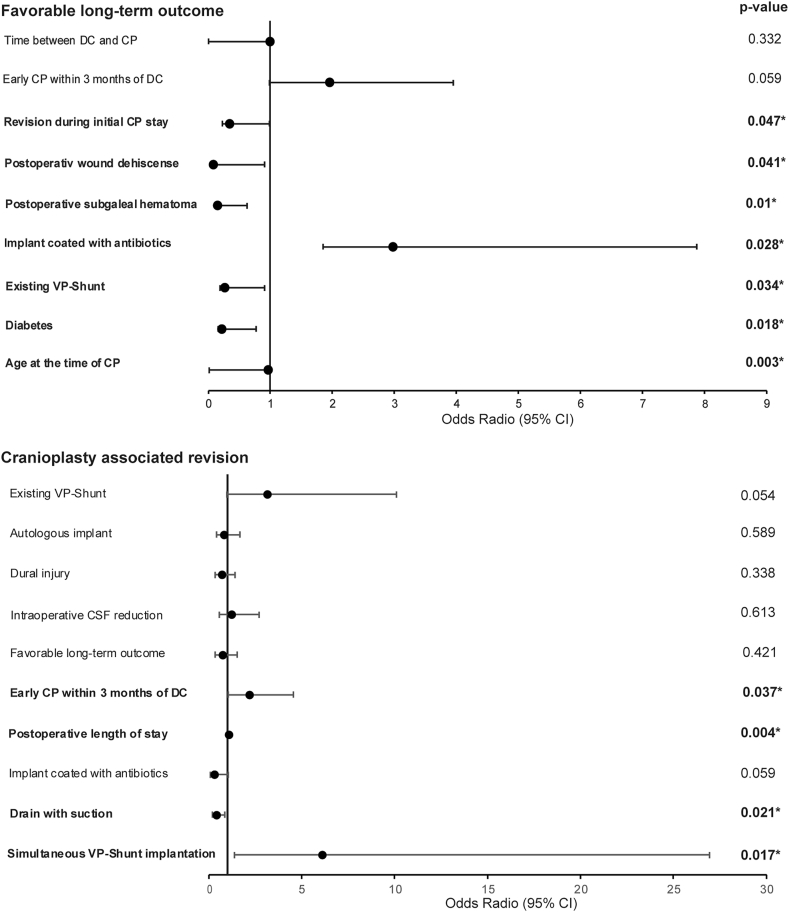 Figure 1
Figure 1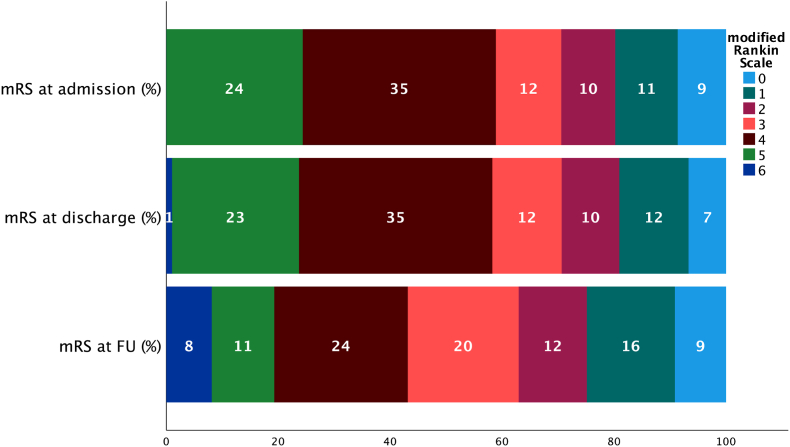 Figure 2
Figure 2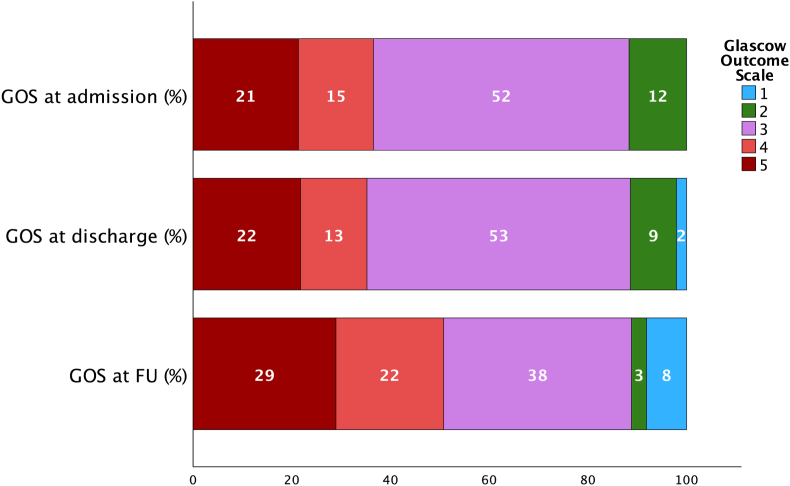 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTraumatic Brain Injury and Neurovascular Disturbances · Spinal Fractures and Fixation Techniques · Craniofacial Disorders and Treatments
Introduction
1
Decompressive hemicraniectomy (DC) is performed to prevent an imminent loss of brain function due to refractory intracranial pressure after malignant infarction of the middle cerebral artery, diffuse traumatic brain injury (TBI), intracerebral hemorrhage (ICH), and aneurysmal subarachnoid hemorrhage (ASAH) (Vahedi et al., 2007; Cooper et al., 2011). Despite improved survival rates, patients often suffer from neurocognitive and neurological deficits for the rest of their lives and often have to undergo further neurosurgical procedures such cranioplasty (CP) and ventriculoperitoneal shunt (VPS) placement. (Cooper et al., 2011). Cranioplasty (CP) has become an important cornerstone in modern neurological rehabilitation because an increase in cerebral perfusion, normalization of cerebrospinal fluid (CSF) hydrodynamics, and intracranial pressure (ICP) can improve the long-term neurological outcomes of patients (Fodstad et al., 1984; Halani et al., 2017; Shahid et al., 2018). CP has been linked to enhanced patient safety by reestablishing a protective barrier that shields the brain parenchyma from external impacts. Additionally, it addresses the increased risk of falls due to neurological morbidity and contributes to improved cosmetic outcomes (Giese et al., 2021).
The German Cranial Reconstruction Registry (GCRR) is a prospective multicenter cohort study with the goal of analyzing postoperative neurological outcomes and the risk of complications after CP (Giese et al., 2015). The initial report on postoperative complications after CP reported a surgical revision rate of 9 % within the first 30 days after CP (Sauvigny et al., 2021). Other studies have also reported a high risk of complications associated with neurosurgical procedures, despite many surgeons deeming it a routine and technically unchallenging procedure (Zanaty et al., 2015). While the general morbidity of patients who undergo DC is a factor, surgical aspects such as large wounds and the head microbiome contribute to the unfavorable risk profile of this type of surgery (Chang et al., 2010).1
This poses an ethical dilemma. Patients with severe neurological impairments and other clinical risk factors are presented with the option of CP, a procedure that carries significant perioperative risks, with the hope of both cosmetic and neurocognitive improvements. While there have been multiple prospective multicenter studies on the 30-day outcomes after CP, only retrospective data have been published so far on the long-term results after CP(Sauvigny et al., 2021; Fountain et al., 2021). The timing of CP following DC has been a subject of considerable debate within the neurosurgical community (Vreeburg et al., 2024). In this study, we present the long-term neurological and surgical outcomes of the patients analyzed in this prospective cohort study and aim to provide both patients and healthcare providers with information that may guide future clinical practice.
Methods
2
The section for Neurotrauma and Intensive Care in Neurosurgery of the German Society for Neurosurgery initiated the GCRR as a procedure-specific prospective cohort study (Giese et al., 2015). All cases of CP after DC at the 16 participating centers in Germany and Austria were screened for inclusion in the study. A standardized questionnaire on CP was used to record patient-specific data, including risk factors, surgical details, materials used for CP, intraoperative and postoperative complications, and clinical follow-up (FU) at discharge. The case report forms (CRF) for CP and postoperative monitoring were specifically designed to evaluate and address the questions of this study (Supplemental Digital Content 1). These forms were used to record all complications from the day of discharge to readmission within 30 days after surgery and again during follow-up by physicians at participating centers (Sauvigny et al., 2021). Neurological status and medical comorbidities were assessed using two different outcome scales: the modified Rankin Scale (mRS) and Glasgow Outcome Score (GOS).
Local ethics committees approved this study for the participating hospitals. This study was conducted in accordance with the ethical standards of the Declaration of Helsinki. Written informed consent was obtained from the patient or the patient's authorized representative prior to inclusion. Pseudonymized data were collected centrally at the Department of Medical Biometry, Heidelberg, and transmitted to an electronic database. This trial was indexed in the German Clinical Trials Register (DRKSID no. DRKS00007931). The Universal Trial Number is U1111–1168–7425.
Only centers that reported on at least 50 % of patient cases with a minimum FU of at least 12 months were further analyzed to reduce bias. This aims to minimize selection bias due to loss of follow-up. In addition, only cases with valid data and a follow-up of at least 12 months were included in this analysis. The primary endpoint was defined as cranioplasty-associated reoperation (CPAR), which included any neurosurgical procedure after the initial CP, including VPS revision surgeries. The second primary endpoint was neurological outcome. A favorable long-term outcome (FLTO) is defined as a follow-up GOS greater than three and a mRS score less than four.
Statistical correlation of clinical data was performed using univariate analysis with the chi-square test, Mann-Whitney U test, or 2-sample t-test, depending on the distribution of the measurements. Cases of deviating statistical test results are indicated in the respective passages. Variables with significant p-values in the univariate analyses or clinical relevance were considered as potentially independent variables in the multivariate analysis. Odds ratios and 95 % confidence intervals were calculated using logistic regression models. The regression models for both CPAR and LFTO were adjusted for age, diagnosis, and sex to specifically target the surgical aspects of CP. Pairwise deletion was used for the missing data. All statistical analyses were performed using IBM SPSS Statistics version 28 (IBM Corp.) under the supervision of a statistician.
Results
3
Patients
3.1
Eight of the 16 participating centers fulfilled the inclusion criteria. In total, 529 cases were initially reviewed for inclusion in the registry between September 2015 and December 2019. Overall, 200 patients fulfilled the inclusion criteria for the long-term analysis. The median follow-up was 883.1 ± 520.5 days. The average age of patients at the time of CP was 49.5 ± 16.07 years. The average age of patients receiving CAD and autologous implants was 47 and 52 years, respectively. Traumatic brain injury (TBI) (n = 82, 41.0 %) and ischemic stroke (n = 75, 37.5 %) were the most common reasons for DC, while intracerebral hemorrhage (ICH) (n = 38, 19.0 %) and subarachnoid hemorrhage (SAH) (n = 42, 21.0 %) were less common. Fourteen patients (7 %) had died at the time of the 12-month follow-up. CP was performed within 3 months in 37.3 % (n = 69) of the cases. The average number of days between DC and CP was 178.1 ± 220.7 days (Table 1) (Supplemental Digital Content 1).Table 1. Overview of patient (n = 200) characteristics; (DC = decompressive craniectomy, CP = cranioplasty, TBI = traumatic brain injury, ICH = intracranial hemorrhage, ASAH = aneurysmatic subarachnoid hemorrhage, CAD = computer aided design, CRAR = cranioplasty-associated reoperation, FLTO = favorable long-term outcome, ASA = American Society of Anesthesiologists).Table 1. Baseline characteristicN (%)CRARFLTOno (%)yes (%)p-valueunfavorable (%)favorable (%)p-valueSex.010.206 Female84 (42)92 (79)24 (21)50 (43)64 (56) Male116 (58)58 (69)26 (31)48 (57)36 (43)1st implantation.919.650 Yes159 (79.5)119 (75)40 (25)79 (50)78 (50) No41 (20.5)31 (76)10 (24)19 (46)22 (54)underlying condition.073<.001 TBI82 (41)60 (73)22 (27)24 (30)57 (70) ICH20 (10)15 (75)5 (25)14 (70)6 (30) Ischemic stroke72 (36)60 (83)12 (17)48 (68)23 (32) ASAH26 (13)15 (58)11 (42)12 (46)14 (54)ASA.001<.001 19 (5)8 (89)1 (11)1 (11)8 (89) 261 (34)50 (82)11 (18)13 (22)47 (78) 3102 (57)73 (72)29 (28)66 (65)36 (35) 47 (4)1 (14)6 (86)6 (86)1 (14)medical history & risk factors Hypertension91 (45.5)64 (70)27 (30).16357 (64)32 (36)<.001 Diabetes23 (11.5)17 (74)6 (26).89819 (83)4 (17)<.001 Smoker33 (16.5)27 (82)6 (18).32219 (58)14 (42).309 Alcohol10 (5)9 (90)1 (10).2616 (60)4 (40).495 Wound healing disorder25 (12.5)16 (64)9 (36).1759 (36)16 (64).149 Immunosuppression7 (3.5)6 (86)1 (14).5055 (71)2 (29).237 Coagulation disorder14 (7)11 (79)3 (21).7496 (43)8 (57).606 Other risk factors41 (20.5)37 (90)4 (10).01129 (73)11 (27).001 Coagulation affecting medication79 (40.9)65 (82)14 (18).05651 (66)26 (34)<.001 Sinking flap syndrome24 (12.2)147 (75)50 (25).14597 (49)98 (50).086 CP performed within 3 months of DC69 (37.3)46 (67)23 (33).02827 (40)41 (60).037Type of implant & material.935.002 Autologous bone93 (46.5)46 (67)23 (33)27 (40)41 (60) CAD107 (53.5)80 (75)27 (25)42 (39)65 (60) Polyetheretherketone12 (6)11 (92)1 (8)5 (42)7 (58) Polymethylmethacrylate23 (11.5)20 (87)3 (13)7 (30)16 (70) Ceramic4 (2)3 (75)1 (25)3 (75)1 (25) Titanium39 (19.5)24 (62)15 (38)16 (41)21 (59) Hydroxyapatite7 (3.5)6 (86)1 (14)2 (29)5 (71) Miscellaneous20 (9)15 (75)5 (25)8 (40)12 (60)
Rate of cranioplasty-associated reoperation (CPAR)
3.2
The rate of cranioplasty-associated reoperation (CPAR) in this long-term follow-up was 25 % (n = 50). There was no statistical difference in the surgical revision rate between allogenic and autologous implants. Of the 93 patients who received autologous bone transplants, 23 (25 %) underwent CPAR. Both univariate (p = .935) and multivariate (p = .589) analyses showed no significant correlation between the rate of reoperation and the implant material (p = .441). The most common reasons for CPAR were wound infection (n = 31, 15.6 %), aseptic bone resorption (n = 4, 3.0 %), and ventriculoperitoneal shunt-associated complications (n = 7, 3.5 %) (Table 2). In total, there were 22 (11.0 %) cases of aseptic bone resorption, with a revision rate of 18.2 % (n = 4) within the follow-up period. Neither the perioperative use of single-shot antibiotics (p = .070) nor the antibiotic coating of the implants (p = .057) predicted a higher rate of CPAR. The average duration of CP surgery was 130.7 ± 41.4 min; however, there was no correlation between the duration of surgery and the rate of reoperation (p = .197). Simultaneous VPS implantation (p = .017, 95 % CI, OR 1.387–26.947), early CP within three months of DC (p = .037, 95 % CI, OR 1.049–4.564), and a higher ASA score (p = .031, 95 % CI, OR 1.363–624.342) predicted an increased rate of surgical revision. The use of drains with suction predicted a lower rate of surgical revision (p .037, 95 % CI OR .298–.0964) (Table 3) (Fig. 1).Table 2. Complications requiring surgical revisions in long-term follow-up grouped by mplant type; (CAD – computer aided design).Table 2. Implant typeComplicationN (%)autologousNo revision69 (75 %)wound infection15 (16 %)Resorption4 (4 %)Pneumocephalus1 (1 %)Shunt associated complications/hydrocephalus3 (3 %)CADNo revision80 (75 %)wound infection18 (17 %)Epidural/subdural hematoma4 (5 %)Pneumocephalus1 (1 %)Shunt associated complications/hydrocephalus4 (4 %)Table 3. Cranioplasty-associated revision: Significant results of the multivariate logistic regression model for independent variables with cranioplasty-associated revision (CPAR) as the dependent variable: All variables were adjusted for age, sex, and diagnosis. ∗represents a statistically significant value of p < .05; (ASA = American society of anesthesiologists, DC = decompressive craniectomy, CP = cranioplasty, TBI = traumatic brain injury, ICH = intracranial hemorrhage, SAH = subarachnoid hemorrhage, VPS = ventriculoperitoneal shunt).Table 395 % CI for ORORLowerUpperp-valueSex1.542.7733.077.219TBI.087TBI vs ICH.710.2222.271.564TBI vs stroke.467.2061.060.069TBI vs SAH1.651.6374.277.302Age at the time of CP1.011.9901.033.302Simultaneous VPS implantation6.1141.38726.947**.017**∗Existing VPS3.143.97910.095.054ASA classification**.022**∗ASA I vs ASA II1.270.13811.673.833ASA I vs ASA III3.226.35929.014.296ASA I vs ASA IV29.1731.363624.342**.031**∗Drain with suction.410.193.874**.021**∗Any complication during hospitalization6.2432.79813.929< .001∗Early CP within 3 months of DC2.1891.0494.564**.037**∗Postoperative length of stay1.0771.0241.133**.004**∗Number of drains.536.298.964**.037**∗Fig. 1. Forest tree plot of the multivariate logistic regression model adjusted for diagnosis, age, and sex: relevant variables assessed in the German Cranial Reconstruction Registry (GCRR) analyzed for their predictive value of the long-term surgical revision rate (CPAR) and favorable long-term outcome (FLTO). (CP – cranioplasty, DC – decompressive craniectomy, VPS – ventriculoperitoneal shunt, CSF – cerebrospinal fluid).Fig. 1
Neurological outcome
3.3
The clinical performance indices indicated that 50 % (n = 100) of patients had favorable long-term outcomes. Of the patients, 37.7 % experienced an improvement in mRS score, and 27.5 % reported an improvement in GOS score (Table 4). In multivariate analysis, TBI was associated with FLTO (p = .001, 95 % CI, OR .127-.532), while an increase in age at the time of CP predicted a poorer functional outcome (p = .003, 95 % CI, OR .950-.990). There was no correlation between FLTO and the reoperation rate (p = .455). An overview of the mRS and GOS scores at admission, discharge, and follow-up is shown in Fig. 2, Fig. 3. Multivariate analysis showed that diabetes mellitus (p = .018, 95 % CI, OR .063-.774) and VPS (p = .034, 95 % CI, OR .077-.905) were variables that predicted unfavorable long-term neurological outcomes (Table 5) (Fig. 1).Table 4. Comparison of the mRS and the GOS at the time of discharge and follow-up.Table 4. Scorechangen%modified Rankin scale (mRS)no change7939.7 %improvement7537.7 %decline4522.6 %Glascow Outcome scale (GOS)no change11859.0 %improvement5527.5 %decline2713.5 %Fig. 2. The modified Rankin scale (mRS) at hospital admission for cranioplasty (CP) surgery, discharge and at the follow-up (mean follow-up 938 days), 0 – no symptoms, 1 - no significant disability, 2 – slight disability, 3 – moderate disability, 4 - moderately severe disability, 5- severe disability 6 – dead.Fig. 2. Fig. 3The Glasgow outcome score (GOS) at hospital admission for cranioplasty (CP) surgery, discharge and at the follow-up (mean follow-up 938 days), 1- dead, 2, - neurovegetative state, 3 – severe disability, 4 - moderate disability, 5 – good recovery.Fig. 3. Table 5Favorable long-term outcome: Significant results of the multivariate logistic regression model for independent variables with favorable long-term outcome (FLTO) as the dependent variable. All variables were adjusted for age, sex, and diagnosis. ∗represents a statistically significant value of p < .05; (ASA = American society of anesthesiologists, CP = cranioplasty, TBI = traumatic brain injury, ICH = intracranial hemorrhage, SAH = subarachnoid hemorrhage).Table 5OR95 % CI for ORLowerUpperp-valueSex1.338.7042.542.374TBI**.001**∗TBI vs ICH1.663.6434.300.294TBI vs stroke.403.1161.406.154TBI vs SAH.432.1661.120.084Age at the time of CP.969.950.990**.003**∗Revision during initial CP stay.347.122.985**.047**∗diabetes.221.063.774**.018**∗Postoperative wound dehiscence.085.008.907**.041**∗Autologous implant1.666.8753.171.120ASA classification**.001**∗ASA I vs ASA II.483.0484.858.537ASA I vs ASA III.115.0121.110.062ASA I vs ASA IV.035.001.812**.037**∗Implant with antibiotics2.9731.1227.876**.028**∗
Discussion
4
The long-term analysis of this prospective cohort study offers a comprehensive assessment of various factors, aimed at guiding the planning, perioperative, and postoperative care of patients who underwent DC. In this study, 50 % of the patients achieved favorable long-term outcomes, whereas 25 % required surgical revision.
An implanted ventriculoperitoneal shunt at the time of CP is a predictor of an increased risk of surgical revision within the initial 30-day period (Sauvigny et al., 2021). However, by applying regression models to patients from the same cohort in the 3-year-follow-up, the existence of a VP shunt failed to predict an increased risk of surgical revision. Owing to underlying pathologies, some patients require VPS placement when CP is indicated. The timing of VPS placement in relation to CP has been under review, with many authors favoring a two-stage procedure (Zhang et al., 2022). A recent Korean study showed a significant risk of VPS and CP complications with simultaneous implantation of both, which was associated with an even higher perioperative risk (Gill et al., 2021). Our study confirmed that simultaneous VPS implantation was predictive of a significant increase in CPAR. Hence, we suggest that these two procedures should be scheduled at two different time points, even if this necessitates additional surgery. The type of valve used in VP shunt surgeries, whether fixed pressure or programmable, was not investigated in this registry.
The role of drains with suction in CP has been a matter of debate in the past, based on insufficient evidence, such as case reports and expert opinions. For instance, there are multiple published cases of patient deaths after CP, in which the authors speculate that the use of drains with suction increases the risk of cerebral edema and death (Broughton et al., 2014; Anuzis et al., 2021). It has been suggested that the negative pressure difference in a large cavity, such as the epidural space, after CP, as well as the resulting brain shift, can cause cerebral edema (Sviri, 2015). The potential benefit of suction drains in CP is likely diminished when dural leaks are detected (Sporns et al., 2016). Others have claimed that this surgical technique minimizes the risk of postoperative epidural hematoma and wound infection (Raju et al., 2023). The results of this prospective study would suggest that the use of drains with suction lowers the overall risk of reoperation without affecting neurological outcomes or mortality. The questionnaire assessed the utilization of drains at the conclusion of surgery. It did not evaluate the placement of the drain (epidural or subgaleal) or the degree of suction applied to the drain. Within this cohort, there was no incidence of brain edema in patients who received suction drains during CP surgery.
The use of CP materials (usually polymethylmethacrylate) coated or imbued with antibiotics seems to predict a more favorable neurological outcome in the regression model of this study without affecting the rate of CPAR in its regression model. We attribute this effect to the small number of patients undergoing CP using antibiotic-coated implants (n = 15). Authors of previously published studies claimed that the antibiotic properties of these implants reduce the rate of postoperative wound infection and therefore lead to overall better neurological recovery (Worm et al., 2016; Lazar et al., 2016). Amendola et al. (2022) published a retrospective cohort study analyzing the antibiotic immersion of CP implants and claimed that this surgical technique led to a significant decrease in postoperative wound infection.
Corallo et al. (2021) showed a significant improvement in neuropsychological and cognitive abilities after CP in patients with TBI. While this study showed an overall improvement of the neurological outcome after CP, there was also a decline in mRS in 25 % and GOS in 12 % of the cases, respectively. A prospective Spanish study demonstrated an association between the timepoint after DC and the measurement of daily autonomy and age (Paredes et al., 2015). The authors observed an objective improvement in the Barthel index, an index used to assess autonomy in activities of daily living, by 40 % within days after CP. The findings of this study show an improvement in GOS and mRS scores of 7.5 % and 37.7 % after CP, respectively. Peredes et al. (Paredes et al., 2015) described a trend in which patients with TBI showed a higher degree of neurological improvement after CP, a finding that was also confirmed by our multivariate logistic regression model. This study did not show an association between implant type and long-term neurological outcomes after CP, independent of the patients’ age and diagnosis. This is despite the fact that neurosurgeons commonly recommend autologous implants for older patients, despite the risk of resorption and the associated risk of reoperation due to reduced life expectancy (Malcolm et al., 2018a).
The process of aseptic bone resorption after CP administration is not fully understood (Göttsche et al., 2021). A recent systematic review of autologous bone resorption showed that bone flap fragmentation, TBI, and younger age increase the risk of bone resorption (Signorelli et al., 2022). Neurosurgeons tend to recommend autologous cranioplasty for patients who accept the risk of bone resorption for a lower infection rate. Thus, non-autologous CP is often recommended for younger patients with greater life expectancy. The authors of a 2017 meta-analysis described a trend of lower explantation rates when comparing CAD implants and autologous bone grafts. They determined a CAD implant failure rate of 8–31 % (Punchak et al., 2017). However, there was no significant increase in the surgical revision rate and no effect on the long-term neurological outcome when comparing cases of autologous and non-autologous implants in this study.
Yang et al. (2018) published the results of a retrospective multicenter study including patients who underwent CP after DC for TBI. The authors argued in favor of early CP within 34 days after DC and showed a correlation between early CP and an improved 6-month GOS. In TBI, early CP is associated with increased cerebral perfusion (Rynkowski et al., 2021). A 2018 meta-analysis indicated that early CP was associated with greater neurological improvement than that with delayed CP (Malcolm et al., 2018b). Vreeburg et al. suggested that early CP, even within the initial hospital stay, in which DC was performed, does not have an increase in rate of complication (Vreeburg et al., 2024). This study, however, suggests that patients who underwent CP within 90 days had a higher revision rate than patients who underwent late CP without a significant impact on neurological outcomes. The healing of the surgical wound after DC, stabilization of CSF fluid dynamics, and recovery from the underlying disease that led to DC may play a role in favoring delayed CP. The economic feasibility of countries such as Germany and Austria, which can finance lengthy rehabilitation processes for patients, may also play a part in this debate. Lastly, in this study, there was no correlation between the syndrome of the trephine and the timing of CP.
Limitations
4.1
To our knowledge, this is the only published prospective multicenter study with a follow-up of multiple years after CP. The strength of this study lies in its prospective and multicenter-based design. Unfortunately, more than half of all patient cases were lost to long-term follow-up and therefore had to be excluded. The low mortality rate is likely also linked to loss to follow-up. The heterogeneity of surgical practice, not only among neurosurgical departments but also among surgeons, can be a confounding variable in our study. Although this study is multinational, it only represents common practices in German-speaking countries, Austria and Germany.
Conclusion
5
This prospective multicenter study suggests that the use of drains with suction is associated with a lower long-term rate of surgical revision after CP, whereas simultaneous VPS implantation increases the risk of surgical revision. Antibiotic coating of implants predicted a FLTO.
Statement
During the preparation of this work, the authors used Microsoft Copilot and Paperpal in order to increase fluency, grammar and spelling of the text. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Declaration of conflicting interests
The German cranial reconstruction registry was funded by 3di GmbH, Skulle implants, OssDsign, 10.13039/100008127DePuy Synthes Spine and the ZNS – 10.13039/501100007731Hannelore Kohl Stiftung.
The authors have no other conflicts to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Amendola F.Vaienti L.Carbonaro R.Nataloni A.Barbanera A.Zingaretti N.Pier C.P.Zanotti B.The antibiotic immersion of custom-made porous hydroxyapatite cranioplasty: a multicentric cohort study J. Craniofac. Surg.3320221464146810.1097/SCS.000000000000836335165242 · doi ↗ · pubmed ↗
- 2Anuzis A.Doherty J.A.Millward C.P.Sinha A.K.Mc Mahon C.J.Sudden death associated with the use of suction drains - a report of 2 cases following uneventful cranioplasty and literature review. Is the use of suction drains safe?Br. J. Neurosurg.202110.1080/02688697.2021.187277633464139 · doi ↗ · pubmed ↗
- 3Broughton E.Pobereskin L.Whitfield P.C.Seven years of cranioplasty in a regional neurosurgical centre Br. J. Neurosurg.282014343910.3109/02688697.2013.81531923875882 · doi ↗ · pubmed ↗
- 4Chang V.Hartzfeld P.Langlois M.Mahmood A.Seyfried D.Outcomes of cranial repair after craniectomy J. Neurosurg.11220101120112410.3171/2009.6.JNS 0913319612971 · doi ↗ · pubmed ↗
- 5Cooper D.J.Rosenfeld J.V.Murray L.Arabi Y.M.Davies A.R.D'Urso P.Kossmann T.Ponsford J.Seppelt I.Reilly P.Wolfe R.Decompressive craniectomy in diffuse traumatic brain injury N. Engl. J. Med.36420111493150210.1056/NEJMOA 110207721434843 · doi ↗ · pubmed ↗
- 6Corallo F.Lo Buono V.CalabròR.S.De Cola M.C.Can cranioplasty be considered a tool to improve cognitive recovery following traumatic brain injury? A 5-Years retrospective study J. Clin. Med.10202110.3390/JCM 10225437 PMC 862455434830718 · doi ↗ · pubmed ↗
- 7Fodstad H.Love J.A.Ekstedt J.Fridén H.Liliequist B.Effect of cranioplasty on cerebrospinal fluid hydrodynamics in patients with the syndrome of the trephined Acta Neurochir.701984213010.1007/BF 01406039(Wien)6741628 · doi ↗ · pubmed ↗
- 8Fountain D.M.Henry J.Honeyman S.O'Connor P.Sekhon P.Piper R.J.Edlmann E.Martin M.Whiting G.Turner C.Mee H.Joannides A.J.Kolias A.G.Hutchinson P.J.Williams A.Sinha A.Leggate A.Belli A.Bahl A.Mc Mahon C.Tolias C.Holsgrove D.O'Brien D.Bulters D.George E.S.Critchley G.James G.Akram H.Pollock J.Prasad M.Ganau M.Wilson M.Hossain-Ibrahim M.Bodkin P.Whitfield P.Mathew R.K.Joshi S.Achawal S.Harrisson S.Smith S.Lawrence T.Al-Tamimi Y.Commit S.Bell A.Shaw S.Brennan P.M.Anderson I.Jamjoom A.A.B.Shoakazemi A.Khan A.Kadhim A.Edwards-Bailey A.Bjornson A.Roylance A · doi ↗ · pubmed ↗