Arrhythmic mitral annular disjunction or not arrhythmic mitral annular disjunction: that is the problem?
Annagrazia Cecere, Martina Perazzolo Marra

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
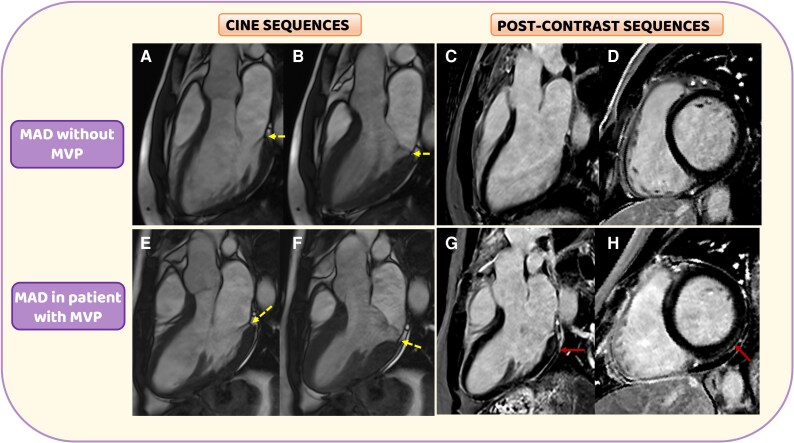 Figure 1
Figure 1 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Cardiovascular Function and Risk Factors · Cardiac Arrhythmias and Treatments
This editorial refers to ‘A tale of two MADs: a case series’, by K. Stankowski et al. https://doi.org10.1093/ehjcr/ytaf266.
Recently, the mitral annular disjunction (MAD) aroused great interest in the scientific community regarding its prevalence and arrhythmic role in patients with mitral valve prolapse (MVP). The role of MAD is traditionally considered as part of morphological features of MVP; however, the variability between different imaging techniques remains a limitation for large population study. First described by Bharati et al.^1^ in a 45-year-old woman with arrhythmic MVP died suddenly, MAD is an abnormal atrial displacement of the posterior mitral leaflet hinge point. Hutchins et al.,^2^ analysing a single block of atrioventricular tissue, identified this anatomical disjunction in 23/25 hearts with bileaflet MVP, speculating on the essential MAD role in the leaflet redundancy. However, after few years, Angelini et al.,^3^ considering the entire atrioventricular junctions in 13 hearts, recognized MAD in 12 of them. So, MAD gave the impression to be an anatomical variation of the mitral annulus, also evident in normal hearts (Figure 1A–D).
Beyond its anatomic role, the presence of MAD recently emerged as a crucial risk factor for arrhythmogenesis in MVP patients. Carmo et al.^4^ demonstrated that the length of MAD correlated with the occurrence of non-sustained ventricular tachycardia on Holter monitoring in MVP patients. Dejgaard et al.^5^ assumed that the only presence of MAD, regardless of the occurrence of MVP, was strongly associated with a greater arrhythmic risk, suggesting an independent role of the MAD in the arrhythmogenesis.
In a retrospective analysis of sudden cardiac deaths in young patients in Veneto region, MAD resulted correlated with an abnormal systolic motion of the left ventricular (LV) basal inferolateral wall, well known as curling, and fibrosis.^6^ So, it was hypothesized that this anatomical separation between posterior mitral leaflet and LV myocardium, acting as substrate, could promote a mechanical stress (trigger) on one side on the mitral valve, responsible for myxomatous degeneration and progressive valve incompetence, and on the other on the LV basal inferolateral wall resulting, time by time, in a replacement-type fibrosis, evaluated through late gadolinium enhancement (LGE) in cardiac magnetic resonance (CMR)^7^ (Figure 1E–H).
After about 10 years from the first recognition of its pro-arrhythmic role, Essayagh et al.^8^ demonstrated that MVP patients with MAD (186/595, 31%) presented a more severe phenotypical spectrum of mitral disease (bileaflet MVP, leaflet redundancy, and great LV volumes), suggesting a progressive myxomatous degeneration. In this study, MAD emerged as an independent risk factor for arrhythmic events, even if, intriguingly, in a 10-year follow-up, MAD was not associated to a reduced overall survival. The case series presented by Stankowski et al.^9^ underlined the criticisms about the arrhythmic role of MAD. They presented two different clinical scenarios of echographically diagnosed MAD in young patients. In the first case, MAD was diagnosed in a 31-year-old woman, presenting exertional syncope and palpitations, without electrocardiogram abnormalities. Echocardiography revealed normal biventricular dimensions and function. A single-leaflet non-classic MVP with a 3-mm inferolateral MAD and a trivial mitral regurgitation was also recognized. No systolic curling or focal/microscopic myocardial fibrosis was found in the CMR. Conversely, in the second case, MAD was identified in a 32-year-old man with an aborted sudden cardiac death due to ventricular fibrillation, occurred after a run. In this case, a 10-mm inferolateral MAD was associated to a bileaflet MVP with systolic curling, positive Pickelhaube sign, moderate mitral regurgitation, and left chamber’s dilation. T-wave inversion in the inferolateral leads was also observed. CMR revealed increased T1 mapping values in the LV basal inferolateral wall without focal macroscopical LGE.
Confirming the strongly debated issues on the arrhythmic role of MAD, the great value of this case series is the suggestion to shift the clinician’s attention from the particular (MAD) to the general (patient’s clinical presentation). First of all, Stankowski et al.^9^ confirmed the MAD diagnosis does not equivalent to the occurrence of an arrhythmic event because it could be also identified in normal hearts.^3,10^ Accordingly, not all the MAD localizations are equivalent. Zugwitz et al.^11^ recently confirmed that, despite MAD is a common CMR finding in general population (1990/2607 patients with MAD, 76%), the inferolateral location, strongly associated with curling (24/134, 17.9%), was quite rare (134 patients, 5.1%). So, in order to avoid a misinterpretation of its potential arrhythmic role, it is essential to include the MAD identification in the general patient’s clinical scenario, paying careful attention to the personal and family history, electrocardiographic features, and imaging findings. In fact, in the second case presented by Stankowski et al.,^9^ MAD was associated to an aborted sudden cardiac death, inferolateral T-wave inversion, systolic curling, mitral regurgitation, left chamber’s dilation, and microscopic fibrosis, just recognized as ‘arrhythmic red flags’.^12^ Conversely, the only diagnosis of MAD, in absence of suggestive clinical and instrumental arrhythmic features, demonstrated to have a limited value in the arrhythmic risk stratification.^8–9^ In a recent study, we evaluated the determinants of ventricular arrhythmias (VAs) in 108 arrhythmic MVP patients without valve regurgitation.^13^ A mediation analysis intriguingly revealed that only curling had a direct and indirect, mediated by LGE, effect on VAs. Conversely, the pro-arrhythmic role of MAD was completely mediated by myocardial fibrosis. Supporting this concept, a reduction of the mechanical LV stress with a surgical insertion of a ring/prosthesis on the mitral annulus could have an impact on the VAs burden reduction because overcomes the disjunction.^8^ However, considering the actual surgical indication in patients with severe mitral regurgitation with symptoms or LV dysfunction, the potential anti-arrhythmic effect of a MV repair in MVP patients with MAD and no significant regurgitation are just speculative.
In conclusion, the arrhythmogenic role of MAD should be carefully considered on the basis of clinical scenario and instrumental findings because it emerged as an epiphenomenon without a direct effect on arrhythmogenesis in MVP patients.^13^ Conversely, curling, as the expression of the abnormal LV myocardium contraction, could act as primum movens in the mechanical stress, demonstrated in MVP patients, and it could be directly responsible for arrhythmogenesis.^13^
Further studies will be necessary to confirm this clinical-oriented approach to the MAD identification in MVP patients, but this case series raises important steps in this direction.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bharati S, Granston AS, Liebson PR, Loeb HS, Rosen KM, Lev M. The conduction system in mitral valve prolapse syndrome with sudden death. Am Heart J 1981;101:667–670.7223606 10.1016/0002-8703(81)90235-0 · doi ↗ · pubmed ↗
- 2Hutchins GM, Moore GW, Skoog DK. The association of floppy mitral valve with disjunction of the mitral annulus fibrosus. N Engl J Med 1986;314:535–540.3945291 10.1056/NEJM 198602273140902 · doi ↗ · pubmed ↗
- 3Angelini A, Ho SY, Anderson RH, Becker AE, Davies MJ. Disjunction of the mitral annulus in floppy mitral valve. N Engl J Med 1988;318:188–189.3336409 10.1056/NEJM 198801213180315 · doi ↗ · pubmed ↗
- 4Carmo P, Andrade MJ, Aguiar C, Rodrigues R, Gouveia R, Silva JA. Mitral annular disjunction in myxomatous mitral valve disease: a relevant abnormality recognizable by transthoracic echocardiography. Cardiovasc Ultrasound 2010;8:53.21143934 10.1186/1476-7120-8-53PMC 3014886 · doi ↗ · pubmed ↗
- 5Dejgaard LA, Skjølsvik ET, Lie ØH, Ribe M, Stokke MK, Hegbom F, et al The mitral annulus disjunction arrhythmic syndrome. J Am Coll Cardiol 2018;72:1600–1609.30261961 10.1016/j.jacc.2018.07.070 · doi ↗ · pubmed ↗
- 6Basso C, Perazzolo Marra M, Rizzo S, De Lazzari M, Giorgi B, Cipriani A, et al Arrhythmic mitral valve prolapse and sudden cardiac death. Circulation 2015;132:556–566.26160859 10.1161/CIRCULATIONAHA.115.016291 · doi ↗ · pubmed ↗
- 7Perazzolo Marra M, Basso C, De Lazzari M, Rizzo S, Cipriani A, Giorgi B, et al Morphofunctional abnormalities of mitral annulus and arrhythmic mitral valve prolapse. Circ Cardiovasc Imaging 2016;9:e 005030.27516479 10.1161/CIRCIMAGING.116.005030 PMC 4991345 · doi ↗ · pubmed ↗
- 8Essayagh B, Sabbag A, Antoine C, Benfari G, Batista R, Yang LT, et al The mitral annular disjunction of mitral valve prolapse: presentation and outcome. JACC Cardiovasc Imaging 2021;14:2073–2087.34147457 10.1016/j.jcmg.2021.04.029 · doi ↗ · pubmed ↗