Regressing calcifications in the carotid artery: What’s going on? A case series
Dianne H.K. van Dam-Nolen, Taihra Zadi, M. Eline Kooi, Jeroen Hendrikse, Paul J. Nederkoorn, Aad van der Lugt, Daniel Bos

TL;DR
This case series reports a surprising decrease in carotid artery calcifications over two years in three elderly men, challenging the belief that calcifications only progress or stay the same.
Contribution
The study introduces the novel observation that carotid calcifications may regress, potentially impacting atherosclerosis prevention strategies.
Findings
Three patients showed reduced carotid calcifications over a 2-year period.
The observed calcification regression challenges the assumption that calcifications only progress or stabilize.
The phenomenon may have implications for understanding and managing atherosclerosis and stroke prevention.
Abstract
This case series describes a finding that carotid calcifications could decrease during follow-up, as the predominant idea is that calcifications either progress or stabilize over time. This novel finding is of great interest considering that potential regression of calcifications could affect prevention strategies for atherosclerosis and ischemic stroke. We describe 3 patients (3 men, age ranging from 72 to 75 years) with decrease in carotid calcifications during 2-year follow-up. All 3 patients had macrocalcifications and used different medications during follow-up. This remarkable finding gives new insights in the natural course of atherosclerosis as a main cause of ischemic stroke. Further study is needed to investigate whether this is a harmful or beneficial process and to unravel pathophysiological mechanisms.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
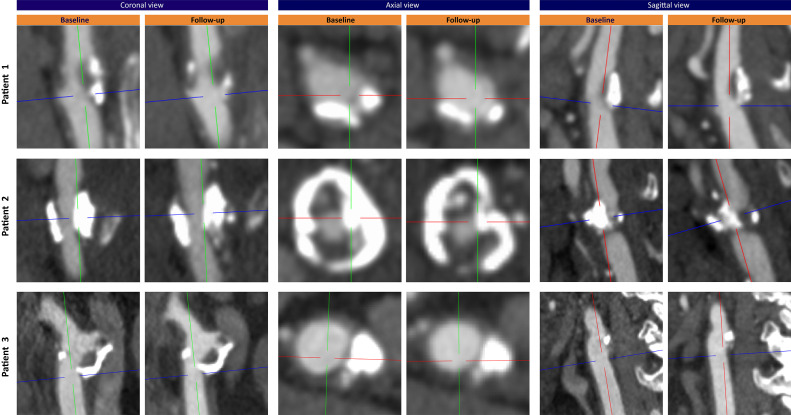 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCerebrovascular and Carotid Artery Diseases · Cardiovascular Health and Disease Prevention · Oropharyngeal Anatomy and Pathologies
Background
Carotid atherosclerosis is a major cause of ischemic stroke, and thereby contributes to considerable morbidity and mortality [1,2]. Atherosclerotic carotid plaques vary greatly in size, composition, and structure, but the presence of calcifications is very common in more advanced plaques [3,4]. Over the years, the presence and amount of calcifications has often served as a marker of atherosclerotic disease and as a risk indicator of stroke events, but its relation with cardiovascular risk remains complex [5,6]. The predominant hypothesis regarding calcifications is that these generally either progress or stabilize over time, yet, evidence for this hypothesis from serial imaging studies remains scarce. Recently, we found that carotid calcifications could also decrease during follow-up. The aim of this case series is to explore and discuss this novel finding, in the belief that this could be of great interest considering that potential regression of calcifications could affect prevention strategies.
Case presentation
An overview of patients’ clinical characteristics at baseline and medication use are shown in Table 1. Table 2 shows the plaque characteristics at baseline. In Figure 1 CTA images in axial, sagittal, and coronal views are compared for baseline and follow-up. We performed state-of-the-art carotid plaque imaging at baseline and after 2 years follow-up using contrast-enhanced CTA and MRI [7]. We assessed extracranial carotid artery calcification (ECAC) volumes within 3 cm proximal and distal to the carotid bifurcation with a custom-made plug-in for the software ImageJ (National Institutes of Health, Bethesda, Maryland). A threshold of 600 Hounsfield units was used to differentiate calcifications from contrast material.Table 1. Clinical characteristics of patients with decrease in ECAC during 2-year follow-up.Table 1. VariablePatient 1Patient 2Patient 3Clinical characteristics at baselineAge, years727572SexMaleMaleMaleEthnicityCaucasianCaucasianCaucasianDiabetes mellitusNoNoNoHypertensionNoYesYesHypercholesterolemiaNoYesYesBMI, kg/m^2^24.124.336.2SmokerFormerFormerFormerAlcohol abuseNoNoNoHistory of CVDYesaNoYesbHistory of malignancyNoNoYescLaboratory values at baselineLDL (mg/dL)96.7100.5189.5HDL (mg/dL)61.944.138.7Triglycerides (mg/dL)125.888.6372.0Total cholesterol (mg/dL)185.6162.4274.6Lipoprotein(a) (mg/dL)Unknown59.83.0Medication use at discharged- Alimentary tract and metabolismOmeprazoleHydrocortisonePantoprazole- Blood and blood-forming organsClopidogrelCarbasalate calciumDipyridamoleCarbasalate calciumDipyridamole- Cardiovascular systemSimvastatinLisinoprilSimvastatinMetoprololSimvastatin- Genito-urinary system and sex hormonesTamsulosinTestosterone- Hormonal preparations, excl. sex hormones and insulinsLevothyroxine- Anti-infectives for systemic useCotrimoxazole- Nervous systemPrimidoneaPrevious amaurosis fugax.bIschemic heart disease and peripheral artery disease.cPituitary metastasis of unknown primary tumor which was treated with stereotactic radiotherapy.dAt discharge when treated for their baseline event.BMI, body mass index; CVD, cardiovascular disease; LDL, low-density lipoprotein; HDL, high-density lipoprotein.Table 2. Plaque characteristics at baseline of patients with decrease in ECAC during 2-year follow-up.Table 2. VariablePatient 1Patient 2Patient 3Side of plaqueRightRightLeftPlaque ipsilateral to index eventYesYesNoPlaque size Degree of stenosis (ECST, %)a658119 Degree of stenosis (NASCET, %)a20400 Total plaque volume (mm^3^)b12382086870Plaque components Presence of calcificationsaYesYesYes Percentage of calcificationsa14.7%14.4%17.8% Presence of lipid-rich necrotic corebYesYesNo Percentage of lipid-rich necrotic coreb12.7%3.9%n.a. Presence of intraplaque hemorrhagebYesNoNo Percentage of intraplaque hemorrhageb7.9%n.a.n.a.Plaque morphology Plaque ulcerationaNoNoNo Thin-or-ruptured fibrous capbYesNoNoaDegree of stenosis, percentage and presence of calcifications, and plaque ulceration are assessed with CTA.bTotal plaque volume presence and percentage of lipid-rich necrotic core and intraplaque hemorrhage, and thin-or-ruptured fibrous cap are assessed with MRI.ECST, European Carotid Surgery Trial; NASCET, North American Symptomatic Carotid Endarterectomy Trial.Fig. 1. Baseline and follow-up CTA of patients with decreasing ECAC. CTA images in axial, sagittal, and coronal views at baseline and 2-year follow-up of patients with decrease in ECAC.Fig 1
Patient 1
The first patient is a 72-year-old, formerly smoking man with a medical history of amaurosis fugax. He was admitted to the hospital with an ischemic stroke in the right hemisphere. Carotid MRI at baseline showed an ipsilateral plaque with calcifications, a lipid-rich necrotic core (LRNC) including intraplaque hemorrhage (IPH), and a thin-or-ruptured fibrous cap (TRFC), causing a stenosis of 65% (according to the European Carotid Surgery Trial criteria). We found that the calcification decreased during follow-up (baseline ECAC volume: 64.7 mm^3^; follow-up ECAC volume: 35.3 mm^3^), predominantly in the proximal region of the plaque. The distal part of the plaque conversely showed larger calcifications at the follow-up scan.
Patient 2
The second patient concerns a 75-year-old, formerly smoking, male patient with hypertension and hypercholesterolemia. He was referred to the out-patient clinic due to a right-sided amaurosis fugax. At baseline he had an ipsilateral carotid plaque with calcifications and a small LRNC, without IPH, causing a stenosis of 81%. During follow-up the calcification decreased, especially in the bulk of the plaque (baseline ECAC volume: 288.6 mm^3^; follow-up ECAC volume: 127.1 mm^3^). However, new IPH and an increased LRNC (from 3.9 to 10.8%; 80.8 to 154.6 mm^3^) was found at the follow-up scan.
Patient 3
The third patient is a 72-year-old, formerly smoking, male patient, also with hypertension and hypercholesterolemia. He was admitted to the hospital with a TIA in the right hemisphere. During follow-up he had decrease in calcifications in the contralateral carotid plaque (baseline ECAC volume: 364.9 mm^3^; follow-up ECAC volume: 203.8 mm^3^). At baseline, this plaque was composed of only calcifications and fibrous tissue, causing a stenosis of 19%. The decrease in calcification was seen in all regions of the plaque (Fig. 1 shows decrease in the proximal region). It seemed that in the ipsilateral plaque also some decrease in calcifications occurred during follow-up, but it was not that evident as on the contralateral side.
Discussion and conclusions
We found that carotid calcifications can regress over time. This is a new and remarkable finding. Although previous studies have described carotid plaque regression (often to evaluate statin therapies) [8,9], no studies have explicitly reported about carotid calcification regression. In the coronary field, studies particularly focusing on statin use have shown that coronary calcifications could both decrease and increase [10,11]. However, it is important to realize that the development of calcifications may differ across different vessel beds within 1 individual, as evidenced by merely weak-to-moderate correlations [12,13].
Increase in calcifications have possible stabilizing effects [10]. It is believed that especially macrocalcifications rather than micro or spotty calcifications contribute to these potential protective effects [14]. All 3 patients in our study had macrocalcifications which makes the finding of a decrease in calcifications more intriguing.
The process of calcifications is enigmatic. Multiple factors like lipoproteins and inflammatory cells play a role and medications could have pleiotropic effects. There are some notable clues in our case series. First, the third patient used long-term hydrocortisone during the whole follow-up because of a pituitary tumor. We hypothesize that the use of anti-inflammatory medication could be a factor mitigating carotid calcifications. Based on previous literature, we already know that anti-inflammatory medication might delay atherosclerosis progression [15], yet it may also cause decrease in calcifications. The fact that decrease was seen in the whole plaque and possibly on both sides, strengthens this idea. Secondly, 2 patients (no. 1 and 2) had low LDL levels while using statins. Raggi et al. reported in a study among patients without manifest coronary artery disease that only in treated patients who achieved an LDL level <120 mg/dL calcification regression was seen [16]. The use of statins and relatively low LDL levels in these 2 patients may have contributed to the calcification decrease. However, it is remarkable that this happened in probable late-stage macrocalcification. Besides this, the decrease in calcifications happened in 2 patients (no. 1 and 2) at specific regions of the calcification, suggesting a more local process or suggesting that the calcification at those points was more sensitive for changing due to an earlier stage. It is obvious that our findings provide more questions than answers.
Besides the question about the pathophysiology, these findings also raise the question whether regressing calcifications are beneficial or harmful. When total plaque size is regressing it could be a beneficial process reducing the risk of stroke. However, when calcifications are decreasing but components like IPH and LRNC are increasing, the plaque could become more vulnerable and prone to rupture. In light of preventing stroke and new therapies, it is important to investigate these questions further and more deeply in future research and in larger cohorts.
In conclusion, in this case series, we showed 3 examples of decreasing carotid calcifications during follow-up which gives new insights in the natural course of atherosclerosis. This remarkable finding needs to be validated in other and larger multicenter cohorts and studied further to investigate whether this is a harmful or beneficial process and to unravel underlying pathophysiological mechanisms.
Ethics approval and consent for participate
Institutional Review Board approval was obtained (Medisch Ethische Commissie azM/UM, Maastricht, the Netherlands, approval number NL29116.068.09/MEC 09-2-082) and all patients gave written informed consent for participation in this study and for publication of collected information regarding their medical case and imaging. The study was performed in accordance with the principles of the Declaration of Helsinki.
Availability of data and materials
The data underlying this article cannot be shared publicly due to the privacy of individuals that participated in this study. The data will be shared on reasonable request to the corresponding author.
Author contributions
DvDN: Conceptualization, Formal analysis, Methodology, Writing—original draft, Visualization. TZ: Conceptualization, Formal analysis, Visualization. MEK: Funding acquisition, Writing—review and editing. JH: Funding acquisition, Writing—review and editing. PN: Funding acquisition, Writing—review and editing. AvdL: Funding acquisition, Supervision, Writing—review and editing. DB: Methodology, Supervision, Writing—review and editing.
Patient consent
Included patients gave informed consent for publication of collected information regarding their medical case and imaging in context of the PARISK study.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Roth G.A.Mensah G.A.CO Johnson Addolorato G.Ammirati E.Baddour L.M.Global burden of cardiovascular diseases and risk factors, 1990-2019: Update From the GBD 2019 Study J Am Coll Cardiol 76252020298230213330917510.1016/j.jacc.2020.11.010PMC 7755038 · doi ↗ · pubmed ↗
- 2Bos D.Arshi B.van den Bouwhuijsen Q.J.A.Ikram M.K.Selwaness M.Vernooij M.W.Atherosclerotic carotid plaque composition and incident stroke and coronary events J Am Coll Cardiol 77112021142614353373682510.1016/j.jacc.2021.01.038 · doi ↗ · pubmed ↗
- 3van Dam-Nolen D.H.K.van Egmond N.C.M.Dilba K.Nies K.van der Kolk A.G.Liem M.I.Sex differences in plaque composition and morphology among symptomatic patients with mild-to-moderate carotid artery stenosis Stroke 53220223703783498323710.1161/STROKEAHA.121.036564 PMC 8785521 · doi ↗ · pubmed ↗
- 4van den Bouwhuijsen Q.J.Vernooij M.W.Hofman A.Krestin G.P.van der Lugt A.Witteman JC.Determinants of magnetic resonance imaging detected carotid plaque components: the Rotterdam Study Eur Heart J 33220122212292182184410.1093/eurheartj/ehr 227 · doi ↗ · pubmed ↗
- 5Saba L.Nardi V.Cau R.Gupta A.Kamel H.Suri J.S.Carotid artery plaque calcifications: lessons from histopathology to diagnostic imaging Stroke 53120222902973475330110.1161/STROKEAHA.121.035692 · doi ↗ · pubmed ↗
- 6Baradaran H.Al-Dasuqi K.Knight-Greenfield A.Giambrone A.Delgado D.Ebani E.J.Association between carotid plaque features on CTA and cerebrovascular ischemia: a systematic review and meta-analysis AJNR Am J Neuroradiol 38122017232123262907463810.3174/ajnr.A 5436 PMC 7963758 · doi ↗ · pubmed ↗
- 7Truijman M.T.Kooi M.E.van Dijk A.C.de Rotte A.A.van der Kolk A.G.Liem M.I.Plaque at RISK (PARISK): prospective multicenter study to improve diagnosis of high-risk carotid plaques Int J Stroke 9620147477542413859610.1111/ijs.12167 · doi ↗ · pubmed ↗
- 8Migrino R.Q.Bowers M.Harmann L.Prost R.La Disa J.F.Jr.Carotid plaque regression following 6-month statin therapy assessed by 3T cardiovascular magnetic resonance: comparison with ultrasound intima media thickness J Cardiovasc Magn Reson 132011372181299210.1186/1532-429X-13-37PMC 3166901 · doi ↗ · pubmed ↗