Ceftazidime–Avibactam Pharmacokinetic Comparative In Vivo/In Vitro Study in a Critically Ill Children Under High‐Volume Continuous Venovenous Hemodiafiltration
Michael Thy, Alexandre Debs, Gabrielle Lui, Leo Froelicher‐Bournaud, Jean‐Marc Tréluyer, Mehdi Oualha

TL;DR
This study compares how ceftazidime–avibactam behaves in simulated dialysis and real-life cases in critically ill children.
Contribution
The study introduces a comparative in vitro/in vivo analysis of ceftazidime–avibactam under high-volume dialysis in children.
Findings
Ceftazidime and avibactam are significantly removed during high-volume CVVHDF.
Higher dosing or continuous infusion is needed for effective treatment in critically ill children on CRRT.
Abstract
Ceftazidime–avibactam is a novel cephalosporin/beta‐lactamase inhibitor combination developed to address increasing antimicrobial resistance. This report presents a comparative study of the pharmacokinetics of ceftazidime and avibactam, utilizing in vitro data derived from two experiments with continuous venovenous hemodiafiltration (CVVHDF) simulation and a comparison with a previously published in vivo case report. The results highlight the importance of therapeutic drug monitoring and the need for higher dosing or continuous infusion of ceftazidime–avibactam in critically ill children under crontinuous renal replacement therapy (CRRT).
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
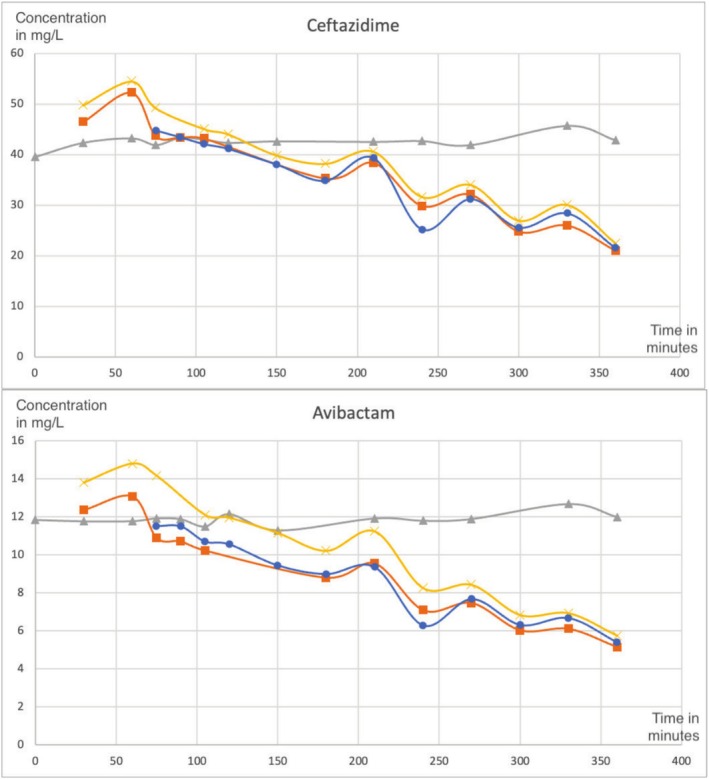 FIGURE 1
FIGURE 1| Compound name | Sample type | Median concentration (mg/L) | Interquartile range (mg/L) |
|---|---|---|---|
| Ceftazidime | T (Control) | 42.6 | 42.4–42.9 |
| E (Prefilter) | 37.2 | 31.2–41.4 | |
| S (Postfilter) | 31.8 | 27.0–39.6 | |
| F (Effluent) | 36.4 | 27.7–41.3 | |
| Avibactam | T (Control) | 11.9 | 11.8–12.0 |
| E (Prefilter) | 10.2 | 7.9–11.4 | |
| S (Postfilter) | 7.5 | 6.9–9.7 | |
| F (Effluent) | 9.2 | 6.6–10.6 |
| Parameter | In vivo (Ceftazidime) | In vitro (Ceftazidime) | In vivo (Avibactam) | In vitro (Avibactam) |
|---|---|---|---|---|
| CL (L/h) | 1.7 | 3.02 | ||
| CLCRRT (L/h) | 0.49–1.02 | 0.85 [0.82–0.86] | 0.43–0.99 | 0.80 [0.76–0.83] |
- —Baxter International Foundation10.13039/100005643
- —Société de Réanimation de Langue Française10.13039/501100008800
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntibiotic Resistance in Bacteria · Antibiotics Pharmacokinetics and Efficacy · Antibiotic Use and Resistance
Introduction
1
Ceftazidime–avibactam is a novel cephalosporin/beta‐lactamase inhibitor combination developed to address the increasing prevalence of multidrug‐resistant Gram‐negative (MDR‐GN) pathogens [1, 2]. Its use in pediatric patients was approved by the US Food and Drug Administration in 2019 for intra‐abdominal infections, and recent literature reviews have demonstrated its efficacy and safety in various MDR‐GN infections [3, 4]. The pharmacokinetics (PK) of ceftazidime–avibactam under continuous renal replacement therapy (CRRT) have been described in a few adult cases, but data in pediatric patients are limited [5]. This study aims to describe the PK of ceftazidime–avibactam with in vitro data derived from two experiments with continuous veno‐venous hemodiafiltration (CVVHDF) simulation, then compare in vitro results with a previously published in vivo case report of a critically ill pediatric patient undergoing CRRT.
Methods
2
In Vivo Study
2.1
The in vivo data were obtained from a case report of a 6‐month‐old, 8‐kg‐weighted, female with sepsis due to Stenotrophomonas maltophilia infection following stem cell transplantation [5]. The patient was treated with ceftazidime–avibactam every 8 h with a 2‐h infusion of 30–7.5 mg/kg.
Residual diuresis during CVVHDF remained stable at approximately 0.5 mL/kg/h.
CVVHDF was performed using the Prismaflex system machine (Baxter Int, SE) with an ST 60 set. Phoxilium was used as both the dialysate and replacement solution. Anticoagulation was avoided due to hemorrhagic risk and liver failure. The blood flow rate was maintained at 80 mL/min (10 mL/kg/min), with a dialysate flow rate of 300 mL/h (37.5 mL/kg/h), a replacement flow rate of 600 mL/h (75 mL/kg/h), and a net ultrafiltrate flow rate ranging from 30 to 40 mL/h (3.75–5 mL/kg/h). This resulted in a total effluent rate of 930–940 mL/h (116.2–117.5 mL/kg/h), a critical parameter impacting drug clearance.
In Vitro Study
2.2
In vitro experiments were conducted to simulate the conditions of CRRT [6]. The experiments were performed using the Prismaflex system machine (Baxter Int, SE) with an ST 60 set. Dialysate and replacement solutes were Phoxilium. No anticoagulation was administered. The weight was set to 8 kg, the blood flow rate to 80 mL/min (10 mL/kg/min for an 8 kg patient); dialysate flow rate to 300 mL/h (37.5 mL/kg/h); replacement flow rate to 600 mL/h (75 mL/kg/h) and net ultrafiltrate flow rate to 35 mL/h (4.4 mL/kg/h). The total effluent rate was 935 mL/h (117.5 mL/kg/h).
The circuit was primed with 1 L of 0.9% NaCl containing heparin to prevent clotting. Ceftazidime–avibactam was both prepared at a concentration of 50 mg/L by adding 250 mg of each antibiotic to 5 L of Phoxylium.
An adsorption and steady state phase of 60 min was conducted by running the CVVHDF system with the only antibiotic solution circulating. After this initial phase, sample collections were collected at multiple time points (0 to 360 min) to assess drug concentration decay over time from four distinct sites: prefilter (E), postfilter (S), effluent (F), and the reservoir as a control (T). Each sample underwent analysis to measure the concentrations of ceftazidime–avibactam using validated high‐performance liquid chromatography techniques, allowing for accurate monitoring of pharmacokinetic changes over time.
Results
3
In vitro data for ceftazidime and avibactam are summarized in Table 1, showing the median and interquartile ranges for the concentrations at different time points.
Blood samples were collected at various time points to evaluate the pharmacokinetics of the administered drugs during CVVHDF. Timepoint 0 represents the baseline sample taken immediately before antibiotic administration. Timepoint 30 was collected 30 min after drug administration to assess the initial concentration and potential adsorption by the CVVHDF filter. Timepoint 60 was collected at 60 min before initiation of the CRRT by CVVHDF. Timepoints 75 to 360 were obtained at regular intervals (every 15 to 30 min) to capture both the distribution and elimination phases of the drug. This sampling strategy provided comprehensive monitoring of the drug's pharmacokinetics over time (Figure 1 and Table 1). A comparison with the in vivo case report is displayed in Table 2.
Concentration dynamics of ceftazidime and avibactam over time under CVVHDF. Gray line for control sample (T), yellow line for prefilter sample (E), orange line for postfilter sample (S), blue line for effluent sample (F).
Discussion
4
The in vitro data provide valuable insights into the pharmacokinetics of ceftazidime–avibactam under CRRT conditions. The in vitro data showed a significant decrease in the concentrations of ceftazidime and avibactam over time, particularly in the prefilter and postfilter samples. This confirms that the drugs are being effectively removed by the CRRT system, which is consistent with the high clearance rates observed in the in vivo study. The effluent samples also showed a significant decrease in the concentrations of both drugs, indicating that the drugs are being eliminated through the CRRT system. The significant decrease in the concentrations of ceftazidime and avibactam over time suggests that higher dosing or continuous infusion may be necessary to maintain therapeutic levels and prevent the development of microbiological resistance. The in vitro data also highlight the importance of therapeutic drug monitoring in critically ill patients undergoing CRRT.
The in vitro clearances (CLCRRT) for both ceftazidime and avibactam were less variable than the corresponding in vivo CRRT clearances. This aligns with the hypothesis that the in vitro model corresponds to an ideal PK model due to the absence of complicating factors such as blood, albumin, and clotting, which can hinder filter efficiency in vivo.
In vivo total clearance (CL) is known to surpass CRRT clearance (CLCRRT) due to residual endogenous elimination pathways such as residual renal function. While in vitro models provide valuable experimental control and are instrumental in developing physiologically based pharmacokinetic (PBPK) models, they lack the contribution of these endogenous processes, emphasizing their limitations. Furthermore, in vitro models demonstrate lower variability compared to in vivo data, reflecting their reproducibility and precision. However, this reduced variability highlights the need to account for the more complex and variable conditions present in clinical settings when interpreting in vitro findings.
Thus, while in vitro models offer significant advantages for hypothesis testing and parameter estimation, they complement rather than replace in vivo studies, which remain essential for capturing the full spectrum of pharmacokinetic variability in patients [7].
Conclusion
5
The in vitro data provide valuable insights into the pharmacokinetics of ceftazidime–avibactam under CRRT conditions in critically ill children, highlighting the importance of therapeutic drug monitoring and the need for higher dosing or continuous infusion in this context. The study underscores the utility of in vitro experiments in predicting the clearance of drugs by CRRT.
Author Contributions
M.T. and M.O. conceived the study and the in vitro model. M.T. and A.D. collected the data. L.F.‐B. and G.L. performed the dosages. J.‐M. T. contributed to the review and edit the final manuscript. M.T. and M.O. contributed to the acquisition, analysis, and interpretation of the results. M.T. and M.O. drafted the manuscript and critically revised the manuscript.
Ethics Statement
The authors have nothing to report.
Consent
All authors critically revised the manuscript and consent for publication.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A. Lawandi , C. Yek , and S. S. Kadri , “IDSA Guidance and ESCMID Guidelines: Complementary Approaches Toward a Care Standard for MDR Gram‐Negative Infections,” Clinical Microbiology and Infection 28, no. 4 (2022): 465–469, 10.1016/j.cmi.2022.01.030.35150882 · doi ↗ · pubmed ↗
- 2M. Paul , E. Carrara , P. Retamar , et al., “European Society of Clinical Microbiology and Infectious Diseases (ESCMID) Guidelines for the Treatment of Infections Caused by Multidrug‐Resistant Gram‐Negative Bacilli (Endorsed by European Society of Intensive Care Medicine),” Clinical Microbiology and Infection 28, no. 4 (2022): 521–547, 10.1016/j.cmi.2021.11.025.34923128 · doi ↗ · pubmed ↗
- 3Zavicefta , “European Medicines Agency (EMA),” European Medicines Agency, accessed January 5, 2025, https://www.ema.europa.eu/en/medicines/human/EPAR/zavicefta.
- 4FDA , “Research C for DE and. Ceftazidime Avibactam Injection,” (2023), https://www.fda.gov/drugs/development‐resources/ceftazidime‐avibactam‐injection.
- 5C. Collignon , S. Benaboud , I. Gana , et al., “Pharmacokinetic of Ceftazidime‐Avibactam in a Critically Ill Patient Under High‐Volume Continuous Venovenous Haemodiafiltration: A First Paediatric Case Report,” British Journal of Clinical Pharmacology 90 (2024): 890–894, 10.1111/bcp.15993.38178624 · doi ↗ · pubmed ↗
- 6M. Thy , F. Kecili , S. Urien , et al., “Impact of Pediatric Continuous Renal Replacement Therapy Parameters on Meropenem, Piperacillin, and Tazobactam Pharmacokinetics: An In Vitro Model,” Expert Opinion on Drug Metabolism & Toxicology, ahead of print, December 22, 2024, 10.1080/17425255.2024.2443754.39692096 · doi ↗ · pubmed ↗
- 7M. Oualha , M. Thy , N. Bouazza , S. Benaboud , and A. Béranger , “Drug Dosing Optimization in Critically Ill Children Under Continuous Renal Replacement Therapy: From Basic Concepts to the Bedside Model Informed Precision Dosing,” Expert Opinion on Drug Metabolism & Toxicology 21 (2024): 173–190, 10.1080/17425255.2024.2422875.39470330 · doi ↗ · pubmed ↗