Bariatric Surgery and Lung Transplant Outcomes: Case Series and Insights from a Propensity-Matched Analysis at a High-Volume Transplant Center
Andrés Latorre-Rodriguez, Mark Shacker, Hesham Mohamed, Ross M. Bremner, Sumeet K. Mittal

TL;DR
This study finds that prior bariatric surgery does not worsen lung transplant outcomes, including survival and graft function.
Contribution
The study provides new evidence that bariatric surgery does not compromise lung transplant outcomes in patients with advanced respiratory disease.
Findings
Bariatric surgery recipients had similar survival rates and graft outcomes compared to matched controls.
Hospital and ICU lengths of stay were comparable between bariatric and control groups.
Rates of complications like primary graft dysfunction and rejection were similar in both groups.
Abstract
An increasing number of patients with a history of bariatric surgery and advanced respiratory disease are presenting for lung transplantation (LTx). We aimed to describe and compare LTx outcomes between recipients with prior bariatric surgery and a matched control group at a high-volume lung transplant center. After IRB approval, we identified bilateral LTx recipients with a pre-LTx history of bariatric surgery (Roux-en-Y gastric bypass [RYGB], sleeve gastrectomy [SG], or laparoscopic adjustable gastric band [LAGB]). The institutional experience is reported as a case series. Furthermore, perioperative and mid-term transplant outcomes such primary graft dysfunction (PGD), antibody-mediated rejection (AMR), acute cellular rejection (ACR), chronic lung allograft dysfunction (CLAD)-free survival, and overall survival (OS) were compared to a 1-to-2 propensity score-matched control group.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
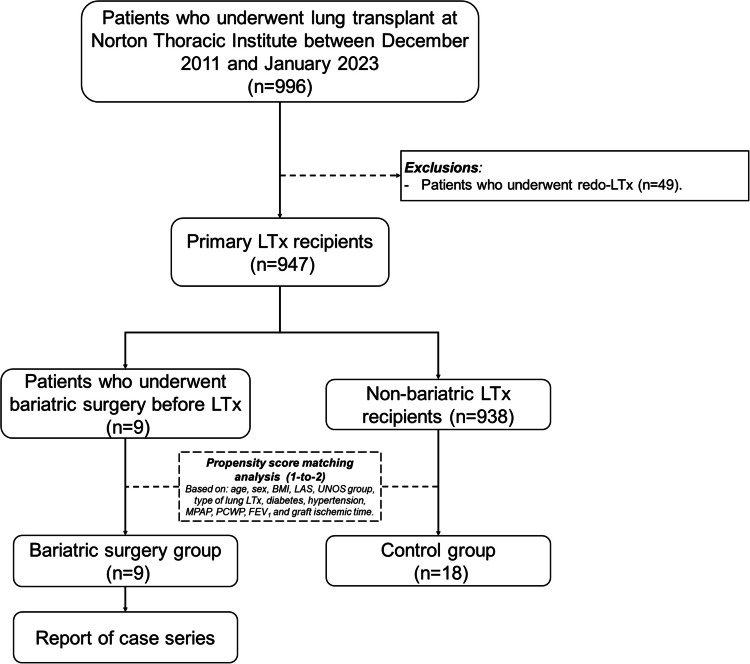 Figure 1
Figure 1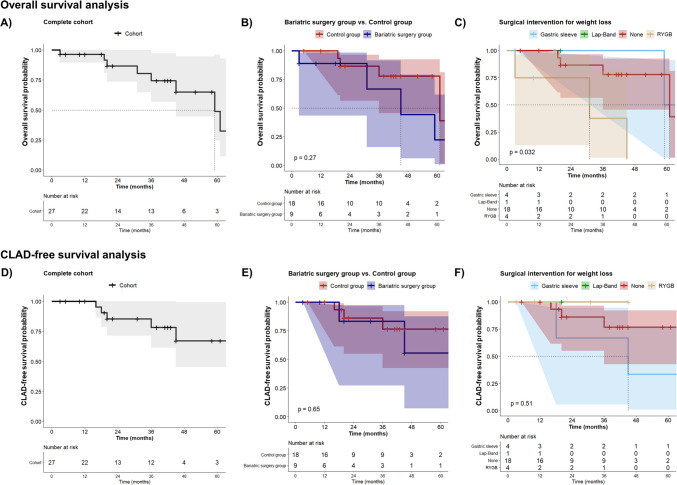 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTransplantation: Methods and Outcomes · Organ Transplantation Techniques and Outcomes · Organ and Tissue Transplantation Research
Introduction
Lung transplantation (LTx) is the only definitive treatment for end-stage lung disease [1]; however, it is complex and has a median survival of approximately 6 years, limited in most cases by chronic lung allograft rejection (CLAD) [2, 3]. Moreover, roughly 30% of patients will develop early complications such as primary graft dysfunction (PGD), antibody-mediated rejection (AMR), or acute cellular rejection (ACR) [4–6].
Due to the arduous postoperative course, careful candidate selection and candidate optimization have been proposed to ease morbidity and mortality [7, 8]. Obesity is a common medical condition among LTx candidates due to its increasing worldwide incidence, and severe obesity is usually a contraindication to LTx due to increased postoperative risks [9–12]. Therefore, an intervention that provides substantial weight reduction with a relatively uncomplicated postoperative recovery may improve LTx candidacy.
By the same token, with the growing popularity and use of surgical interventions for weight loss [13], the number of patients with prior bariatric surgery seeking LTx is expected to increase. Furthermore, bariatric surgery patients (particularly after sleeve gastrectomy [SG]) have a higher incidence of gastroesophageal reflux disease (GERD) and esophageal dysmotility, which are both associated with worse outcomes after LTx [14–16]. However, data on outcomes among LTx recipients with a history of bariatric surgery are limited. Therefore, we present a case series and compare early and mid-term LTx outcomes between recipients who had undergone pre-LTx bariatric surgery for weight loss and a matched control group.
Methods
Study Design and Setting
We present a case series of bilateral LTx recipients with a history of bariatric surgery before their LTx evaluation at a high-volume lung transplant center. In addition, we retrospectively compared the postoperative course and mid-term outcomes of these patients to a propensity score-matched control group. Patient demographics, history of bariatric surgery, listing conditions, and perioperative and postoperative course were retrospectively obtained through chart review or from prospectively maintained institutional databases. This research was approved by our institutional review board (PHXU-21–500-136–73-18; February 24, 2023) with waiver of written patient consent due to the study design. The STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) statement and checklist were followed (Supplementary material S1).
Sampling and Study Population
All adult patients (> 18 years) with history of bariatric surgery for weight loss (i.e., Roux-en-Y gastric bypass [RYGB], sleeve gastrectomy [SG], or laparoscopic adjustable gastric band [LAGB]) before LTx were identified using an institutional transplant listing repository; thus, sampling was completed by convenience. Patients were included in the study (i.e., bariatric surgery group) if they underwent bilateral LTx between December 2011 and January 2023 at our institution. Patients who underwent redo-LTx procedures were excluded. A 1-to-2 propensity score-matched control group was created from all transplanted patients during the same period considering 12 parameters: age, sex, body mass index (BMI), lung allocation score (LAS), United Network for Organ Sharing (UNOS) group, type of transplant, diabetes, hypertension, mean pulmonary artery pressure (MPAP), pulmonary capillary wedge pressure (PCWP), forced expiratory volume in one second (FEV1) at listing, and graft ischemic time. Figure 1 presents the study flow diagram.Fig. 1. Study flow diagram. Abbreviations: BMI Body mass index, FEV_1_ forced expiratory volume in one second, LAS lung allocation score, LTx lung transplantation, MPAP Mean pulmonary artery pressure, PCWP Pulmonary capillary wedge pressure, UNOS: United Network for Organ Sharing
Outcomes and Definitions
Hospital length of stay (LOS), intensive care unit length of stay (ICU-LOS), incidence of PGD, AMR, and ACR within one year of LTx, CLAD-free survival, and overall survival (OS) were compared between the bariatric surgery and the matched control group. Standard definitions and diagnostic criteria were adopted from The International Society for Heart and Lung Transplantation guidelines [17–20].
Patient Care, Testing, and Surveillance
Pulmonary Functional and Histological Testing
As standard practice, we obtain multiple pulmonary function tests (PFTs) before and after LTx using spirometry. After LTx, PFTs are conducted every 2–3 weeks during the first 6 months, then every month until year 2, and thereafter every 3–6 months. Moreover, all recipients undergo surveillance bronchoscopy (i.e., bronchoalveolar lavage and transbronchial biopsy) at 1, 3, 6, 9, and 12 months after LTx, and thereafter every 6 months. Additional tests are obtained as indicated.
Esophageal Functional Testing
Pre-LTx (i.e., during listing workup) and post-LTx (i.e., usually within 3–6 months after LTx) ambulatory esophageal 24-h pH monitoring, high-resolution manometry, and barium esophagram are completed following standard protocols and analyzed by an experienced foregut or thoracic surgeon.
Postoperative Patient Care
Most LTx recipients receive a similar immunosuppressive regimen for induction with IV methylprednisolone and basiliximab before perfusion of the lung allografts. A small subset of patients receives rituximab in combination with IV immunoglobulin. Immunosuppression in all cases is maintained with triple-drug therapy (steroids, mycophenolate mofetil, and tacrolimus).
Sampling and Statistical Analysis
A maximum available sample size was achieved by convenience. Descriptive statistics were applied, reporting continuous variables as median (IQR) and categorical variables as count and proportion. Clinical characteristics and LTx outcomes of the bariatric patients were tabulated and presented as a case series. A propensity-matched control group was created using logistic regression and nearest neighbor without replacement. Balance was determined with an absolute standardized difference < 0.2. Differences in pre-specified outcomes were assessed using Fisher’s exact and Mann–Whitney U tests. Overall and CLAD-free survival were calculated via Kaplan–Meier curves and assessed with the log-rank test. Missing data were handled with pairwise deletion (available-case analysis), and p-values were adjusted by Bonferroni correction. Statistical significance was set a p < 0.05. All analyses were conducted using SPSS version 29.0 (IBM SPSS Statistics; Armonk, NY, USA) and R version 4.3.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Demographic and Clinical Characteristics
A total of 996 LTx procedures were performed between December 2011 and January 2023; of these, 49 redo procedures were excluded. Nine patients with a history of bariatric surgery for weight loss before LTx were identified (7 [77.8%] women; median age at LTx, 65 [IQR 57–69] years). All bariatric procedures (RYGB, n = 4; SG, n = 4, LAGB, n = 1) were performed at other institutions. The median time from bariatric surgery to LTx was 76 (IQR 48–93) months. All but one patient was listed for LTx for restrictive lung disease (i.e., UNOS group D). Table 1 summarizes clinical characteristics and outcomes within the bariatric group (i.e., case series). Table 1. Detailed clinical characteristics and outcomes of individuals in the bariatric groupPre-LTx characteristicsPost-LTx characteristicsAge, SexSurgery TypeSurgery to LTx, moDiagnosisUNOS GroupLASBMI kg/m^2^CCIHRMDMSHRMDMSICU LOS, daysLOS, daysPGDWorst PGD gradeAMRACRWorst ACR gradeCLADFU time, moBMI at last FU kg/m^2^Status****Cause of death66, FRYGB169UIP/IFPD40.6227.45Inconclusive IEM3.1Normal2.31222NoG0NoYesA1No3121.9DeceasedSepsis40, FRYGB76COVID-FibrosisD62.1927.01--Normal0.7732YesG3NoNoA0No1030.1Alive-77, FRYGB63ILD/HPD43.4530.95Inconclusive IEM25.9Normal1.21750YesG3NoNoA0No4523.3DeceasedUnknown69, FRYGB151COPDA37.1019.94DES10.7--1340YesG1NoNoA0No318.8DeceasedType A aortic aneurysm57, FSG93UIP/IFPD37.8028.92Inconclusive EGJOO23.2Inconclusive EGJOO1141NoG0NoNoA0No13515.5Alive-64, FSG48NSIP/UIPD42.4230.14Normal24.5Normal25.3922YesG2NoYesA2No326.2Alive-55, FSG43NSIP/UIPD37.8032.52Inconclusive IEM15.9Inconclusive IEM30.9731YesG3YesYesA2Yes1839.1Alive-73, MLB12NSIP/UIPD46.5022.74Inconclusive EGJOO0.6--840YesG2NoYesA1No2029.1Alive-65, MSG76UIP/IFPD85.0326.74--Inconclusive IEM88.61535YesG3NoNoA0Yes5928.3DeceasedRespiratory failureAbbreviations: ACR, acute cellular rejection; AMR, antibody mediated rejection; BMI, body mass index; CCI, Charlson comorbidity index; CLAD, chronic lung allograft dysfunction; COPD, chronic obstructive pulmonary disease; DES, distal esophageal spasm; DMS, DeMeester score; EGJOO, esophagogastric outflow obstruction; F, female; FU, follow-up; HRM, high-resolution manometry; HP, hypersensitivity pneumonitis; ICU, intensive care unit; IEM, ineffective esophageal motility; IFP, idiopathic pulmonary fibrosis; ILD, interstitial lung disease; LAS, lung allocation score; LB, LapBand; LOS, length of stay; M, male; NSIP, nonspecific interstitial pneumonia; LTx, lung transplantation; PGD, primary graft dysfunction; RYGB, Roux-en-Y gastric bypass; SG, sleeve gastrectomy; UIP, usual interstitial pneumonia; UNOS, United Network for Organ Sharing
The control group was developed from the remaining 938 primary LTx recipients during the same period. After propensity-matching, 18 patients formed this group. The median age at LTx was 67.5 (IQR 59.5–70.8) years, 17 (94.4%) were female, and most had a restrictive lung disease (88.9%). The age, pre-LTx BMI, history of diabetes and hypertension, UNOS group, LAS, and type of LTx were adequately balanced and remarkably similar between groups. Similarly, although not reaching Cohen’s d cutoff for a small effect size, the remaining baseline characteristics (sex, history of smoking, MPAP, PCWP, FEV1, and graft ischemia time) were also comparable (Supplementary material S2).
Pulmonary and Esophageal Function
The DeMeester score (DMS), total acid exposure time (AET), and the proportion of patients with impaired esophageal body peristalsis were similar between the groups before and after LTx (Supplementary material S3). However, within the bariatric surgery group after LTx, patients in the SG subgroup had a higher median DMS and AET than those in the RYGB subgroup (30.9 vs. 1.2 and 9.8% vs. 0.1%, respectively), suggesting that the SG subgroup was more prone to pathological reflux and its related complications (Supplementary material S4).
Bariatric patients and controls demonstrated similar pulmonary function before LTx, and most patients improved after LTx. Regardless of the group, pulmonary function was stable among patients who reached 1-, 2-, and 3-year post-LTx follow-ups; nevertheless, a slight trend toward functional decline was noted thereafter (i.e., 5-year follow-up) among the survivors (Supplementary material S4).
Hospital and ICU Length of Stay
Both the hospital-LOS and ICU-LOS after LTx were slightly longer in the bariatric surgery group than the control group, but this difference was not statistically significant (median LOS: 35 (IQR 31–40) vs. 24 (IQR 17–30) days; median ICU-LOS: 11 (IQR 8–13) vs. 9 (IQR 5–11) days (Table 2)). Moreover, the RYGB and SG subgroups had a median LOS of 36 (IQR 27–45) and 33 (IQR 26.5–38) days, respectively, and a median ICU-LOS of 12.5 (IQR 9.5–15) and 10 (IQR 8–13) days, respectively (Supplementary material S4). Table 2. Perioperative and lung transplant outcomes among lung transplant recipients with history of bariatric surgery and a control groupBariatric surgery group (n = 9)****Control group (n = 18)p-valuePerioperative outcomesLength of ICU stay, days11 [8, 13]9 [5, 11]0.11Hospital length of stay, days35 [31, 40]24 [17, 30]0.19Post-LTx outcomesAny grade of PGD within 72 h after LTx7 (77.8)10 (55.6)0.42PGD grade 3 within 72 h after LTx4 (44.4)6 (33.3)0.68AMR within 1 year after LTx1 (11.1)4 (22.2)0.57Any grade of ACR within 1 year after LTx4 (44.4)3 (16.7)0.12Highest grade of ACR documented*No evidence of ACR (grade A0)5 (55.6)16 (88.8)0.22Mild ACR (grade A1)*2 (22.2)1 (5.6)*Moderate ACR (grade A2)*2 (22.2)1 (5.6)*Severe ACR (grade A3)*0 (0)0 (0)Evidence of CLAD at any time after LTx2 (22.2)3 (16.7)0.73All values are presented as counts and proportions or medians and interquartile rangesAbbreviations: ACR, acute cellular rejection; AMR, antibody mediated rejection; CLAD, chronic lung allograft dysfunction; ICU, intensive care unit; LOS, length of stay; LTx, lung transplantation; PGD, primary graft dysfunction
Incidence of PGD, AMR, and ACR
There was a slightly higher (not statistically significant) incidence of any grade of PGD within the first 72 h after LTx among the bariatric group compared to controls (77.8% vs. 55.6%, p = 0.42) (Table 2). The incidence of severe PGD (i.e., grade 3) and AMR were similar between the groups (PGD: 44.4% vs. 33.3%, p = 0.68; AMR: 11.1% vs. 22.2%, p = 0.57). The incidence of ACR among the bariatric group and controls was 44.4% and 16.7%, respectively (p = 0.12), but all cases of ACR were minimal (A1) or mild (A2) (Tables 1 and 2).
Survival Analysis
Four (44.4%) patients with history of bariatric surgery and 4 (22.2%) in the control group died during the observation period. The median overall survival of the entire cohort was 59 months (Fig. 2A), whereas the median survival for the bariatric surgery and control groups was 45 months and 61 months, respectively. The cumulative survival in the bariatric group at 1, 2, and 3 years was 88.9%, 88.9%, and 66.7% compared to 100%, 86.7%, and 78% in the control group (log-rank test, p = 0.27, Fig. 2B). The causes of death within the RYGB subgroup (n = 3) were immunosuppression-related sepsis (n = 1), acute type A aortic aneurysm dissection (n = 1), and unknown (n = 1), and the cause of death in the SG patient was CLAD. Deaths in the control group were COVID-19 sequelae (n = 2) and CLAD-related respiratory failure (n = 2). Notably, patients in the RYGB subgroup had lower overall survival than those in the SG subgroup (Fig. 2C). Five (18.5%) patients were diagnosed with CLAD during the study period (Fig. 2D). CLAD-free survival appeared to be similar between the bariatric surgery group and controls (Fig. 2E) but slightly worse among the SG subgroup (Fig. 2F).Fig. 2. Kaplan–Meier curves. A Overall survival for the entire cohort, B stratified overall survival for bariatric surgery and control groups, C stratified overall survival according to the type of bariatric intervention, D CLAD-free survival for the entire cohort, E stratified CLAD-free survival for bariatric surgery and control groups, F stratified CLAD-free survival according to the type of bariatric intervention. Of note, subgroup survival analyses and plots (i.e., between type of interventions) are recommended to be taken as descriptive observations rather than inferential analyses. Abbreviations: CLAD: chronic lung allograft dysfunction; RYGB: Roux-en-Y gastric bypass
Discussion
Bariatric surgery for the treatment of severe obesity is rapidly increasing; Approximately 280,000 procedures were performed in the United States in 2022, a 6.5% increase from 2021 [13]. Likewise, lung transplants rose by 6.8% over the same period, from 2,569 to 2,743 [21]. Thus, it is becoming more common for lung transplant centers to evaluate patients with a history of bariatric surgery. This intersection requires particular attention, as bariatric surgery may contribute to the development of GERD and/or esophageal dysmotility—both recognized risk factors for ACR and CLAD.
Although the effects of bariatric surgery on LTx outcomes are largely unknown, there are multiple mechanisms by which bariatric surgery may improve patient candidacy for LTx and lead to outcomes similar to those of non-obese LTx recipients. Bariatric surgery may facilitate the resolution of obesity-associated structural changes in the thoracoabdominal region and decrease the systemic pro-inflammatory signaling status [22]. After bariatric surgery, an overall increase in pulmonary functional capacity (especially in patients with interstitial lung disease) is expected due to an improvement in diaphragmatic and thoracic cage mobility [22–24]. Such changes may also delay the need for lung transplant listing. Furthermore, weight loss can reduce the overproduction of obesity-related cytokines that can induce a continuous pro-inflammatory state and predispose patients to develop bronchial hyperresponsiveness [25].
By 2020, only three centers had reported their experience [22, 26, 27], including 28 patients with end-stage respiratory disorders (mostly interstitial lung disease [n = 26, 92.8%]) who were not considered candidates for LTx due to obesity [24]. Of these patients, after bariatric surgery (RYGB = 18, SG = 9, LAGB = 1), eight (28.6%) were listed for LTx and two (7%) underwent LTx. One of these recipients had reached a survival of 88 months without complications [22]. Moreover, four (14.3%) patients improved clinically, precluding the need for listing. These data support the safety of bariatric surgery even in patients with severe associated medical problems as well as the important role of surgical weight loss management to achieve LTx listing and eventually undergo LTx; however, they do not directly address LTx outcomes in patients with a history of bariatric surgery.
Our experience including nine LTx recipients with a history of pre-LTx bariatric surgery may provide significant and novel insights. Overall, compared to a matched control group, these patients did not perform significantly worse after LTx. This suggests that a history of bariatric surgery should not be a contraindication to LTx. Nevertheless, there is a need for further clarification of potential post-LTx risks derived from prior bariatric procedures. Despite the limited small sample size, we observed that patients in the RYGB subgroup had worse overall survival than those in the SG subgroup, but paradoxically a trend toward increased rates of ACR, CLAD, and worse CLAD-free survival was seen among the SG subgroup.
The shorter median overall survival in the RYGB subgroup may be attributed to early, non-LTx-related deaths (e.g., type A aneurysm dissection) or deaths unrelated to graft dysfunction (e.g., sepsis-induced multiorgan failure). Additionally, anatomical changes from RYGB could impact medication pharmacokinetics and absorption (including that of immunosuppression therapy), which warrants tailored strategies—such as serum monitoring of medication levels—to ensure therapeutic efficacy and reduce risks of toxicity or undertreatment [28]. Meanwhile, in patients with a history of SG, the higher risk of GERD-related aspiration and subsequent allograft injury may explain the trend toward an increased CLAD incidence and worse CLAD-free survival in this group. For these patients, regular functional esophageal and respiratory surveillance may be advised to detect complications early. Furthermore, early surgical management of GERD after LTx (i.e., before 180 days) has been proven to be safe and is a critical step to improve patient outcomes [29]. Another important aspect of bariatric surgery to consider is the narrow and altered anatomy of the SG, which makes postoperative nutrition management more difficult (i.e., J or G tube placement) than that after RYGB. Thus, the potential complexity of postoperative enteral access for SG patients theoretically places them in a different risk category. Finally, patients who have undergone RYGB may have an increased risk of developing a marginal ulcer due to chronic steroid use after LTx [30].
Our study has several limitations including a single-center design with a small, heterogeneous sample (i.e., multiple bariatric surgery techniques), limiting further statistical analyses (e.g., competing events in survival analysis) and generalizability. Given a small sample size and reduced statistical power (~ 20.5% based on a post hoc calculation for overall survival), the p-values were reported only for pre-specified outcomes to minimize spurious findings. However, this is the largest report to date, and we propose using these results to guide future larger studies. Furthermore, as the bariatric procedures were performed at different institutions, we were not able to retrieve specific anthropometric or operative data. Moreover, the median time from bariatric surgery to lung transplantation varied among included patients, which may have influenced both weight loss maintenance and graft outcomes. Lastly, the LTx procedures were performed in a wide observation period (i.e., 2011–2023), which makes the postoperative course of each patient unique and susceptible to variations in standard practices.
Conclusion
The postoperative course—measured by hospital-LOS and ICU-LOS as well as the incidence of PGD, AMR, ACR, and CLAD—appear to be similar between LTx recipients with a history of bariatric surgery for weight loss and matched controls. Therefore, a history of bariatric surgery should not preclude LTx. However, some trends indicating variations in post-LTx outcomes based on the type of bariatric intervention were observed. Thus, we recommend a multidisciplinary approach both pre- and post-LTx for these patients, involving specialists in bariatric surgery, thoracic surgery, pulmonology, nutrition, and pharmacy to address specific concerns that may arise (i.e., weight control, nutrition and medication absorption, GERD and aspiration, and enteral complications such as delayed gastric emptying). Further research involving larger sample sizes is needed.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary file1 (PDF 455 KB)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Guimarães C, Martins MV, Moutinho Dos Santos J. Pulmonary function tests in obese people candidate to bariatric surgery. Rev Port Pneumol 2012;18(3):115–119. 10.1016/j.rppneu.2012.01.00510.1016/j.rppneu.2012.01.00522402178 · doi ↗ · pubmed ↗
- 2Takata MC, Campos GM, Ciovica R et al. Laparoscopic bariatric surgery improves candidacy in morbidly obese patients awaiting transplantation. Surg Obes Relat Dis 2008;4(2):159–164; discussion 164–155. 10.1016/j.soard.2007.12.00910.1016/j.soard.2007.12.00918294923 · doi ↗ · pubmed ↗
- 3Razia D, Mittal SK, Fournier S et al. Antireflux surgery versus medical management of gastro-oesophageal reflux after lung transplantation. Eur J Cardiothorac Surg 2023;63(3). 10.1093/ejcts/ezad 06310.1093/ejcts/ezad 06336806922 · doi ↗ · pubmed ↗