Sustained acoustic medicine increases local circulation with a diclofenac delivery patch: a randomized placebo controlled study
Anthony Scanzuso, Tabitha Hendren, Mia Egmont, Julia Zarkar, Michael Roberge

TL;DR
A wearable ultrasound device called SAM boosts local blood flow and temperature, and combining it with a diclofenac patch doesn't reduce its effectiveness.
Contribution
This study demonstrates that SAM's diathermic effects are sustained and not hindered by diclofenac gel, while enhancing drug delivery through sonophoresis.
Findings
SAM increased blood flow by 19.2 PU and temperature by 2.4°C compared to placebo.
Diclofenac gel did not affect SAM's biological effects on circulation or temperature.
SAM's effects on blood flow and temperature were sustained for 60 minutes.
Abstract
Sustained Acoustic Medicine (SAM) is a non-invasive long-term wearable device that delivers localized long duration high-frequency continuous ultrasound. SAM's biomechanical and diathermic stimuli enhance local circulation and oxygenation, accelerate tissue healing, and alleviate pain. The sonophoresis effects of SAM further improve transdermal drug delivery. Diclofenac is a topical Nonsteroidal anti-inflammatory drug for treating localized musculoskeletal (MSK) pain. Its efficacy is significantly dependent on skin porosity. This study aims to determine the diathermic effects of SAM and diclofenac on localized blood circulation. Sixty-four healthy participants were randomly assigned to four groups (Active SAM group: n = 32, Placebo SAM group: n = 32): (A) Coupling gel + placebo SAM), (B) Coupling gel + active SAM, (C) 2.5% Diclofenac gel + placebo SAM, and (D) 2.5% Diclofenac gel +…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
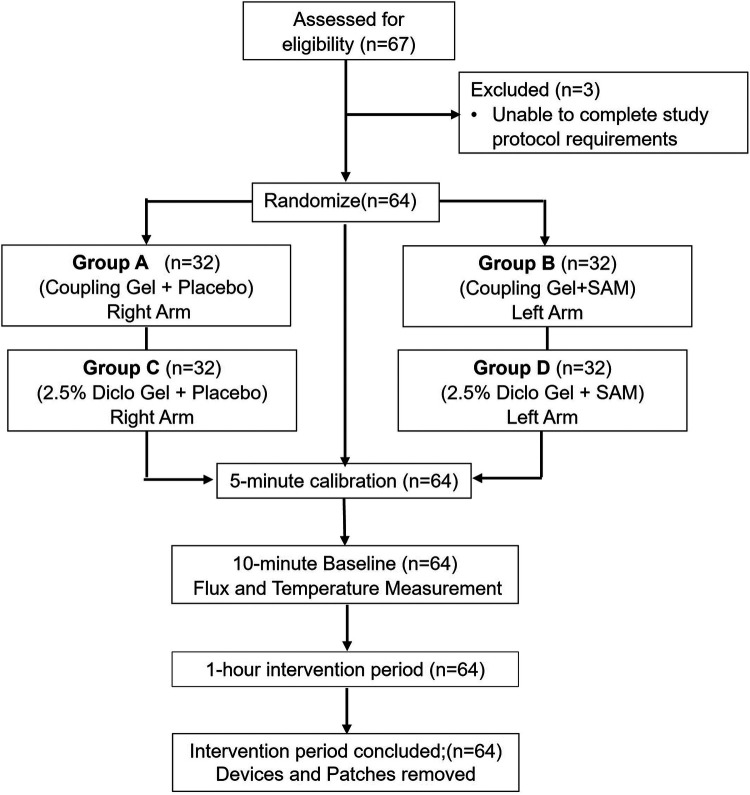 Figure 1
Figure 1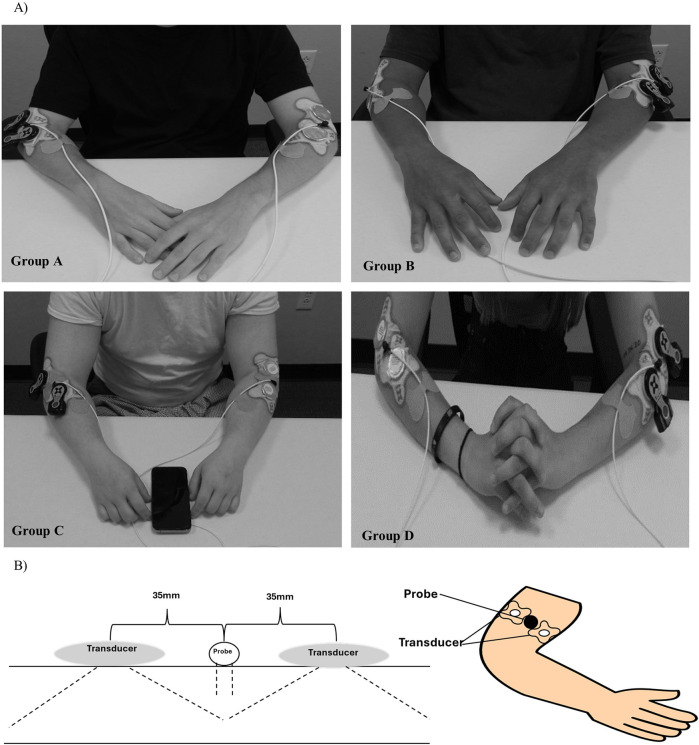 Figure 2
Figure 2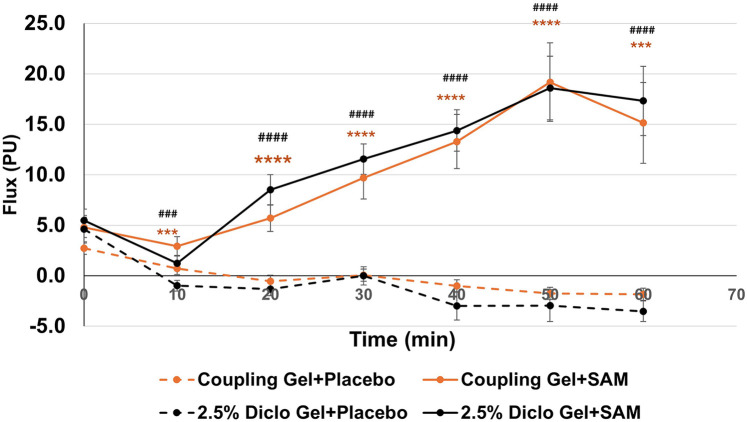 Figure 3
Figure 3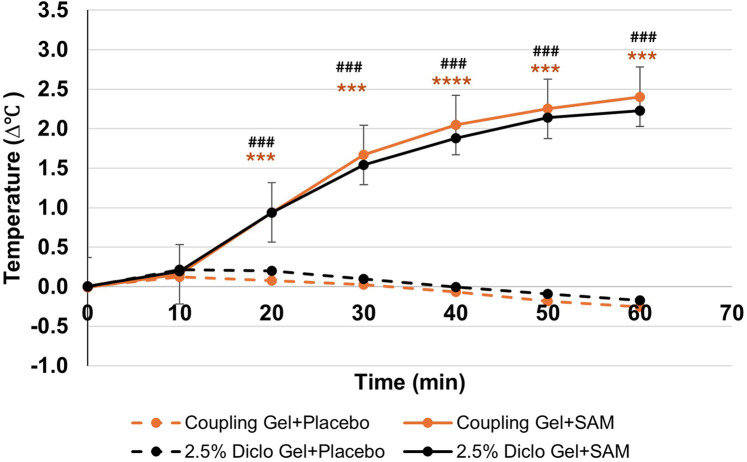 Figure 4
Figure 4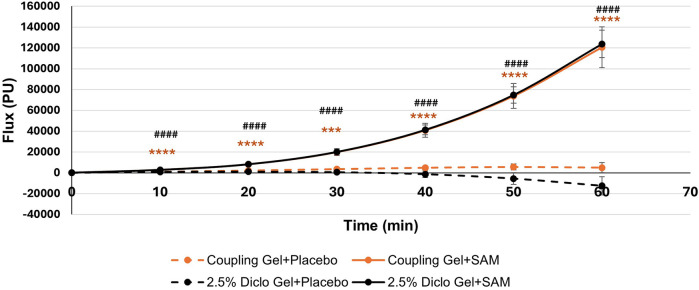 Figure 5
Figure 5| Variable | Group A (coupling Gel + Placebo) | Group B (coupling Gel + SAM) | Group C (2.5% Diclo Gel + Placebo) | Group D (2.5% Diclo Gel + SAM) | |
|---|---|---|---|---|---|
|
| 32 Right Arms | 32 Left Arms | 32 Right Arms | 32 Left Arms | 1 |
| Sex (M/F) | 18/14 | 18/14 | 18/14 | 18/14 | 1 |
| Age, years | 23.8 ± 8.4 | 23.8 ± 8.4 | 25.9 ± 9.8 | 25.9 ± 9.8 | 0.9043 |
| BMI | 23.0 ± 3.4 | 23.0 ± 3.4 | 23.3 ± 2.8 | 23.3 ± 2.8 | 0.7013 |
| Pulse | 74.5 ± 12.4 | 74.5 ± 12.4 | 76.2 ± 12.9 | 76.2 ± 12.9 | 0.5929 |
| Time (Min) | Coupling Gel + Placebo (PU) | Coupling Gel + SAM (PU) | Mean Diff, 95% confidence interval & | 2.5% Diclo Gel + Placebo (PU) | 2.5% Diclo Gel + SAM (PU) | Mean Diff, 95% confidence interval & |
|---|---|---|---|---|---|---|
| 0 | 2.7 ± 9.3 | 4.8 ± 5.7 | 2.06 (−1.34 to 5.47, | 4.6 ± 7.6 | 5.5 ± 6.3 | 0.86 (−1.62 to 3.34, |
| 10 | 0.7 ± 3.3 | 2.9 ± 5.2 | 2.21 (0.80 to 3.36, | −1.0 ± 2.9 | 1.2 ± 4.0 | 2.23 (0.78 to 3.68, |
| 20 | −0.5 ± 3.6 | 5.7 ± 7.3 | 6.25 (3.54 to 8.95, | −1.3 ± 3.6 | 8.5 ± 8.5 | 9.84 (6.71 to 12.97, |
| 30 | 0.0 ± 3.3 | 9.7 ± 11.8 | 9.65 (5.12 to 14.19, | 0.0 ± 5.0 | 11.5 ± 8.6 | 11.55 (8.48 to 14.63, |
| 40 | −1.0 ± 4.1 | 13.3 ± 15.2 | 14.30 (8.62 to 20.00, | −3.0 ± 7.8 | 14.4 ± 11.6 | 17.35 (12.40 to 22.30, |
| 50 | −1.8 ± 5.8 | 19.2 ± 22.0 | 20.93 (12.89 to 28.97, | −3.0 ± 8.8 | 18.6 ± 17.8 | 21.56 (15.92 to 27.21, |
| 60 | −1.8 ± 4.4 | 15.1 ± 22.6 | 17.39 (9.08 to 25.70, | −3.5 ± 5.7 | 17.3 ± 19.3 | 20.83 (14.65 to 27.03, |
| Time | Coupling Gel + Placebo (ΔT°C) | Coupling Gel + SAM (ΔT°C) | Mean Diff, 95% confidence interval & | 2.5% Diclo Gel + Placebo (ΔT°C) | 2.5% Diclo Gel + SAM (ΔT°C) | Mean Diff, 95% confidence interval & |
|---|---|---|---|---|---|---|
| 0 | 0.0 ± 1.1 | 0.0 ± 1.1 | 0.00 (−0.19 to 0.19, | 0.0 ± 1.1 | 0.0 ± 1.1 | 0.00 (−0.22 to 0.22, |
| 10 | 0.1 ± 1.1 | 0.2 ± 1.1 | 0.04 (−0.15 to 0.23, | 0.2 ± 1.1 | 0.2 ± 1.1 | 0.025 (−0.23 to 0.19, |
| 20 | 0.1 ± 1.1 | 0.9 ± 1.1 | 0.87 (0.65 to 1.08, | 0.2 ± 1.1 | 0.9 ± 1.1 | 0.74 (0.50 to 0.99, |
| 30 | 0.0 ± 1.1 | 1.7 ± 1.1 | 1.65 (1.41 to 1.90, | 0.1 ± 1.1 | 1.5 ± 0.9 | 1.44 (1.16 to 1.72, |
| 40 | −0.1 ± 1.1 | 2.0 ± 1.1 | 2.12 (1.85 to 2.40, | 0.0 ± 1.1 | 1.9 ± 0.8 | 1.88 (1.56 to 2.20, |
| 50 | −0.2 ± 1.1 | 2.3 ± 1.2 | 2.44 (2.14 to 2.75, | −0.1 ± 1.1 | 2.1 ± 0.8 | 2.23 (1.90 to 2.56, |
| 60 | −0.3 ± 1.0 | 2.4 ± 1.2 | 2.67 (2.35 to 2.99, | −0.2 ± 1.1 | 2.2 ± 0.7 | 2.40 (2.04 to 2.75, |
| Time | Coupling Gel + Placebo (PU) | Coupling Gel + SAM (PU) | Mean Diff, 95% confidence interval & | 2.5% Diclo Gel + Placebo (PU) | 2.5% Diclo Gel + SAM (PU) | Mean Diff, 95% confidence interval & |
|---|---|---|---|---|---|---|
| 0 | 51.4 ± 168.0 | 87.6 ± 102.7 | 36.23 (−26.17 to 98 63, | 85.5 ± 140.28 | 101.5 ± 101.46 | 16.01 (−28.71 to 60.73, |
| 10 | 994.15 ± 1306 | 2846.69 ± 3127.13 | 1852.54 (778.95 to 2926.14, | 931.00 ± 1776.09 | 2835.35 ± 2768.82 | 1904.35 (929.72 to 2878.99, |
| 20 | 2135.71 ± 3096.1 | 8154.83 ± 8761.21 | 6019.12 (3174.04 to 8864.21, | 1124.94 ± 4379.91 | 8206.36 ± 7399.18 | 7081.42 (4339.99 to 9822.85, |
| 30 | 3476.30 ± 5670.79 | 19848.22.4 ± 18494.87 | 16371.92 (10162.70 to 22581.13, | 613.17 ± 9190.54 | 20052.13 ± 14851.21 | 19435.97 (13728.04 to 25149.90, |
| 40 | 4827.39.1 ± 9660.10 | 40843.74 ± 37220.53 | 36016.36 (22934.25 to 49098.47, | −1315.09 ± 17782.85 | 41260.60 ± 26645.49 | 42575.69 (32308.04 to 52843.34, |
| 50 | 5556.94 ± 16547.34 | 73779.55 ± 67517.43 | 68222.60 (43902.82 to 92542.38, | −5527.47 ± 31302.01 | 74787.98 ± 44869.12 | 80315.44 (63313.45 to 97317.44, |
| 60 | 4956.00 ± 26897.20 | 120658.43 ± 110944.52 | 115702.44 (75111.73 to 156293.15, | −12525.19 ± 49310.20 | 123733.24 ± 74816.34 | 136258.43 (108867.65 to 163649.21, |
- —National Institutes of Minority Health and Health Disparities
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPhonocardiography and Auscultation Techniques · Anesthesia and Pain Management · Vagus Nerve Stimulation Research
Introduction
Musculoskeletal (MSK) disorders, which affect approximately 1.71 billion people globally, are a leading cause of disability and economic burden, with their prevalence steadily increasing due to the aging population. These conditions account for an estimated 0.2% of the global gross domestic product (GDP) (1, 2). In the U.S. alone, the annual cost of treating MSK disorders exceeds $125 billion (3). Beyond the economic impact, MSK disorders are linked to cardiovascular diseases, chronic depression, insomnia, and a diminished quality of life.
Blood circulation plays an essential role in treating MSK disorders. Enhanced blood flow (hyperemia) improves tissue oxygenation, metabolic activity, and the clearance of damaged tissue (4). Studies have shown that increased tissue temperature correlates with localized hyperemia (5–7) Low-intensity ultrasound (US) generates acoustic mechanical waves, inducing mechanical and thermal forces that travel through a medium. The propagation of acoustic waves through biological tissue induces tissue, cellular, molecular, and genetic responses. The biomechanical forces induce the alignment of the extracellular matrix, activating transmembrane integrin, ion channels, receptors, and downstream pathways (6, 8). US has been shown to enhance endothelial nitric oxide (eNOS) synthase activity, increasing localized production of nitric oxide, which is known to increase blood flow, smooth muscle relaxation, and vasodilation (9, 10). US increases localized muscle temperature, leading to increase blow flow Long-duration continuous ultrasound serves as an effective modality to stimulate localized mechanical and thermal effects, promoting vasodilation, cellular proliferation, inflammation resolution, tissue regeneration, and pain relief (11–16).
Sustained Acoustic Medicine (SAM) is an FDA-approved, noninvasive, wearable medical device delivering localized ultrasound therapy. SAM operates at 3 MHz and 132 mW/cm^2^, providing 18,700 joules of energy over a four-hour treatment duration (17, 18). The therapy induces vigorous diathermic effects (>4°C over local temperature), increasing localized tissue temperature, accelerating healing, and alleviating MSK pain (7, 19–23). SAM's acoustic ultrasound waves generate biomechanical forces, compression and rarefaction, which form localized cavitation bubbles in the skin and enhance its permeability (24). This diametric effect loosens the extracellular matrix, further improving transdermal drug delivery (25, 26).
Diclofenac sodium, a cyclooxygenase (COX1 and COX2) inhibitor, is a widely used non-steroidal anti-inflammatory drug (NSAID) for treating chronic inflammatory and degenerative MSK conditions (27–29). The inhibition of COX1 suppresses the expression of prostaglandin E2, a key modulator of inflammation and pain. COX2 upregulates inflammation and tissue degradation by activating inflammatory pathways (27, 30, 31). Additionally, diclofenac modulates cytokine expression, decreasing levels of pro-inflammatory mediators such as tumor necrosis factor-alpha (TNF-α) and interleukin-1β (IL-1β), further contributing to its analgesic and anti-inflammatory properties (27, 29, 32). However, oral diclofenac often results in systemic side effects, including gastrointestinal, cardiovascular, and neurological complications (29). Topical formulations of diclofenac are safer with limited efficacy due to poor skin permeability (33). This single-blind, placebo-controlled study aims to evaluate the impact of SAM-induced hyperemia and diathermic effects on the transdermal delivery of 2.5% diclofenac ultrasound gel compared to standard ultrasound gel.
Materials and methods
Participants
Sixty-seven (n = 67) healthy adults (male and female) between the ages of 18 to 50 were screened by a board-certified medical officer. Individuals were excluded if they did not meet age criteria, were pregnant or nursing, had a history of hypertension or cardiovascular disorders, had recently had coronary artery bypass graft surgery (within the past six months), had known allergic reactions to diclofenac or other NSAIDs, or had prior treatment for MSK disorders. Following this screening process, 64 participants were enrolled in the study.
Participants were recruited through flyers, social media, word of mouth, and collaborations with local physician practices. All volunteers underwent physical examinations, reviewed the Case Report Form (CRF), and informed consent with the research assistant and medical director for eligibility confirmation before enrollment.
Study design
A voluntary, randomized, single-site, placebo-controlled study was conducted at ZetrOZ Systems (Trumbull, CT). Participants were randomized with a random number generator. The study was registered on ClinicalTrials.gov (Identifier: NCT06510062) and received approval from the Advarra Institutional Review Board (IRB) (Protocol ID: Pro00080714). All the participants signed a written informed consent form, and the study adhered to Good Clinical Practice (GCP) guidelines. Sixty-four (n = 64) healthy participants, male and female, (Table 1) were randomly assigned to four groups (n = 32): A) Coupling gel + placebo SAM), B) Coupling gel + active SAM, C) 2.5% Diclofenac gel + placebo SAM, and D) 2.5% Diclofenac gel + active SAM (Figure 1). All the female participants were not post-menopausal. For groups A and C, placebo treatments were administered to the left forearm, while active SAM treatments were applied to the right forearm in a contralateral design. For groups B and D, placebo treatments were administered to the right forearm, while active SAM treatments were applied to the left forearm (Figure 2). The treatment side was selected by flipping a coin.
CONSORT flow diagram of study inclusion/exclusion test subjects, randomization, calibration, baseline, and intervention period.
Sustained acoustic medicine (SAM) stimulation setup: (A) application to lateral forearm position for all four study groups (A–D), (B) graphic illustration of SAM x1 and probe positioning.
Participants were instructed to refrain from strenuous exercise and only indulge in day-to-day activities. The study was conducted during daily working hours (9 am—5 pm EST) in a well-controlled environment at 20°C. Participants were seated comfortably in an upright position for 15 min before and throughout the 60 min stimulation period (Figure 2). A high-power Laser Doppler Flowmetry (LDF) probe was positioned 2.5 cm distal to the elbow, between the two SAM x1 transducers, to monitor changes in blood circulation and skin temperature during stimulation. Patches were placed over the cables 5 cm equidistant from the probe's laser location to minimize any excess movement from the LDF device. Participants were checked every 15 min to ensure comfort and were permitted to watch pre-selected television shows or listen to music during the procedure. Each participant received $100 compensation at the completion of the study.
Continuous data acquisition was performed using the LDF software provided by the manufacturer during a 5 min calibration period, a 10 min baseline period, and a subsequent 60 min stimulation period. Measurements were recorded at 10 min intervals throughout the entire baseline and stimulation periods for analysis. No data was analyzed during the 5 min calibration period.
Instrumentation
The study utilized the dual SAM x1 device and four ultrasound coupling patches (two per forearm) to deliver active or placebo ultrasound treatment for one hour per subject. All the devices were new and calibrated prior to application. The patches were prefilled with 3 ml of coupling gel containing either standard coupling ultrasound gel or 2.5% diclofenac gel (Compounded Solutions, Monroe, CT).
A high-power Laser Doppler Flowmetry (LDF) system (VMS-LDF2-HP, Moor Instruments, UK), connected to non-invasive skin probes (VP2-V2-HP), was employed to measure real-time circulation and skin temperature. The system operated with a 785 nm, 20 mW laser, and probes were calibrated with polystyrene latex particle suspensions before each session, following manufacturer instructions. The LDF system continuously recorded data during the 1 h, 15 min protocol.
Circulation was quantified as flux perfusion units (PU), representing the red blood cell movement rate at 1–3 mm below the skin's surface, alongside temperature in degrees Celsius. Data was analyzed using moorVMS-PC research software and exported into Excel for biostatistical analysis.
This study, supported by Minority Health and Health Disparities (Project ID: MD015912), assessed the mechanotransduction performance of the wireless SAM x1 device (model SA551) with diclofenac and aqueous coupling gels.
Statistical analysis
A statistical analysis was conducted to evaluate differences in blood flow and temperature between placebo and active treatment arms using coupling and 2.5% diclofenac gel. The primary factor analyzed was the SAM stimulation (active or placebo), with gel type (water-based or diclofenac gel) considered as an interaction factor. Raw data was aggregated, normalized in Microsoft Excel, and analyzed by an independent biostatistician using R programming.
Data analysis included baseline and treatment intervals measured every 10 min. A two-way ANOVA was employed to compare group means and assess the independent and interaction effects of SAM active or placebo treatment and aqueous or 2.5% diclofenac gel type. A post hoc test was used to determine p-values for the two-way ANOVA data. Descriptive statistics for demographic data were calculated using chi-square tests for categorical variables and t-tests for the means between the active and placebo groups at the 10 min intervals.
Statistical significance was defined as p < 0.05, with results presented as mean ± standard deviation (SD) unless stated otherwise. Confidence intervals (95%) and p-values were reported to provide additional statistical context. Graphical representations, including error bars denoting standard error of the mean (SEM), and data tables were generated using R and Excel.
Results
Subject enrollment demographics
Sixty-four participants were selected for the study after physical examination and randomly assigned to four groups (n = 32), applying for a contralateral study design. The demographic data shows no significant differences between sex, age, BMI, and pulse rate before the start of the stimulation (Table 1).
Circulation results
SAM stimulation significantly enhanced circulation and tissue perfusion during 60 min with standard coupling gel or 2.5% Diclofenac gel. With standard coupling gel, circulation increased to a maximum mean difference of 20.93 PU (95% CI: 12.89 to 28.87; p = 0.0001) compared to placebo at 50 min. Similarly, SAM with 2.5% Diclofenac gel achieved a maximum mean difference of 21.56 PU (95% CI: 15.92 to 27.21; p = 0.001) vs. placebo at 50 min (Table 2).
Both groups exhibited statistically significant increases in circulation compared to placebo at 10 min (Coupling Gel: 95% CI: 0.80 to 3.36; p = 0.0032; Diclofenac Gel: 95% CI: 0.78 to 3.68; p = 0.0037), with effects sustained throughout the duration of stimulation (Figure 3). No significant differences were observed between the two active SAM-stimulated groups, while placebo groups without SAM stimulation showed no significant changes in circulation (Figure 3). These findings show that SAM stimulation effectively enhances circulation, irrespective of the coupling medium.
Normalized circulation is below lateral forearm skin averaged at each 10 min segment for baseline and stimulation periods. (** p < 0.005, **** p < 0.0005 between Coupling Gel + Placebo and Coupling + SAM, ### p < 0.005, #### p < 0.0005 between 2.5% Diclofenac).*
Temperature results
SAM treatment significantly increased tissue temperature over 60 min of stimulation compared to the placebo group. When paired with coupling gel, temperature increased by 2.67°C (95% CI: 2.35 to 2.99, p = 0.0001), while using 2.5% diclofenac gel resulted in a 2.40°C increase (95% CI: 2.04 to 2.75, p = 0.0001) (Table 3). Both SAM-treated groups exhibited a gradual rise in tissue temperature, with significant differences observed after 20 min of stimulation and sustained gradual increases through 60 min. No significant differences were noted between the coupling gel and diclofenac gel groups. The placebo groups did not show temperature change during the 60 min period (Figure 4).
Normalized temperature change at lateral forearm skin averaged at each 10 min segment for baseline and stimulation periods. [** p < 0.005, **** p < 0.0005 between Coupling Gel + Placebo and Coupling + SAM, ### p < 0.005, #### p < 0.0005 between 2.5% Diclofenac Gel + Placebo and Diclofenac + SAM, Error bar represent (SEM)]. SEM bars are present in placebo groups however they are not visible.*
Total cumulative circulation results
Temporal cumulative circulation showed a significant increase in both the Coupling Gel and 2.5% Diclofenac Gel groups during 60 min of SAM stimulation. Significant changes were observed as early as 10 min (Coupling Gel: 95% CI, 778.95 to 2926.14, p = 0.0014; 2.5% Diclofenac Gel: 95% CI, 929.72 to 2872.99, p = 0.0004) (Table 4). Over the stimulation period, both treatment groups demonstrated a rapid, sustained increase in blood flow, with mean differences of 116,000 PU (SAM + Coupling Gel) and 136,000 PU (SAM + 2.5% Diclofenac Gel) compared to the respective placebo treatments (p = 0.0001). Importantly, both active treatments showed similar sustained blood flow increases with SAM stimulation, whereas placebo groups exhibited no significant cumulative flux change over 60 min (Figure 5).
Cumulative circulation changes at the lateral forearm over 60 min treatment period. [** p < 0.005, **** p < 0.0001 between Coupling Gel + Placebo and Coupling + SAM, ### p < 0.005, #### p < 0.0001 between 2.5% Diclofenac Gel + Placebo and Diclofenac + SA, Error bar represent (SEM)].*
Discussion
Sustained Acoustic Medicine (SAM) stimulation significantly improves blood circulation and induces diathermic effects in soft tissue when applied with standard ultrasound coupling gel or 2.5% diclofenac gel during a 60 min session. Importantly, adding diclofenac sodium does not alter SAM's hyperemia or diathermic effects. Placebo groups exhibited no localized blood flow or temperature changes, confirming that these effects are directly attributable to SAM stimulation.
Managing musculoskeletal (MSK) disorders necessitate precise modulation of mechanical stress, angiogenesis, tissue perfusion, and inflammatory responses. These processes involve macrophages, neutrophils, mast cells, and cytokines such as interleukins and tumor necrosis factor-alpha (TNF-α) (34). Adequate blood flow is essential to regulate the treatment by ensuring the delivery of oxygen, nutrients, immune cells, and growth factors. Conversely, impaired blood flow or reduced angiogenesis can disrupt the balance between pro- and anti-inflammatory cytokines and reduce the expression of key angiogenic and vasodilatory mediators such as vascular endothelial growth factor (VEGF), fibroblast growth factor (FGF), and endothelial nitric oxide synthase (eNOS) (35, 36), Biomechanical stimulation, localized shear and axial stress promotes the angiogenesis and blood flow by activating VEGF-2, FGF and eNOS (37–39). Mechanotransduction also regulates inflammatory mediators, including TNF-α, IL-1β, and macrophages (38, 40–43).
SAM provides targeted biomechanical forces (compression and rarefaction), providing the essential mechanical stimulus to upregulate the expression of VEGF, FDF, and eNOS over a long period of time, enhancing the angiogenesis, blood flow and regulating inflammatory responses (6, 20, 44). The diathermic effects of SAM include thermal stimuli that induce vasodilation, improve blood flow, and stimulate cellular metabolism, proliferation, and tissue regeneration (7, 17, 19). Hendren et al. demonstrated significant temperature increases at 1 cm, 2 cm, and 5 cm depths with SAM stimulation, retaining the high temperature above the therapeutic threshold deep into the tissue with little or no adverse effects (45). The biomechanical and thermal modulation of SAM treatment provides the essential stimuli to induce localized angiogenesis and enhanced blood flow to increase oxygen and nutrients and regulate the inflammatory factors to expedite tissue healing.
The regulation of the COX1/COX2 pathway has a crucial role in regulating inflammatory factors and MSK pain. COX1 is essential to retain tissue mucosal integrity and platelet aggregation, and Cox2 expression upregulates the inflammation such as IL-1β, TNF-α contributing to pain and tissue degradation (46). Diclofenac sodium, an anti-inflammatory agent, inhibits PGE2 and cytokines like IL-1β, TNF-α, and VEGF. Diclofenac sodium, a non-selective COX inhibitor, effectively reduces these inflammatory mediators. However, prolonged systemic administration is associated with gastrointestinal and renal side effects (47). Topical diclofenac application improves its safety profile, and its efficacy is limited by the low permeability of the stratum corneum (29, 31, 48). Biomechanical and thermal effects disrupt the skin's lipid bilayers, and losses in the skin's extracellular matrix increase skin porosity (49). Furthermore, US induced cavitation, formation and oscillation of microbubbles, allow the skin to enhance transdermal drug delivery (49–51). SAM long-duration acoustic stimulation enhances skin permeability, facilitating sustained transdermal drug delivery over a long duration. Masterson et al. observed an increase in vitro diclofenac delivery after 4 h of SAM stimulation (52). Madzia et al. reported significant reductions in knee osteoarthritis pain and improved mobility with SAM plus 1% diclofenac sodium (53). Jarit et al. demonstrated that a 4-week intervention using SAM with 2.5% diclofenac gel resulted in 99.3% of patients experiencing pain reduction and 97.8% showing improved function (54).
The study shows little or no significant change in the first 10 min of treatment, there is little change in tissue temperature as body adjust to the SAM stimulation, a significant rise was recorded between after 10 min of stimulation and continued over next 40 min (50 min after the start of treatment) as body start accumulate with the biomechanical and thermal stimulation. The change in blood flux followed the same pattern observed in the increase in the local temperature, exhibiting the relation between the temperature increase and blood circulation. The cumulative flux analysis shows that the quantity of blood flow over time significantly increases in the treated site relative to placebo sites. Placebo-treated sites did not show little or no temperature and flux change, indicating that change in blood circulation was due to the SAM treatment and not systemic physiological changes. The presence of 2.5% diclofenac sodium did not alter SAM's biomechanical or diathermic effects, demonstrating that diclofenac integration does not interfere with the therapeutic ultrasound mechanisms. Both US coupling gel and 2.5% diclofenac gel followed a similar pattern for active and placebo devices, demonstrating that the addition of diclofenac would not affect the SAM thermal and biomechanical effects and making an effective device to be applied for transdermal drug delivery.
Collectively, SAM combined with diclofenac sodium provides a dual-modality approach that leverages mechanical and thermal stimulation alongside pharmacological anti-inflammatory effects, offering a potent and non-invasive strategy for treating MSK disorders. Future research should evaluate the combined efficacy of SAM and topical diclofenac in broader clinical populations, including patients with knee osteoarthritis, low back pain, and other chronic MSK conditions. Furthermore, SAM efficacy with other NSAIDs would be evaluated, and data compared with diclofenac to determine the most effective combination to treat MSK disorders.
Conclusion
Continuous, long-duration ultrasound treatment using the SAMx1 device significantly enhances circulation to localized soft tissues. This study demonstrates that SAM effectively increases tissue perfusion with standard ultrasound coupling gel and 2.5% diclofenac gel. Adding diclofenac did not alter the hyperemic and diathermic effects observed throughout the stimulation period. Future studies will explore SAM's hyperemic and diathermic effects at additional anatomical locations and in populations with specific conditions and MSK disorders.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chen N Fong DYT Wong JYH. Health and economic outcomes associated with musculoskeletal disorders attributable to high body mass index in 192 countries and territories in 2019. JAMA Netw Open. (2023) 6(1):e 2250674. 10.1001/jamanetworkopen.2022.5067436662529 PMC 9860530 · doi ↗ · pubmed ↗
- 2Cieza A Causey K Kamenov K Hanson SW Chatterji S Vos T. Global estimates of the need for rehabilitation based on the global burden of disease study 2019: a systematic analysis for the global burden of disease study 2019. Lancet. (2021) 396(10267):2006–17. 10.1016/S 0140-6736(20)32340-033275908 PMC 7811204 · doi ↗ · pubmed ↗
- 3Gallagher S Heberger JR. Examining the interaction of force and repetition on musculoskeletal disorder risk: a systematic literature review. Hum Factors. (2013) 55(1):108–24. 10.1177/001872081244964823516797 PMC 4495348 · doi ↗ · pubmed ↗
- 4Garnæs KKMørkved STønne T Furan L Vasseljen O Johannessen HH. Mental health among patients with chronic musculoskeletal pain and its relation to number of pain sites and pain intensity, a cross-sectional study among primary health care patients. BMC Musculoskelet Disord. (2022) 23(1):1115. 10.1186/s 12891-022-06051-936544130 PMC 9773452 · doi ↗ · pubmed ↗
- 5Juopperi S Sund R Rikkonen T Kröger H Sirola J. Cardiovascular and musculoskeletal health disorders associate with greater decreases in physical capability in older women. BMC Musculoskelet Disord. (2021) 22(1):192. 10.1186/s 12891-021-04056-433593350 PMC 7888167 · doi ↗ · pubmed ↗
- 6Uddin S Komatsu D Motyka T Petterson S. Low-intensity continuous ultrasound Therapies-A systematic review of current state-of-the-art and future perspectives. J Clin Med. (2021) 10(12):2698. 10.3390/jcm 1012269834207333 PMC 8235587 · doi ↗ · pubmed ↗
- 7Petterson S Plancher K Klyve D Draper D Ortiz R. Low-intensity continuous ultrasound for the symptomatic treatment of upper shoulder and neck pain: a randomized, double-blind placebo-controlled clinical trial. J Pain Res. (2020) 13:1277–87. 10.2147/JPR.S 24746332606899 PMC 7287226 · doi ↗ · pubmed ↗
- 8Zhou J Ning E Lu L Zhang H Yang X Hao Y. Effectiveness of low-intensity pulsed ultrasound on osteoarthritis: molecular mechanism and tissue engineering. Front Med. (2024) 11:1292473. 10.3389/fmed.2024.1292473 PMC 1106136138695024 · doi ↗ · pubmed ↗