Complication of endoscopic vacuum therapy in anastomotic leak: closure of iatrogenic small bowel fistula using a novel helix tacking device
Ahmed Alwali, Clemens Schafmayer, Imad Kamaleddine

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
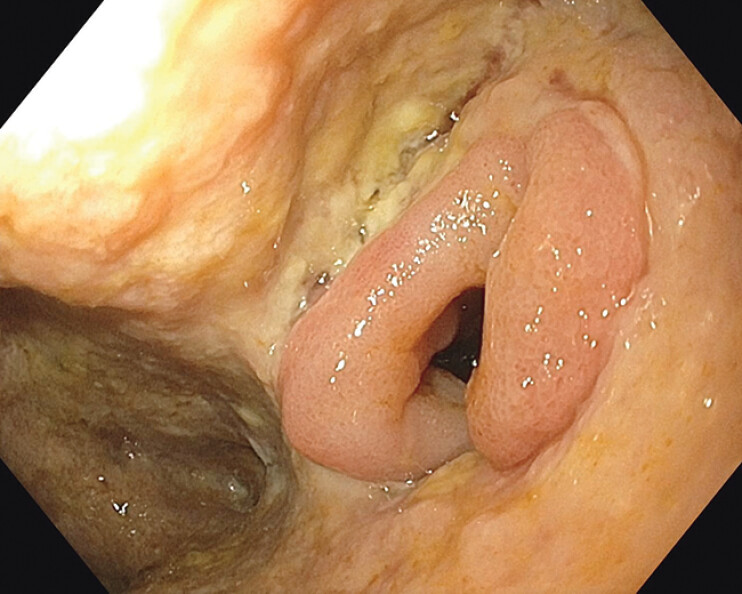 Fig. 1
Fig. 1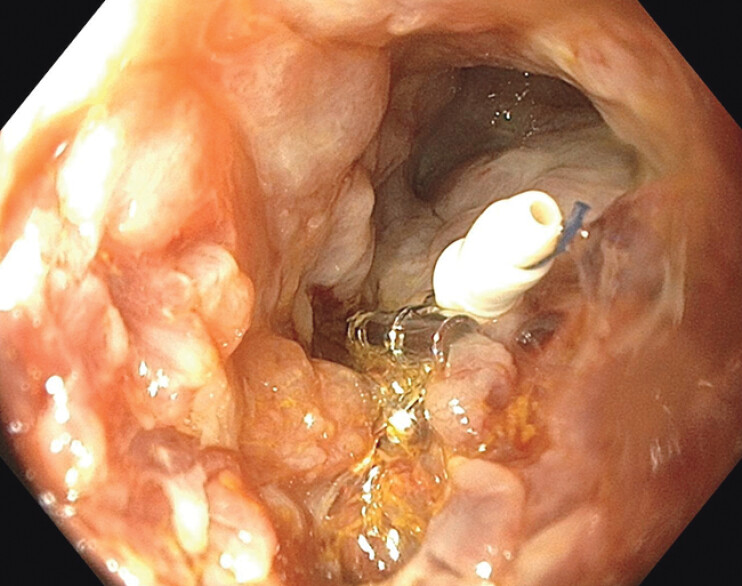 Fig. 2
Fig. 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Abdominal Surgery and Complications · Diverticular Disease and Complications
Endoscopic vacuum therapy is an effective technique for managing colorectal anastomotic leaks 1 . However, its use in cases of intra-abdominal anastomotic leaks should be performed with caution in experienced centers due to the high risk of complications, such as iatrogenic fistulas 2 . This case highlights a novel endoscopic suturing approach to close a small bowel fistula that developed as a complication of endoscopic vacuum therapy for an anastomotic leak after colorectal surgery.
A 66-year-old man underwent Hartmann’s reversal 6 months after surgery for perforated sigmoid diverticulitis. One week postdischarge, he presented with abdominal pain and elevated infection markers. A computed tomography scan and endoscopy confirmed an anastomotic leak 16 cm from the anal verge with an extra-luminal cavity. As the patient showed no signs of peritonitis and the 18th postoperative day was not ideal for reoperation or stoma diversion, conservative management was chosen. After endoscopic lavage, endoscopic intraluminal vacuum therapy (EndoSponge; B. Braun, Melsungen, Germany) was initiated, along with antibiotics therapy and a liquid diet.
Over 10 days, the patient’s condition improved. However, he developed new abdominal pain with rising infection markers. Small bowel contents were observed draining from the lower pole of the laparotomy wound. Endoscopy revealed an opening in a small bowel loop within the insufficiency cavity, suggesting a fistula likely caused by vacuum therapy ( Fig. 1 ).
Endoscopic view of an opening in a small bowel loop within the insufficiency cavity, suggesting a fistula likely caused by vacuum therapy.
Initial attempts to close the fistula with endoscopic clips failed. The daily fistula output was 1,500 mL. Endoscopic suturing with a novel helix tacking device (X-Tack, Apollo Endosurgery, Austin, TX) was performed, reducing output significantly to 100 mL/d ( Fig. 2 ). Vacuum therapy continued for 2 weeks with sponge changes every 3 days to promote granulation. The output decreased to 20 mL/d and oral intake was gradually resumed. The patient was discharged in good condition for outpatient follow-up. Three-month follow-up showed a chronic cavity with granulation tissue but no persistent fistula. No discharge was observed from the laparotomy wound ( Video 1 ).
Closure of small bowel fistula using the X-Tack device.
This video demonstrates a novel approach for closing an iatrogenic small bowel fistula within the anastomotic insufficiency cavity after colorectal surgery using the X-Tack device.Video 1
Endoscopy_UCTN_Code_CPL_1AJ_2AJ
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kouladouros K Applications of endoscopic vacuum therapy in the lower gastrointestinal tract: Tips and tricks and a review of the literature Best Pract Res Clin Gastroenterol 20247010192739053980 10.1016/j.bpg.2024.101927 · doi ↗ · pubmed ↗
- 2Bemelman WA Arezzo A Banasiewicz T Use of sponge-assisted endoluminal vacuum therapy for the treatment of colorectal anastomotic leaks: expert panel consensus BJS Open 20226 zrac 12336268752 10.1093/bjsopen/zrac 123PMC 9585396 · doi ↗ · pubmed ↗