Bilateral middle ear cholesteatoma in children: A single-center retrospective study
Xiaoxu Wang, Lining Guo, Enxia Tian, Min Chen, Wei Liu, Xin Ni, Jie Zhang

TL;DR
This study examines the treatment and outcomes of children with bilateral middle ear cholesteatoma, highlighting the importance of staged surgery and long-term follow-up due to high recurrence rates.
Contribution
The study proposes a management flowchart for bilateral middle ear cholesteatoma in children based on clinical experience and outcomes.
Findings
Staged bilateral surgery is preferred, with surgery on the worse side first.
Postoperative hearing showed no significant difference between congenital and acquired cholesteatoma.
Bilateral middle ear cholesteatoma has a high recurrence rate requiring long-term follow-up.
Abstract
•The incidence of cleft palate malformation in BMEC is high.•Staging bilateral surgery is preferred and surgery on the worse side first.•Simultaneous bilateral surgery in children should be carefully considered.•Postoperative hearing showed no significant difference between CC and AC in BMEC.•BMEC has a high recurrence rate after operation and require a long-term follow-up. The incidence of cleft palate malformation in BMEC is high. Staging bilateral surgery is preferred and surgery on the worse side first. Simultaneous bilateral surgery in children should be carefully considered. Postoperative hearing showed no significant difference between CC and AC in BMEC. BMEC has a high recurrence rate after operation and require a long-term follow-up. To analyze the clinical characteristics of bilateral cholesteatoma in children and summarize the clinical treatment pathway. In this…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
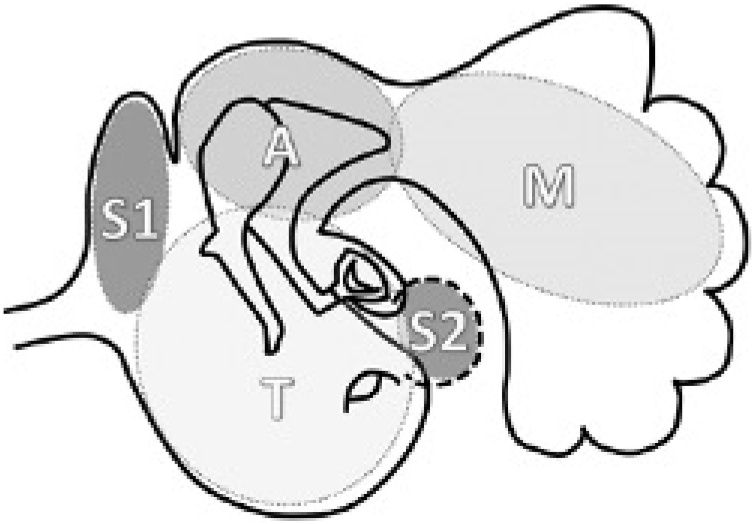 Figure 1
Figure 1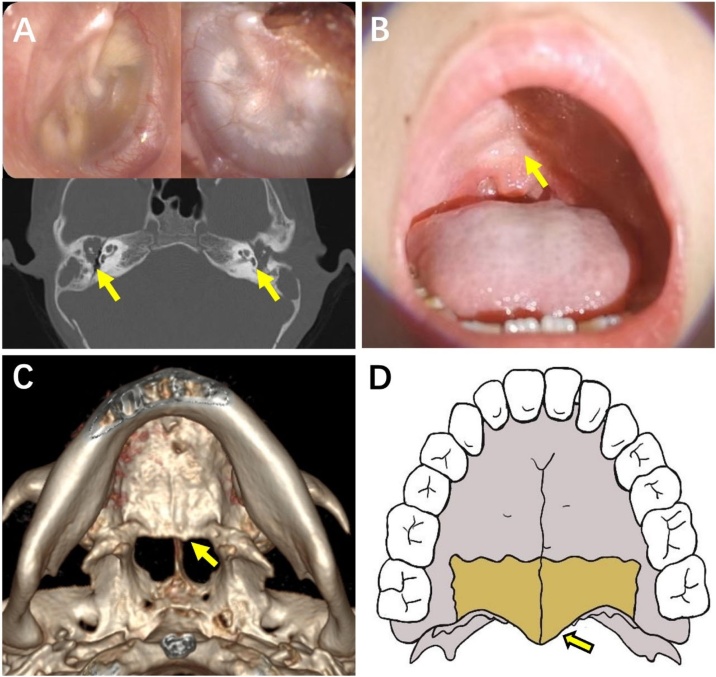 Figure 2
Figure 2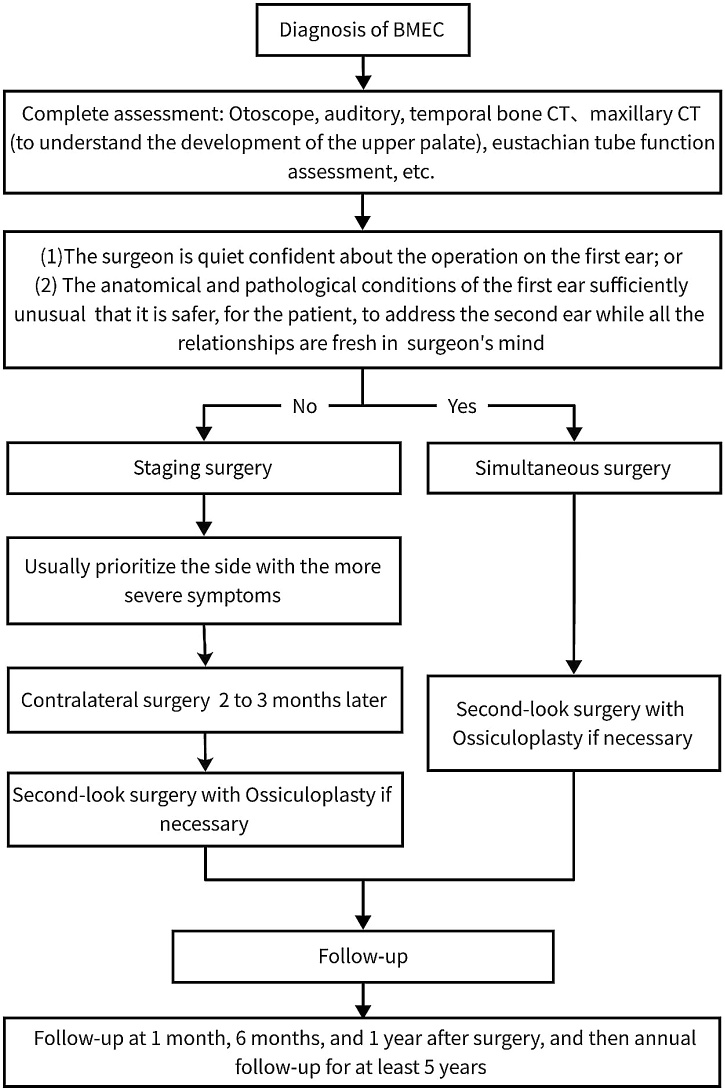 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCleft Lip and Palate Research · Ear Surgery and Otitis Media · Congenital Ear and Nasal Anomalies
Introduction
Cholesteatoma is a mass formed by the keratinizing, squamous epithelium in the tympanic cavity and/or mastoid and subepithelial connective tissue, and progressive accumulation of keratin debris.1 Although cholesteatomas are not true tumors, they can proliferate, and erode and destroy the structure of the middle ear, resulting in hearing loss and serious intracranial and extracranial complications. The annual incidence of middle ear cholesteatoma is approximately 12.6 per 100,000 in adults, and 3 per 100,000 in children.2 Among them, the incidence of binaural disease is about 4.4 %–17.1 %.3, 4
In children, Bilateral Middle Ear Cholesteatoma (BMEC) can cause bilateral hearing loss and requires long-term medical treatment. It can have a serious effect on children’s learning and social adaptation and may affect the speech development of young children. The treatment strategy of BMEC needs more consideration. Published literature on BMEC is limited to a few small series and case reports published during previous decades.5, 6, 7, 8 Currently no standard protocols are available for the management of BMEC in children. Retaining or improving hearing and reducing the recurrence rate make management challenging. In this paper, we review previous cases of BMEC treated at our institution and propose a treatment algorithm based on our experience to improve the understanding of the disease and provide guidance for clinical diagnosis and treatment.
Methods
Study design
A retrospective chart and surgical video review were completed for children with BC who underwent surgery at the Otolaryngology Department of Beijing Children’s Hospital between 2016 and 2023. The inclusion criteria were age ≤18-years, completed the first surgical treatment of BMEC in our department, and were followed up for more than 1-year. Patients with incomplete medical records were excluded. All cholesteatoma diagnoses were pathologically confirmed. The data included details on patient demographics, medical history, physical examination, imaging, extent of lesions, degree of mastoid development, audiometry, treatment and follow-up, and outcome.
The classification of cholesteatoma is divided into CC and AC according to the definition of the European Academy of Otology and Neurotology and Japan Otological Society (EAONO/JOS).1 The extent of cholesteatoma was described using the STAM staging system also proposed by EAONO/JOS.1 The middle ear and mastoid space were divided into four sites: difficult to access Sites (S), the Tympanic cavity (T), the Attic (A) and the Mastoid (M). The difficult access Sites (S) included S1, the supratubal recess, and S2, the sinus tympani (Fig. 1). The degree of mastoid development was classified into three types according to the finding on Computed Tomography (CT) of the temporal bone CT: pneumatic type (numerous large air cells, with high translucency and honeycomb shape); diploetic type (part of the mastoid is pneumatized, with small and dense air cells); and sclerotic type (the mastoid is composed of compact bone). According to the age and degree of cooperation of the children, hearing was tested using pure-tone audiometry or game audiometry. The Pure-Tone Average (PTA) was defined as the average of hearing sensitivity thresholds to pure-tone signals at 500, 1000, 2000, and 4000 Hz.Fig. 1. Divisions of the middle ear space using the STAM system.1 S, The difficult access sites (includes S1, the Supratubal recess and S2, the Sinus tympani); T, Tympanic cavity; A, Attic; M, Mastoid.Fig. 1
The cholesteatoma resection procedures included Canal Wall Up (CWU), Canal Wall Down (CWD), and Transcanal Endoscopic Ear Surgery (TEES). The specific surgical method is selected based on the extent of the lesion. The ossiculoplasty were divided into five categories according to the different condition: (1) With Partial Ossicular Replacement Prosthesis (PORP), (2) With Total Ossicular Replacement Prosthesis (TORP), (3) With tragus cartilage, (4) With complete ossicular chain and no need for ossiculoplasty, and (5) Without ossiculoplasty for various special reasons.
The main outcome indicators were recurrence of cholesteatoma, and postoperative long-term hearing results. The diagnosis of recurrence was based on clinical examination, otoscopy findings, or performance of Diffusion-Weighted Imaging Magnetic Resonance Imaging (DWI MRI) after surgery. The postoperative long-term hearing results were determined at the most recent follow-up (at least 1-year after the surgery).
This study was approved by the Research Ethics Board of Medical Ethics Committee, Beijing Children’s Hospital Affiliated to Capital Medical University and the study was conducted in accordance with the principles of the Declaration of Helsinki and its later amendments. The research ethics board waived the requirement for written informed consent owing to the retrospective study design.
Statistical analysis
Statistical analysis was performed using SPSS 27. Continuous variables were reported as means and standard deviations or medians and ranges, and categorical variables were reported as frequencies and percentages. The normality test used the Shapiro-Wilk test. Paired t-test was used for hearing results before and after surgery. Based on the non-normal distribution of the data, Kruskal Wallis was used to compare the prognosis of hearing with different conditions; p-values <0.05 were considered statistically significant.
Results
Between 2016 and 2023, a total of 320 pediatric with cholesteatoma were treated in our department, including 12 cases of BMEC with 4 girls and 8 boys. Their characteristics are shown in Table 1. The mean age at diagnosis was 6.5 ± 2.6-years (rang from 2.5 to 9.8), with only one child aged younger than 3-years. The mean duration of follow-up was 4.28 ± 2.58-years.Table 1. Demographic data and medical information of 12 children with bilateral middle ear cholesteatoma.Table 1IDSexAgea (years)SideClassificationCourseb (months)Palate developmentMastoid developmentExtensionPer-operative PTA (dB)Binaural surgery interval (months)SurgeryPostoperative recurrence and timeTotal number of operationsOssiculoplastyPost-operative PTA (dB)Follow up time (years)1B9.5RAC84Cleft palateDiploeticSTAM62.536CWUYes (0.8 years)3Without46.255LAC84DiploeticSTAM62.5CWDNOCartilage40.02B3.3LAC1Cleft lip and palateDiploeticSTA63.751CWUYes (2 years)3Without62.59RAC1DiploeticSTA32.5CWUNOTORP38.753B7.0LAC24WithoutPneumaticSTAM36.254CWUNO3PORP31.251.3RAC24PneumaticSTAM38.75CWUNOPORP30.04B3.4LAC2Occult submucosal cleft palateDiploeticSTAM20.08CWUNO3No Need16.258.8RAC2DiploeticSTA30.0CWUYes (2.5 years)Cartilage505G9.5RAC24Occult submucosal cleft palateScleroticSTAM65.036CWUYes (3 years)3Without52.04LAC0ScleroticSTA10.0CWUNONo Need10.06G9.8LAC12WithoutDiploeticSTAM57.513CWUYes (0.9 years)3Without65.01.7RAC24DiploeticSTAM41.25CWDNOCartilage31.257B7.4LCC6WithoutDiploeticT10.00TEESNO2No Need31.255RAC6PneumaticSTAM35.0CWDNOTORP37.58G5.8RAC12Cleft palateDiploeticSTAM61.2516CWDNO2Cartilage51.255.3LCC0DiploeticSTA55.0CWUNOPORP26.259B2.5LCC3Occult submucosal cleft palateDiploeticT35.01CWUYes (1.3 years)4TORP36.254.4RAC3DiploeticSTAM40.0CWUYes (1.5 years)TORP55.010G9.2RAC1Occult submucosal cleft palateDiploeticSTAM37.252CWDNO2Without46.252LAC0DiploeticSTA37.5CWDNOCartilage45.011B4.8RAC12Occult submucosal cleft palateDiploeticSTAM56.253CWDNO2PORP12.53LCC0.3DiploeticTAM21.25CWUNOPORP32.512B5.9LAC36Occult submucosal cleft palateDiploeticSTAM35.02CWDNO2TORP35.01.8RAC36DiploeticSTAM46.25CWDNOPORP25.0AC, Acquired Cholesteatoma; CC, Congenital Cholesteatoma; S, The difficult access sites; T, Tympanic cavity; A, Attic; M, Mastoid; CWU, Canal Wall Up; CWD, Canal Wall Down; TEES, Transcanal Endoscopic Ear Surgery; PORP, Partial Ossicular Replacement Prosthesis; TORP, Total Ossicular Replacement Prosthesis; PTA, Pure-Tone Average.aAge: Age at first diagnosis of middle ear cholesteatoma.bCourse: Duration of ear symptoms.
Four children had CC in one ear and AC in the other ear and 8 children had AC in both ears. The course of disease in the bilateral ears of the same child is different, but there is no significant difference statistically (p = 0.264, t = 1.178). Three children (Cases 6, 10, and 11) had a different course of disease in bilateral ears and two children (Cases 5 and 8) had unilateral middle ear cholesteatoma at the time of their first visit and subsequently developed a cholesteatoma in the contralateral ear. The extent of the lesions differed in bilateral ears in 6 children (Cases 4, 7, 8, 9, 10 and 11) were different. Nine children had maxillary developmental deformities (75%) (cleft palate in 3 cases and occult submucosal cleft palate in 6 cases), all of nine children were accompanied by diploetic or sclerotic type mastoid. Fig. 2 shows the details of a BMEC in a child (Case 12) with occult submucosal cleft palate. There was only 1 case of pneumatolytic type in bilateral mastoid.Fig. 2. Case 12. (A) Otoscope and CT scan on temporal bone. (B) An inverted V-shaped depression at the junction of the soft palate and the hard palate. (C) The three-dimensional reconstruction of the maxillary CT scan confirmed the absence of posterior nasal spine. (D) The hand drawing shows a complete posterior nasal spine structure.Fig. 2
The surgical treatment varied according to the severity of the lesion. The specific surgical methods and ossiculoplasty are shown in Table 1. Only one child (Case 7) underwent simultaneous binaural operation, and the other 11 children underwent staged surgery. The median interval between the first and second surgery was 3-months (range: 1–12 months). Six children (7-ears) (Cases 1, 2, 4, 5, 6, and 9) experienced a recurrence. In the revision operation due to recurrence, 6-ears underwent CWD and one ear underwent CWU surgery. The ossiculoplasty may be performed in the first or second-look stage. The final procedure method used for ossiculoplasty is shown in Table 1. The mean number of operations per patient was 2.67 ± 0.65. The mean preoperative PTA was 41.23 ± 16.50 dB, and the mean long-term postoperative PTA was 37.79 ± 14.42 dB. There was no significant difference in hearing results between preoperative and postoperative patients (p = 0.291, t = 1.082). No postoperative complications such as sensorineural deafness or facial paralysis were observed in any of the children.
There was no significant difference in postoperative hearing between CC and AC (p = 0.355, F = 4.268). There were significant differences in postoperation hearing among different surgical methods (p = 0.006, H = 12.630). In pairwise comparison, there were significant differences in postoperative hearing between the CWU group and the group undergoing recurrent surgery (p = 0.003). There was no significant difference between the other groups. There were significant differences in postoperation hearing among different ossiculoplasty methods (p = 0.001, H = 17.590). In a pairwise comparisons, there was significant difference in hearing outcomes between the without ossiculoplasty group and PORP group (p = 0.006). There was significant difference between the without ossiculoplasty group and no need ossiculoplasty group (p = 0.013). And among the other groups there were no significant differences (Table 2).Table 2. The relationship between long-term postoperative hearing prognosis and classification, surgical methods and ossicloplasty methods.Table 2. CategorynPostoperative PTA (x ± S dB)pTest statisticsClassificationAC2039.04 ± 15.460.355F = 4.268CC431.56 ± 4.13SurgeryCWU726.43 ± 9.990.006H = 12.630CWD935.97 ± 11.90TEES131.25Recurrence surgery752.43 ± 9.76OssiculoplastyPORP626.25 ± 7.330.001H = 17.590TORP540.50 ± 8.20Cartilage543.50 ± 8.16No need319.17 ± 10.92Without554.40 ± 8.90Overall‒2437.79 ± 14.42‒‒AC, Acquired cholesteatoma; CC, Congenital Cholesteatoma; CWU, Canal Wall Up; CWD; Canal Wall Down; TEES, Transcanal Endoscopic Ear Surgery; PORP, Partial Ossicular Replacement Prosthesis; TORP, Total Ossicular Replacement Prosthesis; PTA, Pure-Tone Average.
Discussion
This paper reports 12 cases of BMEC in children. To our knowledge, this is the largest case series on children to date with complete long-term follow-up data. This study revealed that the age at diagnosis was relatively young, with a median age of 6.5-years (considering the delay in diagnosis, the age of onset is likely to have been younger). In addition, bilateral ears had different course, different degrees of lesion, and lesions at different locations. The BMEC in this study included both congenital and acquired, and the pathogenic mechanisms are likely to have been multifactorial. In our cases, palatal malformations, including cleft palate and occult submucosal cleft palate, were important risk factors. According to previous studies, children with cleft palate are prone to middle ear cholesteatoma and otitis media because of abnormalities in Eustachian tube anatomy and function, viscosity of middle ear effusion, and frequency of middle ear infection.9 The incidence of cholesteatoma in children with cleft palate is between 1.5% and 5.9%, which is 200 times higher than that in the general population.10, 11, 12 It is worth paying attention to that children with occult submucosal cleft palate are also susceptible to BMEC. In this study, 3 children had cleft palate, and 6 children had occult submucosal cleft palate. Occult submucosal cleft palate is caused by the defect of a part of the posterior nasal spine of the hard palate.13 Physical examination shows an inverted V-shaped depression at the junction of the soft palate and the hard palate when making an “ah” sound (Fig. 2B), with or without speech impediments. The diagnosis of occult submucosal cleft palate in children is often overlooked because the defect is not easily detected. The middle ear problems associated with occult submucosal cleft palate have not been reported. The palate should be carefully monitored during physical examination. If signs of occult submucosal cleft palate are present, attention should be paid to middle ear problems in the early stage. In addition, habitual sniffing extraction caused by patulous eustachian tube may be related to the pathogenesis of BMEC14, 15 owing to the presence of total closing failure, with an intermittent free transfer of respiratory pressure to the middle ear, the sniffing procedure maintains a negative intratympanic pressure, gradually forming an attic retraction pocket.16 However, in our children, no patulous eustachian tube was found. Additional etiologies of BMEC requires analysis of a larger samples.
In the case of binaural lesions, repeated surgeries and bilateral hearing loss can have a significant impact on children’s development, and complete removal of the lesion and protection of hearing are particularly important. In terms of the surgical treatment strategy, the first choice is between simultaneous or staged surgery. In the traditional experience, bilateral chronic middle ear disease is typically performed by staging surgery for the risk of iatrogenic bilateral sensorineural hearing loss, bilateral facial nerve injury, and temporary bilateral hearing loss during the recovery period in simultaneous binaural surgery. However, there are also arguments for the advantages of simultaneous binaural surgery, such as reduces the cost of surgery and improves convenience for patients and surgeons. We tend to believe that staging surgery is preferred. But if you are quite confident in the surgery for the first ear won’t be injured, simultaneous binaural surgery can be considered. Of the 12 children in our group, 11 underwent binaural staged surgeries and only one underwent simultaneous surgery. The simultaneous surgery was performed because one of his first ear is CC with a very limited small lesion and without any structural damage, the surgery of the ear went very smoothly and quick under otoscopy. In all staged surgeries, the more severe side is selected first. For the Klemens et al.17 suggested another situation that surgeons should consider before surgery of bilateral: Are the anatomical and pathological conditions of the first ear sufficiently unusual or difficult that it is safer, for the patient, to address the second ear while all the relationships are fresh in the surgeon’s mind?. We haven't encountered this unusual situation, but it's worth considering. In summary, simultaneous binaural surgery in children requires more caution and certainty.
In this study, there was no statistical difference in hearing changes before and after surgery, but the PTA of long-term hearing after surgery was better than that before surgery. And there was no significant difference in hearing outcomes between CC and AC. The hearing outcomes were worse in the group that did not undergo ossiculoplasty and worse in the group that underwent recurrent surgery. And there was no significant difference in hearing prognosis between CWU, CWD and TEES groups. There was No statistical difference between PORP, TORP, Cartilage and did not need ossiculoplasty groups. However, the limitation is that the sample size of each group is small. The specific surgical method and the type of ossiculoplasty need to be personalized according to the patient's condition and intraoperative states. Other factors in the actual situation may also lead to unsatisfactory postoperative hearing recovery, such as extensive lesion destruction, congenital eustachian tube dysfunction, poor middle ear ventilation or postoperative ossicle displacement. Early use of hearing aids should be considered in children with poor hearing in both ears (moderate or higher hearing loss) after stabilization of the ear condition after surgery.
The high recurrence rate of the surgeries (7/24, 29.2%) shown in this study may be related to the presence of certain risk factors in these children. In this study, the recurrence time was 0.8‒3-years after surgery and the longest follow-up was 9-years. About the postoperative follow-up, International Pediatric Oncology Group (IPOG) guidelines18 recommend a minimum of 5-years. Most of the children had no interruption in follow-up. We recommend that children with BMEC be followed-up for more than 5-years or even for life. Based on our experience, we summarized a treatment flow chart for BMECs (Fig. 3).Fig. 3. Flow chart of clinical treatment for BMEC in children. BMEC: bilateral middle ear cholesteatoma.Fig. 3
Conclusion
In our cohort, BMEC presented at a significantly younger age and exhibited a high prevalence of concomitant palatal cleft anomalies or occult submucous cleft palates, necessitating particular clinical vigilance in this pediatric population. A staged bilateral surgical intervention was prioritized in most cases, with the more symptomatic ear addressed first. Furthermore, given the elevated recurrence risk in these patients, long-term follow-up surveillance is imperative.
ORCID ID
Xiaoxu Wang: 0000-0002-2329-8730
Lining Guo: 0000-0002-3660-4864
Enxia Tian: 0009-0002-7199-5394
Min Chen: 0000-0001-8935-5606
Wei Liu: 0000-0002-1927-5499
Xin Ni: 0000-0003-0857-8512
Jie Zhang: 0000-0002-1621-7779
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Declaration of competing interest
The authors declare no have conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yung M.Tono T.Olszewska E.EAONO/JOS Joint Consensus Statements on the Definitions, Classification and Staging of Middle Ear Cholesteatoma J Int Adv Otol.132017182805905610.5152/iao.2017.3363 · doi ↗ · pubmed ↗
- 2Tos M.Incidence, etiology and pathogenesis of cholesteatoma in children Adv Otorhinolaryngol.401988110117338922310.1159/000415679 · doi ↗ · pubmed ↗
- 3Kemppainen H.O.Puhakka H.J.Laippala P.J.SipiläM.M.Manninen M.P.Karma P.H.Epidemiology and aetiology of middle ear cholesteatoma Acta Otolaryngol.11919995685721047859710.1080/00016489950180801 · doi ↗ · pubmed ↗
- 4Rosito L.P.S.Silva M.N.L.Selaimen F.A.Characteristics of 419 patients with acquired middle ear cholesteatoma Braz J Otorhinolaryngol.83220171261312723663310.1016/j.bjorl.2016.02.013PMC 9442758 · doi ↗ · pubmed ↗
- 5Hong J.P.Kim M.B.Symmetric bilateral congenital middle ear cholesteatoma: a case report J Audiol Otol.27202345503540506310.7874/jao.2022.00031 PMC 9884991 · doi ↗ · pubmed ↗
- 6Lee C.H.Kim M.K.Kim H.M.Won C.Shin T.H.Kim S.Y.Bilateral congenital cholesteatoma Otol Neurotol.392018 e 336e 3412964905310.1097/MAO.0000000000001803 · doi ↗ · pubmed ↗
- 7Marchioni D.Rubini A.Gonzalez-Navarro M.Alicandri-Ciufelli M.James A.Presutti L.Bilateral congenital cholesteatoma: surgical treatment and considerations Int J Pediatr Otorhinolaryngol.9920171461512868855810.1016/j.ijporl.2017.06.006 · doi ↗ · pubmed ↗
- 8Rohlfing M.L.Sukys J.M.Poe D.Grundfast K.M.Bilateral congenital cholesteatoma: a case report and review of the literature Int J Pediatr Otorhinolaryngol.107201825302950130610.1016/j.ijporl.2018.01.013 · doi ↗ · pubmed ↗